
ORIGINAL ARTICLE
NURSING DIAGNOSES IN OLDER ADULTS WITH COVID-19 ON INVASIVE MECHANICAL VENTILATION: A LONGITUDINAL STUDY
Isadora Barreira Queiroz1, Erika Silva de Sá2, Ricardo Costa da Silva3, Agueda Maria Ruiz Zimmer Cavalcante4
1 Federal University of Goiás, College of Nursing. Goiânia, Goiás, Brazil. ORCID: 0000-0002-3516-1280. E-mail: isadorabarreiraq@gmail.com
2 Federal University of Goiás. Graduate Program in Nursing and Health. Goiânia, Goiás, Brazil. ORCID: 0000-0002-3026-6091. E-mail: erikadesa@mail.uft.edu.br
3 State University of Goiás, Ceres University Unit, Nursing Course. Ceres, Goiás, Brazil. ORCID: 0000-0002-1355-5262. E-mail: ricardo@ueg.br
4 Federal University of Goiás. Graduate Program in Nursing and Health. Goiânia, Goiás, Brazil. ORCID: 0000-0003-3910-2162. E-mail: aguedacavalcante@ufg.br
ABSTRACT
Objective: To identify the NANDA International Nursing Diagnoses (ND) in older adults in intensive care for COVID-19 who required invasive mechanical ventilation support. Methods: A longitudinal observational study, based on the retrospective analysis of nursing records from 41 patient charts at three distinct moments: upon admission to the intensive care unit, 24 hours after orotracheal intubation, and at the moment before the outcome (discharge, death, or extubation). Odds ratios were calculated. The manuscript was guided by the STROBE statement. Results: With an average hospitalization time of 17 days, 127 NDs were identified at admission, 133 NDs 24 hours after intubation, and 159 NDs before the outcome. "Risk for Infection" had the highest frequency throughout hospitalization (53.7%, 75.6%, and 87.8%), while the diagnosis of "Anxiety" showed the largest negative variation (-240%). While "Anxiety" increased the odds of "Ineffective Airway Clearance" (7.5 times) and "Ineffective Breathing Pattern" (27.7 times), "Ineffective Breathing Pattern", in turn, was associated with "Risk for Impaired Skin Integrity" (59 times). Conclusions: Different NDs were identified throughout the hospitalization of the older adults, with great variability in frequencies, depending on the clinical moment evaluated.
Descriptors: COVID-19; Nursing Diagnosis; Nursing Care for Hospitalized Elderly; Nursing Process; Artificial Respiration.
|
How to cite: Queiroz IB, Sá ES, Silva RC, Cavalcante AMRZ. Nursing diagnoses in older adults with COVID-19 on invasive mechanical ventilation: a longitudinal study. Online Braz J Nurs. 2025;24(Suppl 2):e20256884. https://doi.org/10.17665/1676-4285.20256884 |
What is already known:
Older adults hospitalized in intensive care for COVID-19 have complex care demands.
Intensive care nurses use standardized language systems to express clinical-diagnostic judgment even in complex scenarios.
Nursing diagnoses in critically ill patients can vary in frequency and intensity depending on the moment of hospitalization.
What this article adds:
The diagnosis of Risk for infection is frequently observed before, during, and after orotracheal intubation of critically ill hospitalized older adults.
There are weaknesses in the diagnostic and clinical nursing assessment process that result in low-accuracy nursing diagnoses.
The odds ratio of certain nursing diagnoses depends on the moment of hospitalization, making actions to reduce the severity spectrum essential.
INTRODUCTION
The demand for critical care directed at the older adult population in the intensive care unit (ICU) has been expanding globally(1). In Brazil, to date, the average age of ICU admissions is 63 years, and more than 60% of hospitalizations are of older adults aged 60 years or older(2). This reality has altered the work process in the ICU, mainly because the older adult population, when compared to adults, often presents with greater clinical severity and requires more interventions, which, consequently, increase the nursing workload(3-4).
Recently, the global epidemic caused by the Sars-CoV-2 virus infection, called COVID-19, has added a layer of complexity to the care of the critically ill older adults, especially as this age group has been disproportionately affected, with higher rates of hospitalization and mortality(5-7). Furthermore, the presence of comorbidities common in older adults, such as arterial hypertension(8), diabetes(9), chronic respiratory diseases, and kidney disease(10), is a factor that significantly increases the risk for the critical development of this condition(11).
In these cases, the early use of Invasive Mechanical Ventilation (IMV) has proven to be an effective strategy for reducing mortality in patients with COVID-19 complications(12). In general, the clinical manifestations that demand the use of IMV are secondary to a succession of events that include pneumonia, acute respiratory distress syndrome, sepsis, or even multiple organ dysfunction(11). Consequently, the nursing care required to assist these critically ill patients is complex and demands a multidimensional clinical reasoning process, based on the multiplicity of human needs to be addressed(13).
As an ethical-legal requirement of the profession, reaffirmed by Resolution 736/2024 of the Brazilian Federal Nursing Council (14), the nursing process is a methodological model for the systematic performance of professional practice that favors the identification of care demands, even in scenarios of high clinical and therapeutic complexity, and provides support for care planning based on therapeutic prescription and the evaluation of achieved outcomes. Thus, for evidence-based practice and the effectiveness of nursing interventions, it is necessary to anchor clinical-diagnostic reasoning in structured mental models and Standardized Language Systems (SLS) as guides for practice(14-15).
Among the globally recognized classification systems for Nursing Diagnoses (ND), NANDA International (NANDA-I) is the nursing classification with the highest level of evidence and clinical research(16). In this classification, an ND is defined as a "clinical judgment concerning a human response to health conditions/life processes, or a vulnerability for that response, by an individual, family, group, or community"(17). In the ICU, such judgments closely reflect the specific concerns of the discipline, which can provide the first signs of patient deterioration(18). Thus, the prioritization of NDs, considering possible clinical evolutions, aids in the development of care plans with personalized nursing interventions, with a greater possibility of achieving cost-effective outcomes and risk reduction(19).
Studies using nursing SLS encourage their use by clinical nurses, contribute to the documentation and reliable recording of care in practice, and assist in the advancement of nursing science. Therefore, although different studies on ND have been developed in patients with COVID-19(13,20-21), there is still a gap in the evidence directed at older adults on IMV, especially regarding the evolution of human responses at different moments of the clinical spectrum, from the nursing perspective. Therefore, the objective of this study was to identify the NANDA-I classification NDs in older adults hospitalized for COVID-19 in the ICU who required IMV support.
METHOD
Study design, period, and location
This was an observational, longitudinal, and retrospective study, related to the macroproject "Clinical validation of the NOC outcome mechanical ventilation response in older adults with COVID-19", linked to the Federal University of Goiás. The manuscript was guided by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement(22).
