
REVIEW ARTICLE
TELEHEALTH INTERVENTION EFFECTIVENESS AND ITS IMPACT ON PEOPLE WITH RHEUMATOID ARTHRITIS: AN UMBRELLA REVIEW*
Ana Almeida Ribeiro1, Mauro Mota2, Mauro Coelho3, Maria Adriana Henriques3, Madalena Cunha2
1 University of Lisbon; Lisbon School of Nursing; Jean Piaget School of Health Sciences of Viseu. Portugal
2 Polytechnic Institute of Viseu; Viseu School of Health Sciences. Portugal
3 Lisbon School of Nursing. Portugal
ABSTRACT
Objective: To provide a rigorous synthesis drawing on available evidence from systematic reviews assessing telehealth interventions for individuals with rheumatoid arthritis. Method: This umbrella review was conducted following the Joanna Briggs Institute methodology and centers on adults diagnosed with rheumatoid arthritis according to ACR/EULAR criteria. All telehealth modalities were included, following the definition set by the WHO in 2016. Multiple databases were consulted, ensuring rigorous study selection and validation. Results: Telehealth interventions show promise for rheumatoid arthritis self-management, with effectiveness similar to that seen in other chronic conditions. However, some barriers were observed, such as challenges in using technology, heterogeneity in study approaches, and limitations in platform usability. Even so, the results indicated significant improvements across multiple domains, such as physical activity, functional capacity, and medication adherence, in line with prior research. The heterogeneity found across studies indicates the need for more robust future investigations. Conclusion: Telehealth interventions show potential for managing rheumatoid arthritis, offering a safe and effective alternative to support individuals with this condition. It is essential to address the identified challenges by enhancing tool usability and specificity, and by promoting rigorous research that substantiates its long-term effectiveness.
Descriptors: Telehealth; Rheumatoid Arthritis; Self-Management.
|
How to cite: Ribeiro AA, Mota M, Coelho M, Henriques MA, Cunha M. Telehealth intervention effectiveness and its impact on people with rheumatoid arthritis: an umbrella review. Online Braz J Nurs. 2025;24:e20256913. https://doi.org/10.17665/1676-4285.20256913 |
INTRODUCTION
As outlined by the World Health Organization (WHO) in 2022, telehealth has the potential to democratize healthcare access by overcoming geographical barriers and facilitating continuous management, particularly for individuals with rheumatoid arthritis (RA), regardless of their location(1). In Portugal’s current resource-limited context, telehealth’s relevance is particularly evident. Both patients with RA and healthcare providers have benefited from this approach, ensuring care continuity and notable health gains.
However, integrating telehealth into clinical practice for people with RA poses several challenges. Regularly monitoring disease activity and functional status is essential for effective RA management, while transitioning to a virtual environment can present various logistical challenges(2). While teleconsultations enhance accessibility, especially in remote regions, their effectiveness may be limited in situations requiring physical examinations, which are frequent in rheumatology. This transition demands careful consideration, robust infrastructure, and ongoing patient training(3-4).
Renowned organizations, such as the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR), have provided guidelines on integrating telehealth into RA clinical care. While the ACR focused on adapting assessment metrics for virtual contexts(2), the EULAR proposed principles aimed at balancing remote and in-person care, promoting shared decision-making, interdisciplinary collaboration, and adequate training for healthcare professionals(5).
Studies consistently show high patient satisfaction with telehealth interventions, driven by better access to specialists and improved cost-effectiveness(4). However, previous research, such as studies by McDougall et al. and Piga et al., reported mixed results regarding telehealth effectiveness in people with RA(6-7). This heterogeneity underscores the need for an umbrella review designed to deliver a more holistic and systematic analysis covering the available literature.
Even though telehealth was introduced in rheumatology in the 1990s, its application has evolved over time, particularly in expanding care to remote areas(4,8). A preliminary search in reputable databases such as the Joanna Briggs Institute (JBI) Database of Systematic Reviews and Implementation Reports, the Cochrane Database of Systematic Reviews, the International Prospective Register of Systematic Reviews (PROSPERO), the Medical Literature Analysis and Retrieval System Online (MEDLINE) and the Cumulated Index in Nursing and Allied Health Literature (CINAHL), revealed no umbrella reviews directly addressing the research question. Consequently, this review seeks to present a rigorous synthesis drawing on available evidence from systematic reviews evaluating telehealth interventions in people with RA.
