
ORIGINAL ARTICLE
HIV TESTING AT HOSPITAL ADMISSION FOR CHILDBIRTH AND ITS INTERFERENCE WITH BREASTFEEDING: A QUALITATIVE STUDY
Mariana Viana Toledo1, Fernanda Garcia Bezerra Góes2, Fernanda Maria Vieira Pereira Ávila3, Maria da Anunciação Silva4, Nátale Gabriele Ferreira Nunes5, Luana Zaine Aleixo Silvério6
1 Fluminense Federal University, Institute of Health Humanities. Rio das Ostras, RJ, Brazil. ORCID: 0009-0004-1933-6345. Email: marianavianatoledo@id.uff.br
2 Fluminense Federal University, Institute of Health Humanities. Rio das Ostras, RJ, Brazil. ORCID: 0000-0003-3894-3998. Email: ferbezerra@gmail.com
3 Fluminense Federal University, Institute of Health Humanities. Rio das Ostras, RJ, Brazil. ORCID: 0000-0003-1060-6754. Email: fernandamvp@id.uff.br
4 Fluminense Federal University, Institute of Health Humanities. Rio das Ostras, RJ, Brazil. ORCID: 0000-0002-0069-5100. Email: suncahsilva@gmail.com
5 Federal University of the State of Rio de Janeiro, Graduate Program in Nursing and Biosciences. Rio de Janeiro, RJ, Brazil. ORCID: 0000-0001-5335-7140. Email: ferreiranatale@gmail.com
6 Fluminense Federal University, Institute of Health Humanities. Rio das Ostras, RJ, Brasil. ORCID: 0009-0007-1491-892X. Email: luanazainealeixo@gmail.com
ABSTRACT
Objective: To understand the interference of HIV testing performed at hospital admission for childbirth on breastfeeding within the first hour of life. Method: A qualitative, exploratory-descriptive study conducted between December 2024 and June 2025, using semi-structured interviews at a maternity hospital in the Baixada Litorânea region of Rio de Janeiro, Brazil. A total of 35 participants were included: 20 healthcare professionals (five nursing technicians, 12 nurses, and three physicians) and 15 family members (14 postpartum women and one newborn’s aunt). Data were processed using the software Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires (IRAMUTEQ) and subjected to Thematic Analysis. Results: HIV testing at hospital admission for childbirth directly interferes with breastfeeding within the first hour of life, delaying the initiation of this practice. Although it constitutes an institutional routine, its implementation varies according to the professionals’ practices and the type of test performed (rapid or laboratory), and it is affected by material shortages. This dynamic compromises breastfeeding, often resulting in the use of formula. Conclusion: Care workflows must be reconsidered so that HIV testing at hospital admission for childbirth does not hinder breastfeeding within the first hour of life, allowing both practices to occur in an integrated, safe, and timely manner.
Descriptors: Pregnancy; Newborn; HIV Test; Breastfeeding; Hospitals; Nursing.
|
How to cite: Toledo MV, Góes FGB, Ávila FMVP, Silva MA, Nunes NGF, Silvério LZA. HIV testing at hospital admission for childbirth and its interference with breastfeeding: a qualitative study. Online Braz J Nurs. 2025;24:e20256873. https://doi.org/10.17665/1676-4285.20256873 |
What is already known:
Breastfeeding within the first hour of life is an important indicator of neonatal and maternal health, with significant impacts on the well-being of both mother and baby;
Few studies describe the interference of HIV testing performed at hospital admission for childbirth on breastfeeding within the first hour of life.
What this article adds:
The choice of the type of HIV test at hospital admission for childbirth has caused delays in initiating breastfeeding after birth;
The implementation of HIV testing in maternity wards varies according to the practices adopted by professionals and the type of test performed (rapid or laboratory);
The choice of HIV test is influenced by the lack of material resources.
INTRODUCTION
Breastfeeding is widely recommended and offers numerous benefits. For the infant, breast milk prevents infections, diarrhea, and allergies, reduces the risk of obesity, high cholesterol, hypertension, and diabetes mellitus, and contributes to cognitive and emotional development. Early breastfeeding—the intake of colostrum within the first hour of life, known as the “golden hour”—strengthens the newborn’s immune system and helps reduce neonatal mortality(1).