The study was conducted using secondary data from the medical records of older adults admitted to an ICU of a university hospital in the central region of Brazil, a reference center for the treatment of COVID-19 during the initial phases of the pandemic. Hospitalizations that occurred from January 1 to December 31, 2021, were considered for data collection.
Population or sample; inclusion and exclusion criteria
The study population consisted of the medical records of older adults, aged 60 years or older, hospitalized in the ICU during the study period, with a confirmed diagnosis of COVID-19 by rapid tests, RT-PCR, or antigen testing, and who required invasive ventilatory support. Medical records with incomplete or illegible nursing records that made it impossible to verify the NDs identified at the three moments of interest for the study were excluded: at ICU admission, 24 hours after orotracheal intubation (OTI), and before the outcome (extubation or death). Figure 1 shows the sample selection flowchart of the analyzed medical records.
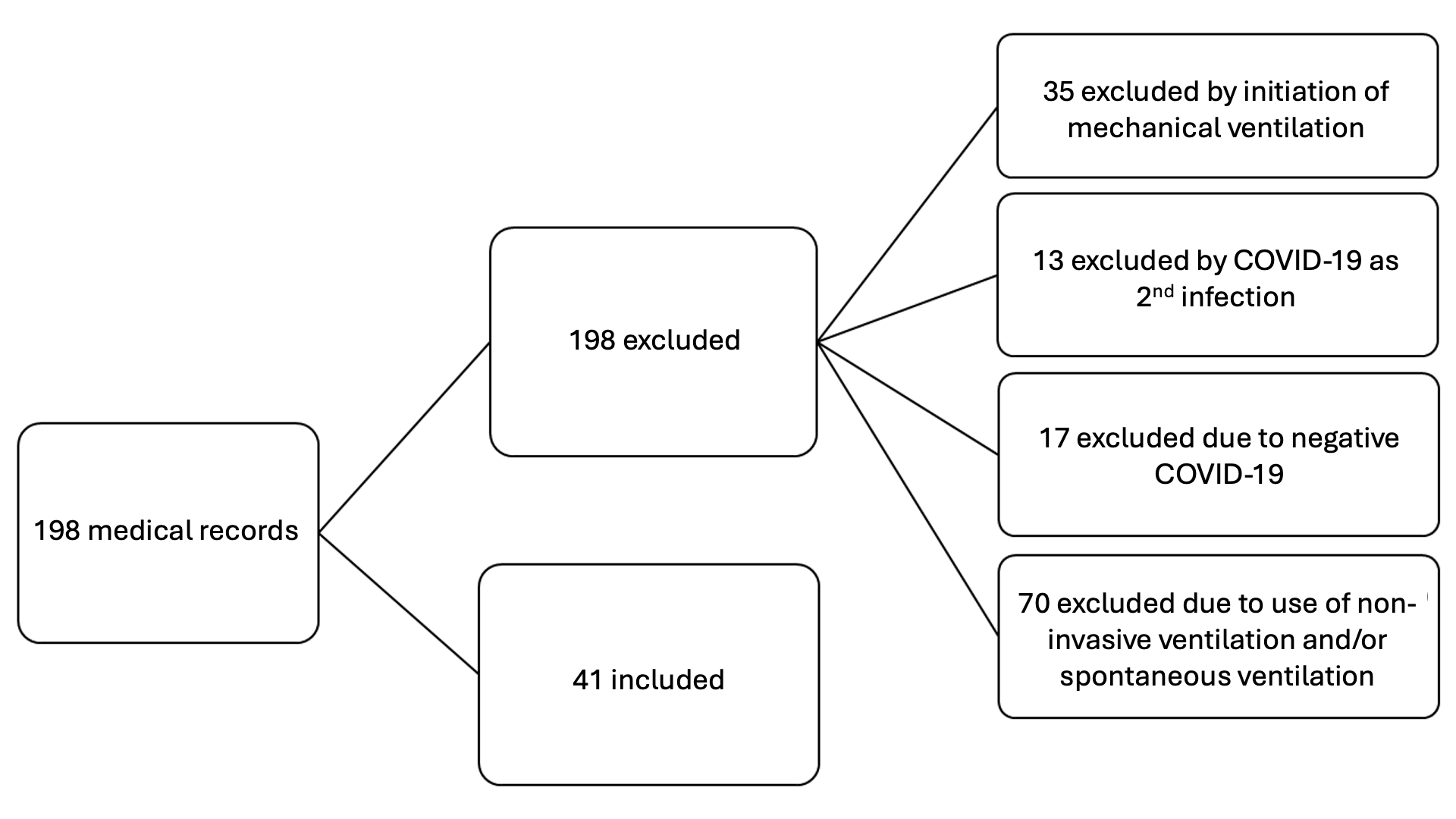
Source: research data, 2021.
Figure 1 – Flowchart of medical records selection of older adult patients hospitalized in the intensive care unit
Study protocol
Initially, in order to identify potential older adults who met the eligibility criteria, the hospital's Internal Regulation Nucleus (NIR) was asked for a list of patients who were admitted to the ICU for COVID-19 in the year 2021. With the list in hand, a screening was carried out to select the older adults and, with that, request each medical record from the institution's medical records service for data collection.
At the said institution, due to the health emergency, physical medical records were used, consisting of patient information (name, sex, age, race, origin, and occupation) and clinical information (medical diagnosis, comorbidities, length of stay, vital signs, fluid balance, neurological, respiratory, cardiovascular, gastrointestinal, skin and mucous membrane, and urinary assessments).
Regarding the NDs, there was a pre-selection in a checklist format of the most frequent ones in the unit, with their defining characteristics and related and/or risk factors as described by NANDA-I, which were selected if considered present based on the nurse's clinical-diagnostic judgment. It should be noted that, despite adopting the pre-selection format, there was space for the inclusion of new NDs in line with the patients' clinical presentation. The medical record also included a specific space for nursing evolutions and prescriptions. The data were collected using an instrument developed by the authors with the variables of interest: sociodemographic and clinical data, and the NDs identified by the nurses at each moment of the clinical evolution.
Analysis of results and statistics
The data were entered into Microsoft Excel spreadsheets and transferred to the statistical software IBM SPSS® version 25 and JAMOVI® version 1.6.23. Continuous variables were analyzed by measures of central tendency (mean and median) and dispersion (standard deviation and interquartile range); categorical variables were analyzed by relative and absolute frequency measures.
To test the normality of the data distribution, the Shapiro-Wilk test was applied, considering a fit to the normal distribution for p-values > 0.05. To verify the increase or decrease in the number of cases for each diagnosis, the coefficient of variation (CV) was calculated, considering the number of cases at the outcome and the number of cases at admission. To check for associations between the presence of NDs and clinical and sociodemographic variables, Fisher's exact test was applied, given the occurrence of frequencies lower than five. P-values ≤ 0.05 were considered significant.