Considering the topic’s relevance and aiming for comprehensive understanding, two main questions were formulated: the first examines the effectiveness of telehealth interventions, evaluating pain, functional impairment, fatigue, and both emotional and physical well-being in individuals diagnosed with RA. Simultaneously, the second question seeks to clarify how these interventions can mitigate the overall disease impact while improving the quality of life of affected patients.
METHOD
This systematic review was meticulously conducted following the JBI methodology for umbrella reviews(9).
The review question was developed based on the PICO mnemonic (Population, Intervention, Comparison, Outcome), frequently used in systematic reviews assessing clinical intervention effectiveness. The guiding question was as follows: How do telehealth interventions influence clinical and functional outcomes in adults with rheumatoid arthritis compared with conventional care?
To ensure data integrity and relevance, strict criteria were established to select participants and studies. Regarding participant selection, the review targeted adults with RA diagnoses confirmed by ACR/EULAR criteria. As for the interventions, an inclusive approach was taken, encompassing all telehealth modalities fitting the WHO definition from 2016(11).
A meticulous review strategy was implemented to ensure comprehensive and robust data collection. The following databases were additionally consulted to broaden research scope: PubMed Central, Scopus, Epistemonikos, PsycINFO, Excerpta Medica Database (Embase), Physiotherapy Evidence Database (PEDro), Campbell Collaboration Library of Systematic Reviews, Repositório Científico de Acesso Aberto de Portugal (RCAPP), among others. Each result emerging from this exhaustive search was independently scrutinized by two independent researchers, who based their decisions on predefined criteria.
Data collection was carried out between January 10 and February 25, 2024. Controlled descriptors and free terms, such as 'rheumatoid arthritis', 'telemedicine', 'telehealth', 'digital health', 'self-management' were used, combined with the Boolean operators AND/OR.
Selected studies’ integrity and relevance were subsequently validated using the JBI Critical Appraisal Checklist for Systematic Reviews and Research Synthesis tool. All relevant data were extracted using the bibliographic reference management software ENDNOTE 20. Data accuracy was ensured through collaboration between two researchers, making a third evaluator unnecessary owing to their consensus.
In conclusion, all collected data were meticulously detailed and systematically organized, culminating in a synthesis that highlights the main findings and offers evidence-based recommendations on the topic.
RESULTS
The literature reports telehealth interventions in RA management. Strict inclusion criteria were applied, yielding a limited, well-defined study selection.
A total of 262 records were identified, 217 from bibliometric databases and 45 from grey literature. After excluding 20 duplicates, 234 studies were discarded based on title and abstract relevance. Among the 8 remaining studies, 6 were excluded for failing to meet at least one eligibility criterion: participants, interventions, outcomes, or study design. Figure 1 presents a flowchart illustrating the detailed selection process.