This practice also reinforces the mother–infant bond, decreases postpartum hemorrhage, and lowers the risk of developing breast, cervical, and ovarian cancer in women. Globally, breastfeeding represents an economical and sustainable alternative, as it does not require production, storage, or consumption processes, and positively impacts the healthcare system by reducing costs associated with treatment and hospitalization of children(2).
The World Health Organization recommends exclusive breastfeeding until six months of age and continued breastfeeding alongside appropriate complementary feeding until two years of age or beyond(1). In Brazil, the Child and Adolescent Statute establishes breastfeeding as a legally guaranteed right, obliging public authorities, institutions, and employers to provide adequate conditions for its implementation(3).
Generally, there are no contraindications to breastfeeding when it is the mother’s desire. However, women living with HIV (Human Immunodeficiency Virus) should not breastfeed due to the risk of viral transmission to the infant through breast milk(4). Given that HIV can be transmitted from mother to child during pregnancy, childbirth, or breastfeeding, HIV testing is recommended during the first and third trimesters of pregnancy, at the time of delivery or abortion, and in other risk situations(5).
Preferably, rapid tests should be used, which require a capillary blood sample obtained via finger prick and provide a qualitative result within 30 minutes, indicating the presence of HIV antibodies. Laboratory tests, which use venous blood samples, allow qualitative and/or quantitative detection of antibodies and/or viral load. However, laboratory results may take several hours to be available and should only be used if the result can be provided in a timely manner(5-6).
In Brazil, between 2000 and June 2023, 158,429 pregnant women, women in labor, and postpartum women were reported as HIV-positive. In 2022, new HIV infections among women of reproductive age (15 to 49 years) accounted for 78.3% of total cases in females(7). During pregnancy, early diagnosis enables prompt initiation of antiretroviral therapy, significantly reducing the risk of vertical HIV transmission(7-8). Prenatal care should facilitate timely detection and treatment of complications, including sexually transmitted infections, and offer HIV testing(7,9). It is essential that pregnant women have access to their test results before delivery(10).
Although HIV testing is also a fundamental strategy during hospital admission for childbirth, it must be carried out in a planned and timely manner. Late testing or delays in result availability compromise early breastfeeding, as demonstrated by a study conducted in Rio de Janeiro(11). In this context, rapid tests are particularly relevant, as results are available within 30 minutes, enabling both the early initiation of antiretroviral therapy for those in need and breastfeeding within the first hour of life for those eligible. Thus, they provide dual protection: preventing vertical HIV transmission while promoting early breastfeeding(5-6).
Few Brazilian studies have examined the interference of HIV testing with breastfeeding within the first hour of life when performed during hospital admission for childbirth. Given the evidence of low breastfeeding rates during the “golden hour”(11), understanding this relationship is essential to support interventions that promote early breastfeeding in maternity wards and improve maternal and neonatal outcomes.
Therefore, the objective of this study was to understand the interference of HIV testing performed at hospital admission for childbirth on breastfeeding within the first hour of life.
METHODS
This was a qualitative, exploratory-descriptive study(12) conducted in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ)(13). The study setting was a maternity ward in a municipal hospital in the Baixada Litorânea region, Rio de Janeiro, Brazil, which serves as the only public reference unit in the municipality.
Participants met the following inclusion criteria: healthcare professionals (nursing technicians, nurses, and physicians) working in the obstetric ward (for the hospitalization of pregnant women), the delivery room/operating room, and/or the mother–baby unit; and pregnant women, postpartum women, and other family members of newborns over 18 years of age, whose babies were in good health. Exclusion criteria included healthcare professionals who were nursing assistants and/or worked exclusively in administrative tasks and/or did not provide direct care to the mother–infant dyad, as well as pregnant women, postpartum women, or family members with any health condition that would hinder participation. Efforts were made to include a diverse range of healthcare professionals and family members to capture multiple perspectives on the phenomenon under study.