The odds ratio (OR) was calculated by the quotient between the proportion of people who developed a certain ND concurrently with another already established ND and the proportion of individuals who did not develop that same diagnosis in the presence of the other. This measure was calculated to identify the extent to which the presence of one diagnosis increases the chances of another occurring during the moments of admission, after OTI, and at the outcome. To assess the statistical significance of the odds ratio, 95% confidence intervals were calculated, with those that did not include the null value of one being considered significant.
Ethical considerations
This study met the scientific requirements for research involving human beings and complied with the standards of Resolution 466/12 of the National Health Council. The main project was evaluated and approved by the Leide das Neves Ferreira Research Ethics Committee. In addition, the chart reviewers were trained and signed a data secrecy and confidentiality agreement.
RESULTS
Among the 41 medical records analyzed, it was observed that 22 (53.7%) of the older adults were male, identified as brown-skinned (53.6%), had incomplete elementary education (31.7%), were retired (60.9%), and had a mean age of 73 years (SD = 7.6). The mean length of hospitalization in the intensive care unit (ICU) was 17 days (SD = 8.4), with a minimum of 3 and a maximum of 39 days of admission. The main diagnostic method used for COVID-19 was RT-PCR (53.6%), and about 75% of the hospitalized patients had been immunized with at least one vaccine dose. Approximately 87% of older adults had a previous diagnosis of at least one comorbidity, the most frequent being arterial hypertension (56.1%) and diabetes mellitus (36.6%).
Table 1 presents the frequency of nursing diagnoses (ND) at each data collection point, as well as their variation throughout the three moments of clinical evolution, which could be positive (an increase in the presence of the ND) or negative (a reduction in frequency over time). The ND with the highest frequency at admission (53.7%) was "Risk for Infection", with an increase of almost 25% after orotracheal intubation (OTI) (75.6%), also rising before the patient's outcome (87.8%), representing a positive growth variation of 39% compared to admission.
Table 1 - Frequency and variation of nursing diagnoses in the three different assessment moments. Goiânia, GO, Brazil, 2021
|
Assessments |
||||||||
|
1st moment |
2nd moment |
3rd moment |
Total (N) |
Variation (%) |
||||
|
n |
(%) |
n |
(%) |
n |
(%) |
|||
|
Risk for infection |
22 |
31 |
75.6 |
36 |
87.8 |
89 |
||
|
Risk for falls |
11 |
26.8 |
15 |
36.6 |
18 |
43.9 |
44 |
39 |
|
Risk for impaired skin integrity |
10 |
24.4 |
12 |
29.3 |
16 |
39 |
38 |
38 |
|
Risco for unstable blood glucose |
12 |
29.3 |
13 |
31.7 |
12 |
29.3 |
37 |
0 |
|
Risk for constipation |
6 |
14.6 |
11 |
26.8 |
10 |
25 |
27 |
40 |
|
Anxiety |
17 |
41.5 |
4 |
9.8 |
5 |
12.2 |
26 |
-240 |
|
Risk for injury |
5 |
12.2 |
9 |
21.9 |
10 |
25 |
24 |
50 |
|
Ineffective breathing pattern |
6 |
14.6 |
6 |
14.6 |
10 |
25 |
22 |
40 |
|
Ineffective airway clearance |
5 |
12.2 |
6 |
14.6 |
9 |
21.9 |
20 |
44 |
|
Risk for contamination |
8 |
19.5 |
5 |
12.2 |
6 |
14.6 |
19 |
-33 |
|
Risk for bleeding |
5 |
12.2 |
4 |
9.8 |
8 |
19.5 |
17 |
38 |
|
Bathing self-care deficit |
4 |
9.8 |
4 |
9.8 |
7 |
17.7 |
15 |
43 |
|
Constipation |
5 |
12.2 |
6 |
14.6 |
4 |
9.77 |
15 |
-25 |
|
Insomnia |
6 |
14.6 |
3 |
7.3 |
4 |
9.77 |
13 |
-50 |
|
Sleep deprivation |
5 |
12.2 |
4 |
9.8 |
4 |
9.77 |
13 |
-25 |
|
Total |
N = 127 |
N = 133 |
N = 159 |
|
|
|||
|
Mean = 3.1 |
Mean = 3.2 |
Mean = 3.9 |
|
|
||||
|
SD = 2.1 |
SD = 2.4 |
SD =2.9 |
|
|
||||
Note: SD: Standard deviation.
Source: research data, 2021.
The ND "Anxiety" was the second most frequent at admission (41.5%). However, after intubation and before the outcome, its frequency reduced considerably to 9.8% and 12.2%, respectively, showing the largest decline variation (-240%). In all three moments, the diagnoses "Insomnia" and "Sleep Deprivation" were the least frequent.
When analyzing the sociodemographic and clinical variables, only one association was statistically significant: for the diagnosis "Ineffective Breathing Pattern", the distribution of cases between older adults and the very old (> 80 years) was significant (p ≤ 0.05).
Considering the odds ratio between the diagnoses, significant interactions were identified in the three moments. At ICU admission (Table 2), the ND "Risk for Falls" was associated with a 4.8-fold increase (95% CI: 1.1 – 21.2) in the odds of "Risk for Unstable Blood Glucose" occurring and an 8-fold increase (95% CI: 1.2 – 52.9) in the odds of "Ineffective Breathing Pattern". In turn, "Ineffective Breathing Pattern" was associated with a 27.7-fold increase (95% CI: 1.4 – 534.8) in the odds of the ND "Anxiety".
In the assessment after OTI, the presence of "Risk for Impaired Skin Integrity" was associated with a 4.8-fold increase (95% CI: 1.1 – 21.2) in the odds of "Risk for Constipation", a 5.4-fold increase (95% CI: 1.2 – 23.0) for "Risk for Unstable Blood Glucose", and a 59-fold increase (95% CI: 2.9 – 1184) for "Ineffective Breathing Pattern". The latter, in turn, was associated with a 24.2-fold increase in the odds of "Risk for Constipation" occurring (95% CI: 2.4 – 245.9).