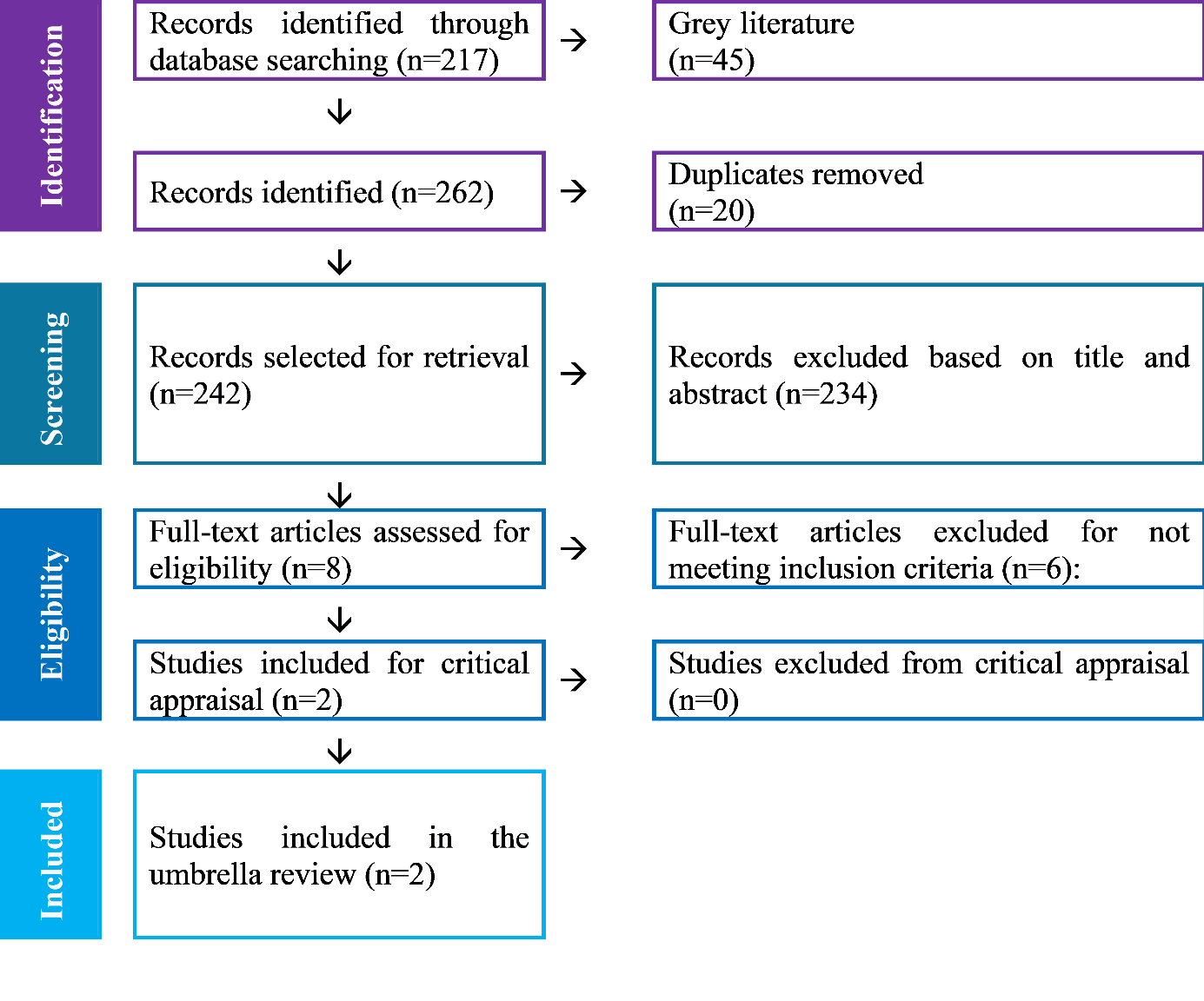
Figure 1 - Flowchart illustrating the study selection process (PRISMA). Viseu, Portugal, 2024
The researchers reached robust agreement(11) and reached consensus without requiring a third party. No authors were contacted for additional information.
According to the JBI checklist, one review achieved a high-quality rating (score: 10), while the other was rated moderate quality (score: 9). All studies included in the review fulfilled the predefined inclusion criteria. Publication bias was assessed in both reviews, and no study was excluded due to quality concerns.
A total of 11 Randomized Controlled Trials (RCTs) were included from the two reviews, but only 10 were deemed relevant due to duplication. The total number of participants was 1,358. Given the clinical heterogeneity, a meta-analysis was not conducted.
Participants’ average age ranged between 49 and 69.3 years, and disease duration varied from 6 months to 11.89 years. Two RCTs did not assess the latter. Most participants were female, with percentages ranging from 29% to 95% across 4 RCTs. Gender information was unavailable for the remaining studies.
The RCTs were conducted in countries such as China, the United States of America (USA), Finland, Italy, the Netherlands, and Switzerland. The reviews covered the period from 2010 to 2021, while the RCTs spanned 2006 to 2021. A growing interest in this topic is evident, with 6 RCTs conducted after 2019.