Before data collection began, the researcher approached potential participants in person, ensuring they met the inclusion criteria, without any prior relationship. At this time, the study objectives, procedures, risks, and benefits were explained. Participants were then invited to join the study, forming a convenience sample. Some professionals and family members declined participation, but there were no withdrawals among those who consented. Due to these refusals, only one family member, a newborn’s aunt, participated alongside postpartum women.
Data were collected through individual, face-to-face, semi-structured interviews, using an anonymous alphanumeric coding system: “P” for healthcare professionals and “M” for women (postpartum participants and the aunt), following the chronological order of interviews. The interviews were conducted by the nursing student and first author under the direct supervision of the second author, a professor with extensive experience in this type of research. Both are affiliated with the federal university in the municipality where data collection occurred. The student received prior training to conduct the interviews and was continuously supervised to ensure data quality and clarify any questions throughout the process.
Two semi-structured interview guides were used: one for healthcare professionals and another for family members, each containing seven questions. Both instruments began with participant characterization questions, followed by questions specifically related to the study objectives.
For healthcare professionals: 1) Is HIV testing a routine practice in this institution for childbirth? Is there a protocol? 2) What are the reasons for requesting HIV testing for pregnant women? 3) What is the workflow for HIV testing requests for pregnant women? 4) How long does it take for the HIV test result to be released? Do you consider this time appropriate? 5) While awaiting the test result, how are newborns fed? 6) How long after birth is the baby placed for the first feeding? Do you consider this timing appropriate? 7) Has the need for HIV testing caused any interference with breastfeeding within the first hour of life? If so, how is this addressed by the team?
For family members: 1) Did you receive prenatal care during pregnancy? How many consultations were conducted? 2) Were tests for sexually transmitted infections performed during pregnancy? 3) Were you informed about HIV testing upon admission for childbirth? 4) How long did it take to receive the HIV test result? Do you consider this time appropriate? 5) While awaiting the test result, how was the baby fed? 6) How long after birth was the baby placed for the first feeding? Do you consider this timing appropriate? 7) Do you believe HIV testing had any impact on the initiation of breastfeeding?
Interviews were conducted once per participant, lasted an average of 10 minutes, and took place in a private location to ensure participant comfort and confidentiality. Data collection began in December 2024 and concluded in June 2025. Interviews were digitally recorded. Feedback on the interviews was not provided to participants, as postpartum women were discharged and most professionals worked in shifts, making follow-up difficult.
No pilot testing was conducted. Data collection was concluded based on two criteria: theoretical saturation, ensuring the breadth and recurrence of information(14–15); and textual corpus utilization in the IRAMUTEQ software (Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires), with a utilization index above 75% in the Descending Hierarchical Classification (DHC)(16). This approach ensured qualitative validity parameters, including exhaustiveness, representativeness, homogeneity, and relevance of the data(12).
Interviews were transcribed in Microsoft Word, and the textual corpus was saved as an unformatted text file (.txt) for processing in IRAMUTEQ, which provides various analytical tools such as Word Clouds, Similarity Analysis, CHD, and Correspondence Factor Analysis (CFA), all applied in this study. In CHD, active forms with a chi-square (χ²) value ≥ 3.84 (p < 0.05) were considered significantly associated with the classes. Words with p < 0.0001 were considered extremely significant(16). After processing in IRAMUTEQ, Thematic Analysis was performed, involving inference and interpretation of the findings by identifying the core meanings of text segments(17).
The study was approved by the Research Ethics Committee in accordance with Brazilian National Health Council Resolution No. 466/12(18), under Opinion No. 7.235.062 and CAAE 83001124.9.0000.8160. All participants signed the informed consent form.
RESULTS
A total of 35 individuals participated in the study. Among the 20 healthcare professionals, 12 were nurses (60.0%), five were nursing technicians (25.0%), and three were physicians (15.0%); 16 were female (80.0%) and four were male (20.0%). Regarding the workplace, nine professionals worked in the mother–baby unit (45.0%), six in the obstetrics ward (30.0%), and five in the delivery room/operating room (25.0%). The mean age of the professionals was 39 years, with an average of 13 years of experience in the field.