Table 2 - Odds ratio between diagnoses at the time of ICU admission, after OTI, and before the outcome. Goiânia, GO, Brazil, 2021
|
1st Moment – Admission |
||||||
|
ND |
RF |
RISI |
RUBG |
RC |
A |
RI |
|
RGI |
4.8 |
|
|
|
|
|
|
IC 95% |
(1.1 – 21.2) |
|
|
|
|
|
|
RL |
|
|
14 |
|
|
|
|
IC 95% |
|
|
(1.4 – 143.6) |
|
|
|
|
PRI |
8 |
|
|
|
27.7 |
|
|
IC 95% |
(1.2 – 52.9) |
|
(1.4 – 534.8) |
|||
|
2nd Moment – Post Orotracheal Intubation |
||||||
|
ND |
RF |
RISI |
RUBG |
RC |
A |
RI |
|
RUBG |
|
5.4 |
|
|
|
|
|
IC 95% |
(1.2 – 23) |
|
|
|
||
|
RC |
|
4.8 |
|
|
|
|
|
IC 95% |
(1.1 – 21.2) |
|
|
|
||
|
RI |
5.11 |
|
|
|
15.5 |
|
|
IC 95% |
(1.1 – 24.9) |
|
(1.4 – 175.4) |
|||
|
IBP |
|
59 |
|
24.2 |
|
|
|
IC 95% |
(2.9 – 1184) |
(2.4 – 245.9) |
|
|||
|
3rd Moment – Outcome |
||||||
|
ND |
RF |
RISI |
RUBG |
RC |
A |
RI |
|
IBP |
|
5.4 |
|
5.0 |
|
5.0 |
|
IC 95% |
(1.4 – 25.9) |
(1.0 – 23.9) |
(1.0 – 23.9) |
|||
|
IAC |
|
|
|
|
7.5 |
|
|
IC 95% |
|
|
|
(1.0 – 55) |
||
Note: RF – Risk for Falls; RISI – Risk for Impaired Skin Integrity; RUBG – Risk for Unstable Blood Glucose; RC – Risk for Constipation; A – Anxiety; RI – Risk for Injury; IBP – Ineffective Breathing Pattern; IAC – Ineffective Airway Clearance.
Source: research data, 2021.
In the pre-outcome assessment (death or extubation), "Ineffective Breathing Pattern" increased the chances of three diagnoses occurring: 5.4 times for "Risk for Impaired Skin Integrity" (95% CI: 1.4 – 25.9), and 5 times for both "Risk for Constipation" (95% CI: 1.0 – 23.9) and "Risk for Injury" (95% CI: 1.0 – 23.9). It was also found that the ND "Anxiety" increased the chances for the occurrence of the ND "Ineffective Airway Clearance" by 7.5 times (95% CI: 1.0 – 55).
DISCUSSION
The results of this study highlight the frequency of nursing diagnoses (ND) at different moments of hospitalization in an intensive care unit (ICU), as well as their clinical characteristics. Most patients were male and had comorbidities that are risk factors for greater severity, such as arterial hypertension and diabetes mellitus, similar to what has been found in other studies(8-9,11). Regarding the human responses arising from this health condition, it is observed that the frequency of NDs increased over time, especially with the need for invasive therapies, such as mechanical ventilation, thus being a possible indicator of care demands(20-21,23).
The ND with the highest frequency in the three analyzed moments was "Risk for Infection", defined by NANDA-I as the "susceptibility to invasion and multiplication of pathogenic organisms"(17). This ND showed a positive growth variation at the outcome compared to admission. This increase may be related to the worsening of the clinical picture and hemodynamic instability, with the consequent need to perform a greater number of invasive procedures, longer permanence of devices, and greater exposure to pathogens that accompany the length of stay in critical care(24).
Another risk factor for this diagnosis is the impaired immune response itself. Aging, by itself, causes changes in the immune system, resulting in decreased innate and acquired immunity(1), and in critical cases of COVID-19, a worsening of this dysfunction is observed(25). In a cross-mapping study that used medical records of adult patients with COVID-19 in the ICU, the diagnosis "Risk for Infection" had a prevalence of 45.61%(26).
Therefore, although it did not increase the chances of other diagnoses occurring in this study, its risk factors are well-established in the literature and closely related to the performance of patient safety management practices(27), with its high frequency being a possible reflection of the institutional safety culture in the investigated unit.
Another diagnosis with high frequency and identified in all three moments of the study was "Risk for unstable blood glucose". It should be noted that this diagnosis was renamed in the NANDA-I 2024-2026 edition to Risk for ineffective self-management of blood glucose pattern and adopts the definition "susceptibility to unsatisfactory management of symptoms, therapeutic regimen, and lifestyle changes associated with living with recurrent fluctuations in blood glucose level outside the desirable range"(17).
It is estimated that approximately 828 million adults worldwide have diabetes, an increase of 630 million since 1990(28). Older adults with COVID-19 in critical care have a high prevalence of DM(6,9), in addition to frequently manifesting excessive stress(29), excessive weight loss, and inadequate food intake(25), which are additional risk factors for this undesirable human response(17).
A systematic review and meta-analysis demonstrated that the lack of glycemic control in critically ill patients with COVID-19 and DM is related to an increased mortality rate, increased infection rate, need for mechanical ventilation, and prolonged hospitalization(30). Therefore, it is of fundamental importance to implement early and personalized strategies to achieve the best glycemic control from admission to the ICU. In line with this finding, in a study conducted to identify possible NANDA-I NDs in critically ill patients with COVID-19, the diagnosis "Risk for unstable blood glucose" was considered valid for this clinical context with 100% agreement from expert nurses(31).
Another relevant diagnosis in this study was "Risk for Falls", defined by NANDA-I in the context of the adult as "susceptibility of an individual > 18 years of age to experience an event that results in an inadvertent displacement to the ground, floor, or other lower surface area"(17). Falls are considered a growing public health problem(32), and frequent assessment of risk status is considered a quality indicator for care, in addition to being one of the international patient safety goals(33).
The occurrence of falls in the ICU is less frequent when compared to other sectors of the hospital(34). In a study that compared fall rates and associated harm in a private hospital, it was identified that, in a one-year period, 90.9% of falls occurred in the Inpatient Units and 9.1% in the ICUs(35). In the present study, the high frequency and linear increase of this diagnosis, when compared to the others, may be associated with low accuracy of the diagnostic process, in addition to the non-reassessment of the maintenance of previously listed NDs at different moments of hospitalization.
However, regardless of the assessment setting, falls in hospitalized patients can result in physical and psychological harm, increase the length of hospitalization and hospital costs, justifying the careful assessment and monitoring of risk gradation(33). In research that investigated the care of hospitalized patients with COVID-19, among the most frequently documented nursing interventions, environmental management stood out, which includes practices such as raising bed rails, aiming to prevent falls and other adverse events(36).
Adult patients at risk for falls may present predisposing factors related to unstable glycemic levels, such as the occurrence of hypoglycemia not addressed in time by the team(30) or a delay in starting nutritional therapy due to clinical instability(37). It is not a matter of causality where "Risk for Falls" causes unstable blood glucose. On the contrary, the critical condition of the older adult, exacerbated by COVID-19, predisposes to a multifactorial dysfunction that impacts both balance and mobility (increasing the risk of falls) and metabolic regulation (leading to glycemic instability). In addition, critical illness is a condition that increases the chances of glycemic instability, justifying more frequent monitoring of this response in the ICU(17).