Figure 2 presents further details on the systematic reviews.
|
|
Srikesavan, Bryer, Ali and Williamson (2019) |
Alison Maclver, Hannah Hollinger, Clare Carolan (2021) |
|
Study Details |
||
|
Year |
2019 |
2021 |
|
Objectives |
To assess the impact of online rehabilitation interventions on factors such as pain, functional capacity, quality of life, self-efficacy, RA-related knowledge, physical activity, and adverse effects in adults with RA. |
To synthesize and assess telehealth interventions’ effectiveness in RA self-management. |
|
Participants (characteristics / total number) |
Adults (+18y/o), diagnosed with RA. Trials reporting mixed data from different arthritis types were excluded.
|
Inclusion Criteria:
Participants:
|
|
Context |
Both passive control groups (waiting list or no treatment) and active control groups (usual treatment or other online intervention) were included. |
Each study compared telehealth interventions to standard care. |
|
Intervention description/ key topics under investigation |
Allam et al, 2015: A website offering educational content, social support, and games. Van den Berg et al, 2006: A physical activity program featuring remote monitoring, quarterly meetings, forums, and self-management strategies. Lorig et al, 2008: A self-management program featuring tailored exercises, cognitive techniques, noticeboards, monitoring tools, and an online forum. Shigaki et al, 2013: RA Help.org – A structured program aimed at improving RA self-efficacy and management, featuring educational modules, task lists, a resource library, self-monitoring tools, telephone support, and online community activities. |
Allam et al, 2015: A website offering educational content, social support, and games. Zuidema et al, 2019: 12-month access to an online self-management program with nine modules and a symptom diary. Kussalo et al, 2020: A text-message–based system designed for self-monitoring RA symptoms. Song et al, 2019: Four nurse-led, telephone-based educational sessions delivered post-discharge. Liu et al, 2020: Post-discharge telephone-based educational sessions. Zhao & Chen, 2019: Post-discharge, telephone-based educational sessions addressing exercise, diet, and medication. Salafti et al, 2016: A web platform for symptom monitoring and information access under clinical supervision. |
|
Research Details |
||
|
Databases searched for relevant studies |
|
|
|
Study period for included studies |
2006 – 2015 |
2014 – 2021 |
|
Number of included studies |
Total: 4 RCTs
|
7 articles (RCTs) |
|
Study types included |
RCTs published in English in peer-reviewed journals. |
Randomized Controlled Trials (RCTs) |
|
Countries represented in included studies |
|
|
|
Assessment |
||
|
Tools employed for bias assessment |
Cochrane risk-of-bias assessment tool |
Cochrane risk-of-bias assessment tool |
|
Assessment rating |
High risk for all 4 included studies |
|
|
Analysis |
||
|
Analytical methodology |
Narrative synthesis |
Narrative synthesis |
|
Results obtained |
|
|
|
Outcomes/Findings |
Online rehabilitation interventions led to significant improvements solely in self-efficacy and RA-related knowledge. |
Intervention components, theoretical frameworks, and measured outcomes varied considerably. Five RCTs reported improvements in disease activity, medication adherence, physical activity, and self-efficacy levels. |
|
Significance/direction |
Clinical outcomes could not be firmly established because evidence quality was low, and potential adverse effects of online interventions were not examined. Selection bias and insufficient blinding further weakened confidence in the findings. |
Studies ranged from low to moderate quality, which affected validity, reliability, and generalizability. |
|
Heterogeneity |
Clinical heterogeneity arose due to differences in participants, interventions, and measured outcomes among groups. |
Clinical heterogeneity arose due to differences in participants, interventions, and measured outcomes among groups. |
|
Comments / Conclusions |
While online interventions for RA demonstrate significant potential, existing evidence indicates limited development and insufficient evaluation. Future research should prioritize patient-centered designs and long-term follow-up. |
Well-structured, tailored telehealth interventions can produce positive outcomes in RA self-management. |
Figure 1 - Study characteristics and methodological details reported in systematic reviews. Viseu, Portugal, 2024
Systematic reviews evaluated telehealth interventions, encompassing online management programs and telephone-based support, and their impact on multiple RA-related outcomes.