Among the family members, 14 postpartum women (93.3%) and one newborn’s aunt (6.7%) were interviewed. Regarding the type of delivery, nine women had a vaginal birth (60.0%) and six underwent a cesarean section (40.0%). The distribution of pregnancies was as follows: first pregnancy, six participants (40.0%); second pregnancy, five (33.3%); fourth pregnancy, one (6.7%); fifth pregnancy, two (13.3%); and sixth pregnancy, one (6.7%). The mean age of this group was 29 years.
Classical textual statistics were performed on a corpus of 35 texts, totaling 8,055 word occurrences, with an average of 230.14 occurrences per text. A total of 769 distinct lexical forms and 324 hapax legomena — words that appeared only once — were identified. In the frequency ranking, the ten most recurring words, highlighted in the Word Cloud (Figure 1), were: gente (people) (f = 92); teste (test) (f = 75); rápido (rapid) (f = 71); bebê (baby) (f = 67); hora (hour) (f = 65); exame (exam) (f = 62); resultado (result) (f = 52); vez (time/occasion) (f = 48); parto (delivery) (f = 48); and laboratório (laboratory) (f = 36).
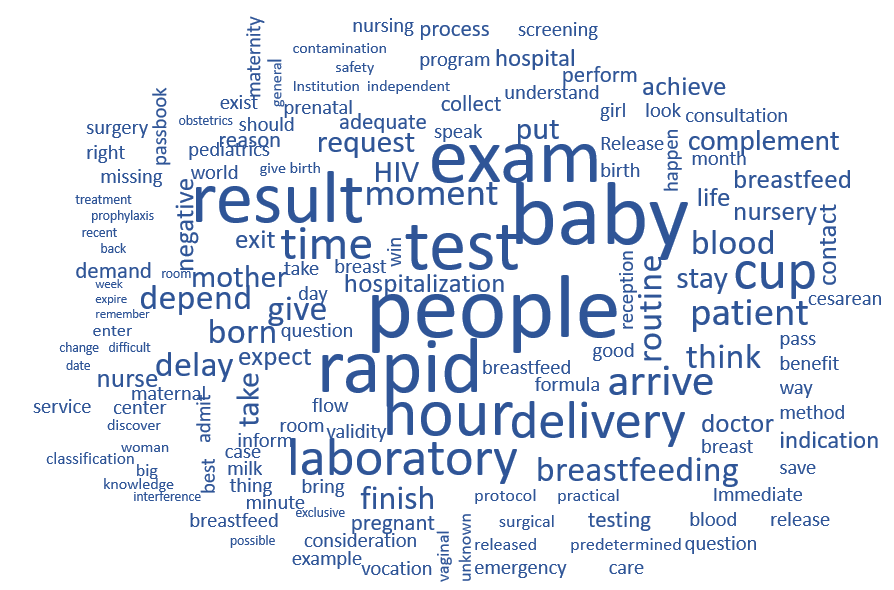
Source: IRAMUTEQ, 2025.
Figure 1 - Word cloud of the textual corpus. Rio das Ostras, RJ, Brazil, 2025
In the process of data interpretation, the most prominent word was “gente” (people), understood as the pronominal expression “a gente” (we), frequently used by healthcare professionals to collectively refer to the team in care activities. This expression appeared in statements such as: “a gente realiza o teste rápido” (“we perform the rapid test”), “a gente liga para o laboratório para verificar se o resultado saiu” (“we call the laboratory to check if the result is ready”), and “a gente informa aos familiares que é necessário aguardar o resultado para liberar a amamentação” (“we inform the family that it is necessary to wait for the result to allow breastfeeding”), among other constructions in the active voice. This linguistic choice reflects a collective and institutionalized practice, in which the team assumes shared responsibility for the procedures carried out, including the performance of the anti-HIV test upon admission, both in the rapid test modality and the laboratory test, depending on availability.
In the Similarity Analysis (Figure 2), the textual corpus was distributed into seven distinct clusters, connected by seven of the most frequently occurring words, represented by thicker lines. As in the Word Cloud, the central and most prominent word was “gente”, connecting to other relevant terms such as rápido (rapid), hora (hour), estar (to be), bebê (baby), exame (exam), and parto (delivery). From these main words, branches emerged to other terms addressed in the discourses.