Similarly, the association between "Risk for falls" and "Ineffective breathing pattern" at admission may indicate that patients with greater fragility and general instability, prone to falls, also present greater respiratory compromise due to the severity of the disease, sedation, muscle weakness, and immobility, factors that, in turn, contribute to an ineffective breathing pattern(38).
The diagnosis "Risk for impaired skin integrity" showed a positive evolution throughout the observed moments. Older adults with COVID-19 on IMV are more susceptible to this human response due to impaired physical mobility, advanced age, presence of comorbidities, decreased level of consciousness, and decreased tissue oxygenation(39). Additionally, older adults present changes in skin structure and function, such as a reduction in elastic and collagen fibers, which leads to greater dryness and reduced thickness, favoring the loss of integrity(40). Therefore, both people at the extremes of age and those hospitalized in intensive care are recognized as populations at risk for this diagnosis(17).
The odds ratios identified reveal complex associations between NDs, which demand careful interpretation in the clinical context. It is essential to recognize that, in observational studies, a statistical association does not necessarily imply a cause-and-effect relationship. Frequently, the coexistence of multiple diagnoses reflects the intricate network of shared risk factors and the inherent vulnerabilities of the patient's condition.
It was observed that patients at "Risk for Impaired Skin Integrity" share predisposing factors for constipation, such as impaired physical mobility, inadequate nutritional intake, and fluid and electrolyte imbalance, which delay peristalsis and the formation of the fecal bolus(17,41-42). Regarding "Risk for Unstable Blood Glucose", inadequate nutritional intake and smoking are common risk factors that influence both diagnoses, which may reinforce a common trigger from the interaction in the causal chain(9,17,37-38).
Regarding the increased chances of "Ineffective breathing pattern" from "Risk for impaired skin integrity", a sharing of risk factors such as bed position and overweight is observed(17), which, although to a lesser extent, can influence the ventilatory process. However, the multisystemic nature of the critically ill patient reinforces the picture of severity that leads to immobilization, sedation, and organ dysfunction, impacting skin integrity and intestinal function. It is also noteworthy that the odds ratio for this finding had a very wide CI, which requires caution in interpretation.
The frequency of the ND "Risk for injury" had a positive variation of 50% from admission to the outcome. This ND was conceptualized by NANDA-I (2021-2023 edition) as "susceptibility to physical injury due to environmental conditions interacting with the individual's adaptive and defensive resources, which may compromise health"(43). The presence of this ND may result from the physical barriers of the ICU, the process of cognitive dysfunction due to hypoxia, unsafe modes of transport, and greater exposure to pathogens(44), which also justifies the association with "Anxiety" and "Risk for falls".
However, in similar studies and area consensuses, this ND was not identified(20-21,26,31), unlike its more specific variations, such as "Risk for corneal injury" and "Risk for pressure injury". As a pre-formatted form was used at the institution, it is possible that the high frequency of this ND is related to the non-specification of the diagnostic axes in the nursing record, harming the accuracy of the process.
In the intensive care setting, the emphasis on NDs that encompass the domain of coping and stress tolerance(17) is not commonly recorded, with care directed towards physiological needs. In a study that described the frequency of NDs in patients with COVID-19, anxiety was one of the most recorded (84%), however, these records were in patients who did not require orotracheal intubation(45). It is believed that anxiety may be related to the severity of the disease, isolation, the absence of significant people, and the feeling of abandonment(46).
The ND "Risk for constipation" was also frequent from the second moment and persisted until the outcome. In patients with severe COVID-19, it was observed that enteral nutrition is feasible, but the incidence of constipation was found in 87% of these patients(37). Furthermore, the SARS-CoV-2 virus infects cells through the Angiotensin-Converting Enzyme 2 receptor, present in large quantities in the gastrointestinal tract, which may increase the risk of constipation(47).
It is also noteworthy that patients with altered breathing patterns may experience an exacerbation of stress and anxiety(48-50), reducing mobility in bed to achieve a balance between oxygen demand and supply. Added to this is the fact that, due to clinical instability, such patients require greater assistance in self-care for activities such as eating and bathing, altering the patient's routine and reducing their autonomy(17,23). Together, all these factors contribute to the risk of constipation.
Regarding the diagnosis "Ineffective breathing pattern", there was an increase of 10.4% in the third moment compared to the two previous ones, proving significant in older patients. This human response is characterized as "difficulty in maintaining adequate ventilation during inspiration and/or expiration"(17). Patients affected by COVID-19 were dealing, in the acute phase of the pandemic, with an unknown situation and excessive stress, which may justify the anxiety, which, in turn, amplifies the severity of the "Ineffective breathing pattern"(38,49-50).
In similar studies, "Ineffective Breathing Pattern" was evidenced along with other oxygenation responses, such as "Impaired gas exchange" and "Impaired spontaneous ventilation"(13,20,26,31,48). Another study identified significantly different frequencies in patients with (100%) and without (66.7%) COVID-19 in the same ICU(51). Thus, it is important to observe that, in the course of this health condition, respiratory responses are significant and demand time-dependent nursing care, with safe and assertive decision-making(50,52).
However, although respiratory diagnoses were observed, the absence of records related to the diagnosis Dysfunctional ventilatory weaning response: adult(17) is noteworthy. Weaning from mechanical ventilation is a common activity that requires nurse expertise to early assess failures in the spontaneous breathing test(53). In a study with critically ill patients with COVID-19, this diagnosis was the least identified(20).
The Federal Nursing Council has a specific resolution on the competencies of nurses in the care of patients on mechanical ventilation(54), but it is observed that their approach to weaning is still fragile, which justifies the absence of identification of this response and the isolated presence of others that influence it unfavorably, such as "Ineffective airway clearance"(17). A study that evaluated the adult population with COVID-19 identified a prevalence of 36.5% for this diagnosis, with the older adults the largest portion(55).
Paper records or pre-formatted forms, such as those used in this study, tend not to fully represent the judgments made by nurses, in addition to demanding more time and harming the accuracy of the record(56-58). Another factor is that, during the pandemic, nurses had difficulties in implementing the nursing process due to the sudden increase in workload(59), which resulted in lower diagnostic accuracy. Thus, these factors together may explain some inconsistencies observed in the results.
As study limitations, the impossibility of generalizing the results stands out as they correspond to data from a secondary source, from a single center, and from an initial period of the pandemic. Additionally, the observational and retrospective nature does not allow for establishing cause-and-effect relationships, with the odds ratios interpreted as indicators of association. However, the results allow for reflection on nursing practice in other contexts and advance by presenting diagnostic profiles in distinct phases of patient evolution, which minimizes this limitation.