The first review focused on evaluating how online rehabilitation interventions affected adults with RA. Assessed effects included pain, functional capacity, quality of life, self-efficacy, RA-related knowledge, physical activity, and potential adverse effects. Among the reviewed interventions, two were online self-management programs: one provided guidance, social support, and interactive games, while the other offered a physical training plan with weekly email follow-ups. A third intervention included an online discussion forum with self-assessment tools, while a fourth combined online activities with weekly telephone-based support(12).
MacIver et al., in turn, evaluated and synthesized evidence on telehealth intervention effectiveness, identifying three online approaches and two delivered via telephone. These interventions were grounded in educational and behavioral theories, promoting self-management and providing education and information about RA. It is worth noting that, in many cases, supervision was provided by healthcare professionals, and treatment duration across the reviews ranged from 6 to 52 weeks(13).
Two outcome types, primary and secondar, are distinguished in the reviews. Primary outcomes carry the greatest weight and comprise functional capacity, quality of life, medication adherence, physical activity, and healthcare use. Secondary outcomes include additional indicators such as efficacy and safety, and in this study comprised disease activity, pain, fatigue, RA-related knowledge, empowerment, and self-efficacy levels.
Disease activity
This metric was assessed in five clinical trials included in a systematic review. No statistically significant results were observed in four studies. One RCT, however, demonstrated notable benefits through an online program enabling RA patients to monitor symptoms and receive personalized treatment adjustments. In this study, the intervention group outperformed the control group regarding disease remission, time to reach remission, and functional performance(13).
Pain
Three studies examined pain. Two, which focused on online self-management, did not report significant effects on pain. A third study, incorporating a more comprehensive online program, also failed to demonstrate meaningful improvements(12-13).
Fatigue
Fatigue was examined in a study using an online self-management program, which revealed no significant differences between intervention and control groups(13).
Functional capacity
Studies focusing on online self-management showed mixed results. While one study did not yield significant improvements, another implementing telephone-based education demonstrated improvements by week 8(12-13).
Quality of life
This aspect, examined in two online physical activity programs, revealed slight improvements in the intervention group at medium- and long-term follow-ups. A third study reported significant improvements after twelve months(12-13).
RA-related knowledge
Online self-management studies demonstrated increased disease-related knowledge in intervention groups for certain comparisons(12-13).
Empowerment
This aspect, examined in an online self-management study, showed improved scores in RA patients who received social support and participated in game-based activities(13).
Self-efficacy
Significant improvements were observed in intervention groups across short-, medium-, and long-term follow-ups with online self-management programs or telephone-based education(12-13).
Physical activity
Some groups showed increased physical activity, while others did not demonstrate consistent improvements(12-13).
Medication adherence
Regarding medication adherence, studies on online and telephone-based self-management showed varied outcomes(12-13).
Healthcare use
A decrease in medical visits was noted in some groups, but findings were not consistent across all studies. One study specifically reported lower hospital readmission rates in the intervention group(13).
The review identified two types of telehealth interventions: online self-management programs and telephone- or text-based programs.
Online self-management programs were beneficial for physical activity, healthcare use, and empowerment (moderate evidence), as well as for quality of life, RA-related knowledge, self-efficacy, and disease activity (low evidence). However, no meaningful effects were observed on functional capacity, medication adherence, or fatigue, with evidence certainty rated as very low.
Telephone- or text-based interventions, in turn, produced meaningful improvements, showing beneficial effects on functional capacity, medication adherence, and self-efficacy, all supported by moderate evidence, whereas no consistent changes were observed in healthcare use.
Findings on pain and fatigue were mostly inconsistent and showed no clinically relevant effects. Evidence for each aspect is summarized in Figure 3.