Source: IRAMUTEQ, 2025.
Figure 2 - Similarity analysis of the textual corpus. Rio das Ostras, RJ, Brazil, 2025
In the blue cluster, centered on the word “gente” (people), branches were identified for the terms birth, test, nurse, know, patient, admit, request, flow, and prenatal care. This cluster highlights the healthcare professional as the main agent in the test request flow and in the care of both the pregnant woman and the mother–baby dyad. It also underscores the importance of prenatal care as an essential tool for identifying obstetric complications, which, when performed with quality, includes the necessary consultations and examinations.
The yellow cluster, centered on the word “rápido” (rapid), shows a thick connection with the blue cluster through the word “teste” (test), directly referring to the rapid test. There is strong interaction between these clusters, linked by terms representing different moments of care, such as laboratory, result, arrive, bring, testing, routine, request, doctor, and admission. These words describe the flow of the anti-HIV test request. When the rapid test is not performed upon admission, it is common for the physician to request a laboratory test. In this context, the laboratory plays a key role, being responsible for the collection, analysis, and release of results. When results are made available promptly, the pregnant woman is directed to delivery with the test recorded in her medical chart.
The red cluster, centered on the word “hora” (hour), with branches in delay, formula, breastfeed, wait, blood, negative, cup, and life, refers to the newborn’s first hour of life — known as the “golden hour”. During this period, the baby should receive colostrum due to its benefits for maternal and infant health. However, delays in releasing anti-HIV test results postpone breastfeeding, leading to the early use of formula administered with a dosing cup.
The pink cluster, centered on the word “bebê” (baby), presents branches in be born, mother, suck, breastfeeding, breast, release, and supplement. This highlights the need for breastfeeding not only for nutritional and immunological benefits but also for strengthening the mother–baby bond. The connection between the pink and blue clusters demonstrates, however, that early breastfeeding is frequently postponed due to the pediatrician waiting for the laboratory test results.
In the green cluster, centered on the word “estar” (to be), with branches in give, month, gestation, trimester, understand, team, cause, time, hospital, center, surgical, and shift, there is overlap with the fluorescent green cluster, centered on the word “exame” (exam), which branches into depend, HIV, pregnant woman, protocol, institution, and reason. Variability in practices is noted across teams depending on the shift, as some professionals validate tests from the last trimester while the majority require a new test upon admission.
Finally, the purple cluster, centered on the word “parto” (delivery), with branches in room, pediatrician, emergency, normal, same, prenatal booklet, take, consideration, contact, and skin, highlights the pediatrician as the professional responsible for authorizing breastfeeding in the delivery room. It also reflects variability in practices across shifts. Statements such as “depends on the team” and “it varies from pediatrician to pediatrician” reinforce this variation. Some pediatricians consider the prenatal booklet and prioritize skin-to-skin contact and early breastfeeding, while others do not adopt these best practices at birth.
The Descending Hierarchical Classification (DHC) (Figure 3) identified 236 text segments (TS), of which 200 were classified, representing 84.75% utilization. The corpus was divided into two independent blocks. The first, represented by Class 1 (red), corresponded to 42.0% (84/200) of TS. The second block was subdivided into Class 2 (green), with 26.0% (52/200), and Class 3 (blue), with 32.0% (64/200).