CONCLUSION
The prevalence of nursing diagnoses in different phases of COVID-19 in older adults on mechanical ventilation demonstrates the complexity of the care required throughout the hospitalization of the critically ill patient. The diagnosis "Risk for Infection" was the most prevalent in the three investigated moments. After orotracheal intubation and at the clinical outcome, other responses, such as "Risk for falls" and "Risk for impaired skin integrity", were also identified. Before intubation, the presence of coping responses, such as "Anxiety", and those related to care management, such as "Risk for unstable blood glucose", are highlighted.
The intrinsic frailty of the older adult patient, pre-existing comorbidities, and the systemic impact of COVID-19 create a favorable environment for the simultaneous manifestation of multiple diagnoses. These interactions provide valuable insights into the interconnection of Nursing Diagnoses, whose clinical complexity points to the coexistence and interdependence of phenomena. Such phenomena must be understood by nursing with the aim of developing more integrated care plans and preventive interventions, optimizing the safety and quality of care.
Despite the end of the public health emergency period of the COVID-19 pandemic, studies that retrospectively evaluate the clinical evolution of patients who were hospitalized, especially in the severe form, point to paths to be overcome to improve nursing care in intensive therapy. Furthermore, they contribute to the reflection on current practice and elucidate the natural history of this condition from the perspective of the nursing discipline.
CONFLICT OF INTERESTS
The authors declare no conflict of interests.
FUNDING
Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq (100391/2023-0).
1. Akinosoglou K, Schinas G, Almyroudi MP, Gogos C, Dimopoulos G. The impact of age on intensive care. Ageing Res Rev. 2023;84:101832. https://doi.org/10.1016/j.arr.2022.101832
2. Associação de Medicina Intensiva Brasileira. Características das internações [Internet]. São Paulo: UTIs Brasileiras; c2023 [cited 2025 Aug 18]. Available from: https://www.utisbrasileiras.com/caracteristicas-das-internacoes/
3. Ferretti-Rebustini RE de L, Nogueira L de S, Silva R de CGE, Poveda V de B, Machado SP, Oliveira EM de, et al. Aging as a predictor of nursing workload in Intensive Care Unit: results from a Brazilian Sample. Rev Esc Enferm USP. 2017;51:e03216. https://doi.org/10.1590/s1980-220x2016237503216
4. Ribeiro JB, Lopes FJ, Barbosa AC de L, Gallasch CH, Santos ES, Ferretti-Rebustini RE de L. Nursing Workload and care required by older adults in intensive care. Rev. bras. geriatr. gerontol. 2023;26:e230134. https://doi.org/10.1590/1981-22562023026.230134.en
5. Abate SM, Checkol YA, Mantefardo B. Global prevalence and determinants of mortality among patients with COVID-19: A systematic review and meta-analysis. Ann Med Surg (Lond). 2021;64:102204. https://doi.org/10.1016/j.amsu.2021.102204
6. Macedo LR, Araújo CB de, Carvalho LF de, Lobato JCP, Paiva NS, Costa AJL. Excesso de mortalidade geral e mortalidade por COVID-19 no Brasil e regiões no ano de 2020. Cad Saude Publica. 2025;40(11):e00217323. https://doi.org/10.1590/0102-311XPT217323
7. Abul Y, Leeder C, Gravenstein S. Epidemiology and Clinical Presentation of COVID-19 in Older Adults. Infect Dis Clin North Am. 2023;37(1):1-26. https://doi.org/10.1016/j.idc.2022.11.001
8. Batista MJ, Lino CM, Tenani CF, Barbosa AP, Latorre M do RD de O, Marchi E. COVID-19 Mortality among Hospitalized Patients: Survival, Associated Factors, and Spatial Distribution in a City in São Paulo, Brazil, 2020. Int J Environ Res Public Health. 2024;21(9):1211. https://doi.org/10.3390/ijerph21091211
9. Fériz-Bonelo KM, Iriarte-Durán MB, Giraldo O, Parra-Lara LG, Martínez V, Urbano MA, et al. Clinical outcomes in patients with diabetes and stress hyperglycemia that developed SARS-CoV-2 infection. Biomedica. 2024;44(Sp. 1):73-88. https://doi.org/10.7705/biomedica.7095
10. Brito C, de Araujo Mariz C, Freitas de Oliveira França R, Lopes EP, Silva LE, Neto RL, et al. Clinical-laboratory characteristics predictive of COVID-19 severity: a prospective hospital cohort, in Pernambuco, Northeast Brazil. Braz J Microbiol. 2024;55(3):2643-2654. https://doi.org/10.1590/0037-8682-0119-2022
11. Cardoso JP, Calazans MIP, Carneiro ALFC, Costa CM, Monteiro ELO, Aristizábal LYG, et al. Association between multimorbidity, intensive care unit admission, and death in patients with COVID-19 in Brazil: a cross-section study, 2020. Sao Paulo Med J. 2022;141(3):e2022226. https://doi.org/10.1590/1516-3180.2022.0226.R1.21072022
12. Green A, Rachoin JS, Schorr C, Dellinger P, Casey JD, Park I, et al. Timing of invasive mechanical ventilation and death in critically ill adults with COVID-19: A multicenter cohort study. PLoS One. 2023;18(6):e0285748. https://doi.org/10.1371/journal.pone.0285748
13. Maurício AB, Cavalcante AMRZ, de Sá ES, Bruni LG, Vieira LGD, Costa A, et al. Accuracy of the defining characteristics of respiratory nursing diagnoses in patients with COVID-19. Int J Nurs Knowl. 2025;36(3):275-283. https://doi.org/10.1111/2047-3095.12481
14. Brasil. Conselho Federal de Enfermagem. Resolução COFEN nº 736, de 17 de janeiro de 2024. Dispõe sobre a implementação do Processo de Enfermagem em todo contexto socioambiental onde ocorre o cuidado de enfermagem. Diário Oficial da União. 2024 Jan 23;Seção 1(16):74.
15. Monsen KA, Heermann Langford L, Bakken S, Dunn Lopez K. Standardized nursing terminologies come of age: advancing quality of care, population health, and health equity across the care continuum. J Am Med Inform Assoc. 2023;30(11):1757-1759. https://doi.org/10.1093/jamia/ocad173
16. Rabelo-Silva ER, Dantas Cavalcanti AC, Ramos Goulart Caldas MC, Lucena A de F, Almeida M de A, Linch GF da C, et al. Advanced Nursing Process quality: Comparing the International Classification for Nursing Practice (ICNP) with the NANDA-International (NANDA-I) and Nursing Interventions Classification (NIC). J Clin Nurs. 2017;26(3-4):379-387. https://doi.org/10.1111/jocn.13387
17. Herdman TH, Kamitsuru S, Lopes CT, editores. NANDA-I nursing diagnoses: definitions and classification 2024-2026. 13th ed. New York: Thieme; 2024.