|
Interventions |
Impact |
No. of Participants |
Evidence certainty (level) / Justification |
|
Online self-management programs |
|||
|
Functional capacity |
No significant difference was observed compared with the control group treatment. |
345 (based on 2 reviews) |
very low
|
|
Quality of life |
**Meaningful improvement with minor beneficial effects. |
474 (based on 2 reviews) |
low
|
|
Medication adherence |
No significant difference was observed compared with the control group treatment. |
157 (based on 2 reviews) |
very low
|
|
Physical activity |
*Meaningful improvement with substantial beneficial effects. |
317 (based on 2 reviews) |
moderate
|
|
Healthcare use |
*Meaningful improvement with substantial beneficial effects. |
198 (based on 2 reviews) |
moderate
|
|
Disease activity |
**Meaningful improvement with minor beneficial effects. |
157 (based on 1 review) |
low
|
|
Pain |
**Meaningful improvement with minor beneficial effects |
461 (based on 2 reviews) |
low
|
|
Fatigue |
No significant difference was observed compared with the control group treatment |
157 (based on 1 review) |
very low
|
|
RA-related knowledge |
**Meaningful improvement with minor beneficial effects |
157 (based on 2 reviews) |
low
|
|
Empowerment |
*Meaningful improvement with substantial beneficial effects. |
157 (based on 2 reviews) |
moderate
|
|
Self-efficacy |
**Meaningful improvement with minor beneficial effects |
458 (based on 2 reviews) |
low
|
|
Telephone- / text-based self-management programs |
|||
|
Functional capacity |
*Meaningful improvement with substantial beneficial effects. |
180 (based on 1 review) |
moderate
|
|
Medication adherence |
*Meaningful improvement with substantial beneficial effects. |
92 (based on 1 review) |
moderate
|
|
Healthcare use |
No significant difference was observed compared with the control group treatment |
254 (based on 1 review) |
very low
|
|
Self-efficacy |
*Meaningful improvement with substantial beneficial effects. |
286 (based on 2 reviews) |
moderate
|
|
We defined *meaningful improvement with substantial beneficial effects when p<0.05. We defined **meaningful improvement with minor beneficial effects when significance was not assessed or p>0.05 |
|||
|
Evidence levels according to the GRADE Working Group High certainty: We have strong confidence that the true effect lies near the estimated effect. Moderate certainty: Confidence in the estimated effect is moderate, meaning the true effect is probably near the estimated effect, but notable differences cannot be ruled out. Low certainty: Confidence in the effect estimate is limited; the true effect may differ substantially from the estimated effect. Very low certainty: The true effect is likely to differ considerably from the estimated effect due to minimal confidence. |
|||
Figure 2 - Evidence summary. Viseu, Portugal, 2024
DISCUSSION
As a chronic and disabling disease, rheumatoid arthritis has experienced a notable shift in management approaches. In recent years, advances in therapies, coupled with increasing digitalization in healthcare, have made a proactive approach to RA self-management increasingly essential. In this context, telehealth stands out as a crucial tool.
This umbrella review synthesizes data from two systematic reviews, covering 10 clinical trials, and provides insights into telehealth intervention efficacy in patients with RA. These findings, suggesting promising efficacy, corroborate earlier research on chronic conditions reported by Thurah et al., Neubeck et al. e So e Chung(14-16).
Other areas where telehealth has been applied, such as diabetes, cardiovascular disease, and mental health, have shown consistently positive effects. This comparison suggests that the telehealth impact in patients with RA may be enhanced through more personalized and interactive approaches.
Nonetheless, certain barriers were identified. Two studies, conducted by Stellefson et al. and Van den Berg et al., reported that participants sometimes faced difficulties using telehealth platforms(17-18). This challenge highlights the need for more intuitive tools developed with user input, as advocated by Rogers et al. and Tuckson et al.(19-20).
Although studies and outcomes were heterogeneous, the findings show consistent gains in physical activity, empowerment, and functional capacity. More encouragingly, no telehealth intervention proved harmful, positioning this modality as a safe alternative to conventional treatment and management approaches.
These studies were carried out in countries with generally high digital literacy, including the United States, China, Italy, Switzerland, Finland, and the Netherlands. As a result, these findings might not generalize to environments with fewer technological and structural resources.
Even so, additional limitations must be considered. Variability across studies, alongside quality and bias issues, underscores the necessity for more rigorous investigations in the future. Heterogeneity notably constrained the potential for in-depth data analysis.
Overall, the findings highlight telehealth as a valuable tool in RA management. Nonetheless, subsequent research should investigate these interventions more thoroughly, emphasizing their long-term effectiveness and safety.