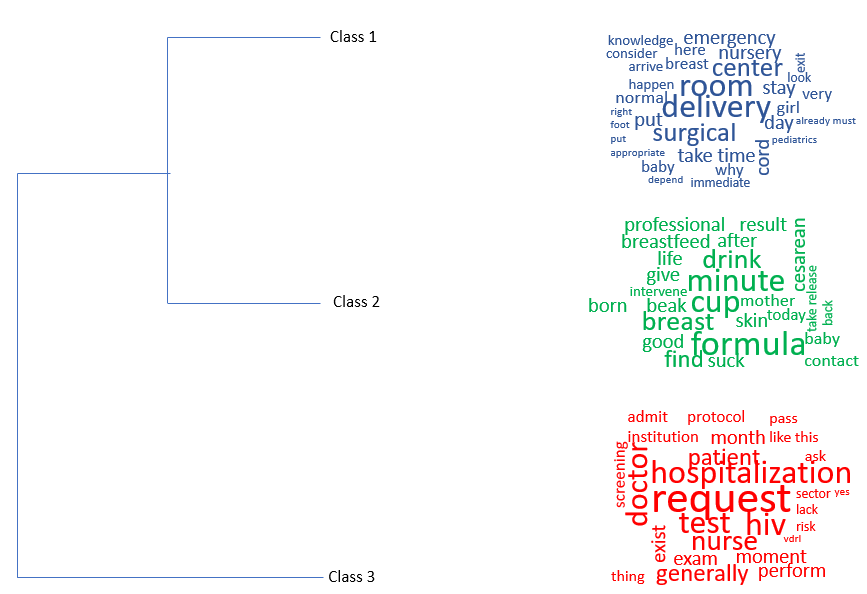
Source: IRAMUTEQ, 2025.
Figure 3 - Dendrogram of the textual corpus. Rio das Ostras, RJ, Brazil, 2025
There was a semantic distancing between Class 1, which primarily addressed the flow of anti-HIV test requests at the time of admission, and Classes 2 and 3, which were thematically closer, linking mode of delivery, breastfeeding within the first hour of life, and the use of infant formula in the nursery until the baby was reunited with the mother in the rooming-in ward. Delays in mother–baby contact were also associated with operating room implications related to cesarean delivery and postoperative care, including delays in performing or releasing the results of the anti-HIV test. The classes were named according to their predominant terms, as shown in Table 1.
Table 1 - Significant words and class names according to the Descending Hierarchical Classification (CHD). Rio das Ostras, RJ, Brazil, 2025
|
p-value |
Class 1 " Anti-HIV test request" |
Class 2 "Formula use and delayed breastfeeding" |
Classe 3 "Mode of delivery and barriers to skin-to-skin contact and breastfeeding" |
|
p < 0.0001 |
request, test, doctor, admission |
cup, minute, formula, think, take |
delivery, room, surgical, center, breastfeeding |
|
p < 0.05 |
patient, nurse, HIV, test, month, generally, moment, institution, case, protocol, admit, thus, request, reception, order, perform, practical, ask, rapid, routine, consideration, always, exist, health record, blood, recent, collect, testing, pregnant woman, lack, risk, VDRL, screening, yes, trimester, ward, through, expire, treatment, past, independent, including, nursing, unaware, contamination, classification, same |
breast, suck, ideal, skin, later, cesarean, soon, life, breastfeed, return, remove, professional, nipple, baby, good, hour, result, supplement, birth, give, manage, wait, contact, birth, today, mother, carry |
delay, remain, place, nursery, normal, day, emergency, breast, direct, girl, cord, there, happen, here, baby, immediate, foot, arrive, put, time, when, already, very, adequate, baby, because |
Source: prepared by the authors, 2025.
Class 1: Anti-HIV test request
The interview responses indicated that healthcare professionals exert direct influence over the process of requesting anti-HIV testing at admission for childbirth. It was observed that practices vary according to the work shift: some nurses perform the rapid test immediately upon admission, while others wait for a physician’s request for the laboratory test. Some professionals consider the validity of the last third-trimester test, whereas others disregard the records in the mother’s health booklet, requesting a new test.
It’s not just the rapid test; along with this anti-HIV test request, other tests are requested. (P30)
Generally, the HIV test is valid for three months, and if it’s not within that period, it is collected upon admission. (P21)
Regardless of the mother’s health booklet, whether she has it or not, it will be requested. (P16)
They take the booklet into account, but even so, they do it. The doctor requests it, the lab comes and collects it, then they bring it to the ward when the result is ready, and when it’s a rapid test, the nursing team does it right there on the spot. (P34)
They did it after she was born because they had forgotten to do it before. (M6)
Even when nurses take the initiative to perform testing during labor, obstacles such as scarcity of materials and unavailability of rapid tests are encountered. In this context, the laboratory flow becomes essential to reduce the time required for result release.