18. Kim M, Kim Y, Choi M. Intensive care unit nurses’ experiences of nursing concerns, activities, and documentation on patient deterioration: A focus-group study. Aust Crit Care. 2025;38(2):101126. https://doi.org/10.1016/j.aucc.2024.09.011
19. De Groot K, De Veer AJE, Paans W, Francke AL. Use of electronic health records and standardized terminologies: A nationwide survey of nursing staff experiences. Int J Nurs Stud. 2020;104:103523. https://doi.org/10.1016/j.ijnurstu.2020.103523
20. Lima-Medeiros GM de, Menezes-Dos-Santos CR, Jesus-Santos T de, Fraga-Santos E, Centenaro-Vaez A, Soares-Pinheiro FG de M, et al. Nursing diagnoses for patients hospitalized with COVID-19 in critical care units in Brazil: A cross-sectional study. Enferm Intensiva (Engl Ed). 2025;36(2):500541. https://doi.org/10.1016/j.enfie.2025.500541
21. Gomes GLL, Oliveira FMRL de, Leal NP da R, Guimarães KSL, Silva DF da, Barbosa KTF. Diagnósticos/resultados e intervenções de enfermagem para pacientes com COVID-19: estudo documental retrospectivo. Online Braz. J. Nurs. 2021;20(Suppl 1):e6512. https://doi.org/10.17665/1676-4285.2021651
22. Ghaferi AA, Schwartz TA, Pawlik TM. STROBE Reporting Guidelines for Observational Studies. JAMA Surg. 2021;156(6):577-578. https://doi.org/10.1001/jamasurg.2021.0528
23. Borges F, Bernardino E, Rorato C, Bobrowec DCDR, Silva OLDS, Carvalho AGRP de, et al. Nursing care for hospitalized patients with COVID-19 in light of Fundamental Care. Rev Bras Enferm. 2025;78(2):e20240075. https://doi.org/10.1590/0034-7167-2024-0075
24. Paiva R de M, Ferreira L de L, Bezerril MDS, Chiavone FTB, Salvador PTC de O, Santos VEP. Infection factors related to nursing procedures in Intensive Care Units: a scoping review. Rev Bras Enferm. 2021;74(1):e20200731. https://doi.org/10.1590/0034-7167-2020-0731
25. Castro-Trujillo S, Castro-Meneses J, Rojas MC, Castro-Amaya M, Lastra G, Narváez CF. Regulatory cytokines modulate early isotype-specific response associated with COVID-19 survival. Front Immunol. 2025;16:1543626. https://doi.org/10.3389/fimmu.2025.1543626
26. Silva CLB de, Moura EL de, Dantas TN do N, Matias KC, Carvalho LM de, Vitor AF. Nursing diagnoses in patients with COVID-19 admitted to the intensive care unit: CROSS-MAPPING. Heliyon. 2024;10(5):e27088. https://doi.org/10.1016/j.heliyon.2024.e27088
27. Silva AMB da, Bim LL, Bim FL, Sousa AFL, Domingues PCA, Nicolussi AC, et al. Patient safety and infection control: bases for curricular integration. Rev Bras Enferm. 2018;71:1170-1177. https://doi.org/10.1590/0034-7167-2017-0314
28. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet. 2024;404(10467):2077-2093. https://doi.org/10.1016/S0140-6736(24)02317-1
29. Zahedi M, Kordrostami S, Kalantarhormozi M, Bagheri M. A Review of Hyperglycemia in COVID-19. Cureus. 2023;15(4):e37487. https://doi.org/10.7759/cureus.37487
30. Chander S, Deepak V, Kumari R, Leys L, Wang HY, Mehta P, et al. Glycemic Control in Critically Ill COVID-19 Patients: Systematic Review and Meta-Analysis. J Clin Med. 2023;12(7):2555. https://doi.org/10.3390/jcm12072555
31. Azevedo C, Moura C de C, Salgado PO, Mata LRF da, Domingos CS, Ercole FF, et al. NANDA-I® nursing diagnoses in adult critical patients with COVID-19. Acta Paul. Enferm. (Online). 2022;35:eAPE03722. http://dx.doi.org/10.37689/acta-ape/2022AO03722
32. Heikkilä A, Lehtonen L, Junttila K. Consequences of Inpatient Falls in Acute Care: A Retrospective Register Study. J Patient Saf. 2024;20(5):340-344. https://doi.org/10.1097/PTS.0000000000001230
33. McKercher JP, Peiris CL, Hill AM, Peterson S, Thwaites C, Fowler-Davis S, et al. Hospital falls clinical practice guidelines: a global analysis and systematic review. Age Ageing. 2024;53(7):afae149. https://doi.org/10.1093/ageing/afae149
34. Assis SF de, Vieira DFVB, Sousa FREG de, Pinheiro CE de O, Prado PR do. Adverse events in critically ill patients: a cross-sectional study. Rev Esc Enferm USP. 2022;56:e20210481. https://doi.org/10.1590/1980-220X-REEUSP-2021-0481en
35. Specht AM, Sousa GP de, Beghetto MG. Incidence of falls in a cohort of critical adults: a cause for concerns? Rev Gaucha Enferm. 2020;41(spe):e20190167. https://doi.org/10.1590/1983-1447.2020.20190167
36. Asghari E, Archibald M, Roshangar F. Nursing interventions for patients with COVID-19: A medical record review and nursing interventions classification study. Int J Nurs Knowl. 2022;33(1):57-63. https://doi.org/10.1111/2047-3095.12332
37. Osuna-Padilla I, Rodríguez-Moguel NC, Aguilar-Vargas A, Rodríguez-Llamazares S. Safety and tolerance of enteral nutrition in COVID-19 critically ill patients, a retrospective study. Clin Nutr ESPEN. 2021;43:495-500. https://doi.org/10.1016/j.clnesp.2021.02.015
38. Lopes MV de O, Silva VM da, Herdman TH. Causation and Validation of Nursing Diagnoses: A Middle Range Theory. Int J Nurs Knowl. 2017;28(1):53-59. https://doi.org/10.1111/2047-3095.12104
39. Frota OP, Paula FM, Ferreira DN, Ferreira-Júnior MA, Domingues EAR, Ruiz JS, et al. Incidence, characteristics and influencing factors of medical adhesive-related skin injury in the indwelling urinary catheter attachment region in critically ill patients: A longitudinal study. Nurs Crit Care. 2025;30(2):e13253. https://doi.org/10.1111/nicc.13253
40. Lichterfeld-Kottner A, El Genedy M, Lahmann N, Blume-Peytavi U, Büscher A, Kottner J. Maintaining skin integrity in the aged: A systematic review. Int J Nurs Stud. 2020;103:103509. https://doi.org/10.1016/j.ijnurstu.2019.103509
41. Batassini É, Beghetto MG. Constipation in a cohort prospective in adult critically ill patients: How much occurs and why? Enferm Intensiva (Engl Ed). 2019;30(3):127-134. https://doi.org/10.1016/j.enfie.2018.08.001
42. Pérez-Sánchez J, Fernández-Boronat J, Martínez-Méndez E, Marín-Cagigas ML, Mota-Puerto D, Pérez-Román MC, et al. Evaluation and handling of constipation in critical patients. Enferm Intensiva. 2017;28(4):160-168. https://doi.org/10.1016/j.enfie.2017.10.003
43. Herdman TH, Kamitsuru S, Lopes CT, editores. NANDA-I nursing diagnoses: definitions and classification 2021-2023. 12th ed. New York: Thieme; 2021.