CONCLUSION
The RA has been shaped over the years by therapeutic and methodological advances, placing greater emphasis on proactive and personalized disease management. In this evolving landscape, telehealth emerges as a valuable tool whose interventions, although promising, still require further scrutiny and refinement.
The collected data highlight telehealth’s potential to enhance multiple aspects of RA treatment and management, from physical activity to functional capacity. This potential, supported by earlier investigations such as those by Thurah et al. e Neubeck et al., shows that telehealth can serve as a safe and effective way to support individuals living with RA.
However, the barriers identified, particularly those related to tool usability and study heterogeneity, raise interesting hypotheses. Telehealth effectiveness in RA patients may be optimized through tools co-designed with individuals living with the condition, ensuring both user-friendliness and disease-specific relevance. Findings from Stellefson et al. e Van den Berg et al. support this hypothesis, highlighting the need for further investigation.
Global disparities in digital infrastructure, technological readiness, and healthcare systems limit the generalizability of these findings, underscoring the need for context-adapted telehealth approaches.
There is a clear need for larger, high-quality studies that both confirm telehealth benefits and elucidate its inherent limitations. Long-term, large-scale longitudinal studies could provide insights into both sustained effects and the broader applicability of these interventions.
In summary, telehealth in the RA context stands out as a valuable and innovative alternative. However, its integration must be pursued in an informed, sustained, and critical way, always keeping patient well-being central to clinical decisions. Continued research in this field is not only advisable but essential, ensuring that telehealth fulfills its promise to reshape RA treatment.
*Article extracted from the doctoral thesis entitled “Desenvolvimento e viabilidade de uma intervenção eNURSING em pessoas com artrite reumatóide: continuidade de cuidados” [Development and feasibility of an eNURSING intervention in people with rheumatoid arthritis: continuity of care], presented to the Doctoral Program in Nursing, University of Lisbon, Lisbon, Portugal, in 2023.
ACKNOWLEDGMENTS
The authors express their gratitude to the Health Sciences Research Unit: Nursing (UICISA:E) for their support and collaboration throughout the development of this work, which contributed substantially to its scientific quality and methodological rigor.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
REFERENCES
1. World Health Organization. Consolidated telemedicine implementation guide [Internet]. Geneva: World Health Organization; 2022 [cited 2024 Jan 02]. Available from: https://www.who.int/publications/i/item/9789240059184
2. England BR, Barber CEH, Bergman M, Ranganath VK, Suter LG, Michaud K. Adaptation of American College of Rheumatology Rheumatoid Arthritis Disease Activity and Functional Status Measures for Telehealth Visits. Arthritis Care Res (Hoboken). 2021;73(12):1809-1814. https://doi.org/10.1002/acr.24429
3. Fernandes AL, Silva C, Miranda LC. Management of Rheumatic Diseases during the COVID-19 Pandemic: Beyond Telehealth Services. Acta Med Port. 2020;33(10):706. https://doi.org/10.20344/amp.14556
4. Oh Y, Hennessey A, Young L, Barrett C. Evaluation of patient satisfaction for telehealth (telephone and video) in rheumatology outpatients during COVID‐19 pandemic. Intern Med J. 2022;52(4):559-565. https://doi.org/10.1111/imj.15663
5. Thurah Ad, Marques A, Souza Sd, Crowson CS, Myasoedova E. Future challenges in rheumatology – is telemedicine the solution? Ther Adv Musculoskelet Dis. 2022;14:1-12. https://doi.org/10.1177/1759720X221081638
6. McDougall JA, Ferucci ED, Glover J, Fraenkel L. Telerheumatology: A Systematic Review. Arthritis Care Res (Hoboken). 2017;69(10):1546-1557. https://doi.org/10.1002/acr.23153
7. Piga M, Cangemi I, Mathieu A, Cauli A. Telemedicine for patients with rheumatic diseases: Systematic review and proposal for research agenda. Semin Arthritis Rheum. 2017;47(1):121-128. https://doi.org/10.1016/j.semarthrit.2017.03.014
8. Ahmed S, Grainger R, Santosa A, Adnan A, Alnaqbi KA, Chen Y-H, et al. APLAR recommendations on the practice of telemedicine in rheumatology. Int J Rheum Dis. 2022;25(3):247-258. https://doi.org/10.1111/1756-185X.14286
9. Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141-146. https://doi.org/10.1097/xeb.0000000000000050
10. World Health Organization. Global diffusion of eHealth: making universal health coverage achievable: report of the third global survey on eHealth [Internet]. Geneva: World Health Organization; 2016 [cited 2024 Jan 02]. Available from: https://apps.who.int/iris/handle/10665/252529
11. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276-282. https://doi.org/10.11613/BM.2012.031
12. Srikesavan C, Bryer C, Ali U, Williamson E. Web-based rehabilitation interventions for people with rheumatoid arthritis: A systematic review. J Telemed Telecare. 2019;25(5):263-275. https://doi.org/10.1177/1357633x18768400 [included in the review]
13. MacIver A, Hollinger H, Carolan C. Tele-health interventions to support self-management in adults with rheumatoid arthritis: a systematic review. Rheumatol Int. 2021;41(8):1399-1418. https://doi.org/10.1007/s00296-021-04907-2 [included in the review]
14. Neubeck L, Redfern J, Fernandez R, Briffa T, Bauman A, Freedman SB. Telehealth interventions for the secondary prevention of coronary heart disease: a systematic review. Eur J Cardiovasc Prev Rehabil. 2009;16(3):281-289. https://doi.org/10.1097/HJR.0b013e32832a4e7a
15. So CF, Chung JW. Telehealth for diabetes self-management in primary healthcare: A systematic review and meta-analysis. J Telemed Telecare. 2018;24(5):356-364. https://doi.org/10.1177/1357633x17700552
16. Thurah A de, Bremander A, Primdahl J. High-quality RMD rehabilitation and telehealth: Evidence and clinical practice. Best Pract Res Clin Rheumatol. 2020;34(2):101513. https://doi.org/10.1016/j.berh.2020.101513
17. Stellefson M, Chaney B, Barry AE, Chavarria E, Tennant B, Walsh-Childers K, et al. Web 2.0 chronic disease self-management for older adults: a systematic review. J Med Internet Res. 2013;15(2):e35. https://doi.org/10.2196/jmir.2439
18. van den Berg MH, Ronday HK, Peeters AJ, Voogt-van der Harst EM, Munneke M, Breedveld FC, et al. Engagement and satisfaction with an Internet-based physical activity intervention in patients with rheumatoid arthritis. Rheumatology (Oxford). 2007;46(3):545-552. https://doi.org/10.1093/rheumatology/kel341
19. Tuckson RV, Edmunds M, Hodgkins ML. Telehealth. N Engl J Med. 2017;377(16):1585-1592. https://doi.org/10.1056/NEJMsr1503323
20. Rogers MA, Lemmen K, Kramer R, Mann J, Chopra V. Internet-Delivered Health Interventions That Work: Systematic Review of Meta-Analyses and Evaluation of Website Availability. J Med Internet Res. 2017;19(3):e90. https://doi.org/10.2196/jmir.7111
Submission: 09-Apr-2024
Approved: 19-May-2025
Editors:
Rosimere Ferreira Santana (ORCID: 0000-0002-4593-3715)
Geilsa Soraia Cavalcanti Valente (ORCID: 0000-0003-4488-4912)
Érica Brandão de Moraes (ORCID: 0000-0003-3052-158X)
Corresponding author: Ana Almeida Ribeiro (anaalmeidaribeiro@hotmail.com)
Publisher:
Escola de Enfermagem Aurora de Afonso Costa – UFF
Rua Dr. Celestino, 74 – Centro, CEP: 24020-091 – Niterói, RJ, Brazil
Journal email: objn.cme@id.uff.br
|
AUTHORSHIP CONTRIBUTIONS |
|
Study conception: Ribeiro AA. Data acquisition: Ribeiro AA. Data analysis and interpretation: Ribeiro AA, Mota M, Coelho M, Cunha M. Textual writing and/or critical review of intellectual content: Ribeiro AA. Final approval of the text to be published: Ribeiro AA, Mota M, Coelho M, Henriques MA, Cunha M. Responsibility for the text and for guaranteeing the accuracy and integrity of any part of the work: Ribeiro AA, Cunha M. |