44. Tajari M, Ashktorab T, Ebadi A. Components of safe nursing care in the intensive care units: a qualitative study. BMC Nurs. 2024;23(1):613. https://doi.org/10.1186/s12912-024-02281-5
45. Hernández AD, Márquez DLD, Muñiz GM, Garcia CÁT. Frecuencia de diagnósticos de enfermería en pacientes hospitalizados con infección Covid-19. Rev. enferm. neurol. 2022;21(1):29-40. https://doi.org/10.51422/ren.v21i1.343
46. Correia TSP, Martins MMFPS, Barroso FF, Pinho LG, Fonseca C, Valentim O, et al. The Implications of Family Members’ Absence from Hospital Visits during the COVID-19 Pandemic: Nurses’ Perceptions. Int J Environ Res Public Health. 2022;19(15):8991. http://dx.doi.org/10.3390/ijerph19158991
47. Santra D, Banerjee A, De SK, Thatoi H, Maiti S. Relation of ACE2 with co-morbidity factors in SARS-CoV-2 pathogenicity. Comp Clin Path. 2023;32(2):179-189. https://doi.org/10.1007/s00580-023-03434-9
48. Santos CRM dos, Santos T de J, Vaez AC, Araújo D de C. Analysis of the nursing diagnosis of [ineffective breathing pattern (00032)] in patients hospitalized with COVID-19: A cross-sectional study. Int J Nurs Knowl. 2025;1-9. https://doi.org/10.1111/2047-3095.70007
49. Maurício AB, Silva VM da, Cavalcante AMRZ, Bruni LG, Moorhead SA, Swanson E, et al. Evidence of internal structure validity of the nursing outcome "Mechanical Ventilation Weaning Response: Adult (0412)" for critically ill COVID-19 patients. Int J Nurs Knowl. 2025;1-10. https://doi.org/10.1111/2047-3095.70020
50. Barreto LNM, Silva MB da, Nomura ATG, Lucena A de F, Almeida M de A. Clinical evolution of nursing outcome indicators in patients with ineffective breathing pattern. Rev. eletrônica enferm. 2020;22:60784. https://doi.org/10.5216/ree.v22.60784
51. Barioni EMS, Nascimento C da S do, Amaral TLM, Ramalho Neto JM, Prado PR do. Clinical indicators, nursing diagnoses, and mortality risk in critically ill patients with COVID-19: a retrospective cohort. Rev Esc Enferm USP. 2022;56:e20210568. https://doi.org/10.1590/1980-220X-REEUSP-2021-0568en
52. Sá ES de, Maurício AB, Bruni LG, Vieira LGD, Santos VB, Cavalcante AMRZ, et al. Content analysis of NOC outcomes related to mechanical ventilation in people with COVID-19. Rev Esc Enferm USP. 2024;58:e20230343. https://doi.org/10.1590/1980-220X-REEUSP-2023-0343en
53. Silva LCR da, Tonelli IS, Oliveira RCC, Lemos PL, Matos SS de, Chianca TCM. Clinical study of Dysfunctional Ventilatory Weaning Response in critically ill patients. Rev Lat Am Enfermagem. 2020;28:e3334. https://doi.org/10.1590/1518-8345.3522.3334
54. Brasil. Conselho Federal de Enfermagem. Resolução COFEN nº 639/2020. Dispõe sobre as competências do Enfermeiro no cuidado aos pacientes em ventilação mecânica no ambiente extra e intra-hospitalar. Diário Oficial da União. 2020 Maio 8;Seção 1(87):222.
55. Dantas JR, Almeida ATD, Matias KC, Fernandes MI da CD, Tinôco JD de S, Lopes MV de O, et al. Accuracy of the nursing diagnosis of ineffective airway clearance in intensive care unit patients. Rev Bras Enferm. 2023;76(1):e20220174. https://doi.org/10.1590/0034-7167-2022-0174
56. Akhu-Zaheya L, Al-Maaitah R, Bany Hani S. Quality of nursing documentation: Paper-based health records versus electronic-based health records. J Clin Nurs. 2018;27(3-4):e578-3589. https://doi.org/10.1111/jocn.14097
57. Baumann LA, Baker J, Elshaug AG. The impact of electronic health record systems on clinical documentation times: A systematic review. Health Policy. 2018;122(8):827-836. https://doi.org/10.1016/j.healthpol.2018.05.014
58. Hants L, Bail K, Paterson C. Clinical decision-making and the nursing process in digital health systems: An integrated systematic review. J Clin Nurs. 2023;32(19-20):7010-7035. https://doi.org/10.1111/jocn.16823
59. Tosun H, Tosun A, Ödül Özkaya B, Gül A. The Most Commonly Determined Nursing Diagnoses According to NANDA-I Taxonomy and Difficulties Using the Nursing Process in COVID-19 Outbreak. Clin Nurs Res. 2022;31(3):395-403. https://doi.org/10.1177/10547738211051565
Submission: 21-Jul-2025
Approved: 08-Oct-2025
Editors:
Rosimere Ferreira Santana (ORCID: 0000-0002-4593-3715)
Geilsa Soraia Cavalcanti Valente (ORCID: 0000-0003-4488-4912)
Suzana Mangueira (ORCID: 0000-0003-0931-8675)
Corresponding author: Agueda Maria Ruiz Zimmer Cavalcante (aguedacavalcante@ufg.br)
Publisher:
Escola de Enfermagem Aurora de Afonso Costa – UFF
Rua Dr. Celestino, 74 – Centro, CEP: 24020-091 – Niterói, RJ, Brazil
Journal email: objn.cme@id.uff.br
|
AUTHORSHIP CONTRIBUTIONS |
|
Study conception: Queiroz IB, Sá ES, Silva RC, Cavalcante AMRZ. Data acquisition: Queiroz IB, Sá ES. Data analysis: Silva RC, Cavalcante AMRZ. Data interpretation: Queiroz IB, Sá ES, Silva RC, Cavalcante AMRZ. All authors are responsible for the textual writing and critical review of the intellectual content, for the final published version, and for all ethical, legal, and scientific aspects related to the accuracy and integrity of the study. |