Yes, there is a rapid test, but the HIV one isn’t available. (P26)
I did the blood test, but not the rapid one. (M9)
I did the finger-prick test when I was admitted. (M3)
The mother should already enter the delivery room with the test done. She should have done it at admission. As soon as she gives birth, the rapid test should be done immediately in the delivery room so we can put the baby to breastfeed. (P22)
It was also observed that changes in the management team affected practices and guidance across departments, influenced by new administrative decisions. During the study period, partial adherence to rapid testing at admission was noted.
It’s a recent practice; they only started using the rapid test a few months ago. Not the entire team performs it because of lack of materials or lack of interest. (P35)
The rapid test is new to me. We usually do the laboratory test requested by the physician. We didn’t do the rapid test. The patient arrives, they collect it, she goes to the surgical center, the baby is born, and they wait 2–3 hours to breastfeed. (P24)
Currently, there is no protocol. There is a new coordination team instituting these processes. (P22)
Class 2: Formula use and delayed breastfeeding
In Class 2, the negative impact of prolonged waiting for laboratory test results became evident. When a blood test is requested for anti-HIV screening, breastfeeding is only authorized after the test result has been validated. This occurs because the institution requires that the result be properly attached to the patient’s medical record before permitting the initiation of breastfeeding, which sometimes takes more than an hour.
The delay in receiving rapid test results has directly interfered with establishing the mother-baby bond through breastfeeding within the first hour of life. As an alternative, the newborn is given infant formula in a small cup until the mother is cleared to start breastfeeding.
The laboratory timing for releasing this is about 2 hours. (P30)
Ideally, we should have the result of this test before birth. (P29)
The result interferes because of the delay. (P24)
He drank from the cup before he got to me. (M11)
It depends on the shift; it has happened here that the baby received formula three times because the result wasn’t ready. (P22)
The statements also highlighted the anxiety caused by delayed early breastfeeding, underscoring the importance of immediate and humanized contact between mother and baby during the first hour of life, as a way to strengthen the bond and promote the emotional well-being of the mother-infant dyad.
I was anxious for her to breastfeed on me. (M15)
The first contact, you know, I found it very distant. (M3)
Ideally, it should happen within the first hour, in a more humanized way for both mother and baby. (P19)
Class 3: Mode of delivery and barriers to skin-to-skin contact and breastfeeding
In Class 3, it was observed that, in this care context, the mode of delivery—whether vaginal or cesarean—emerged spontaneously in the statements as another factor affecting breastfeeding during the first hour of life. Cesarean deliveries were more frequently associated with delayed breastfeeding due to several factors, including anesthetic recovery, surgical suturing time, staff availability, and post-operative procedures. Additionally, there is often a delay in transferring the mother to the postpartum ward, which postpones contact with the baby, compounded by waiting for the anti-HIV test result.
Unfortunately, this does not happen, partly due to the hospital’s structural limitations. In cesarean deliveries, the baby takes more than one hour to have first contact and the first breastfeeding. In a vaginal birth, if the patient already has the test result, we can do it. (P29)
He drank formula on the first night because I was in pain from the cesarean. (M1)
About an hour and a half, roughly, it took because it was a cesarean. (M3)
Another aspect mentioned concerns the institution’s physical and organizational structure. All deliveries take place in the operating room, increasing the workload of the unit. This structural limitation represents an additional barrier to breastfeeding within the first hour, compounded by some professionals who do not routinely incorporate these practices into their workflow.
Because there is no proper structure, even normal deliveries occur in the operating room, and the baby is not immediately placed for breastfeeding. (P30)
In the delivery room, whether the child was born via cesarean or vaginally, we do not have the habit of putting the baby to the breast immediately. This varies greatly from one pediatrician to another. It’s not just because of the test result. (P16)
It’s not a standard practice here, but some obstetricians request it, depending also on having all the tests ready. (P20)
Participants also expanded their statements on the reasons for delays in early breastfeeding, linking them not only to waiting for anti-HIV test results but also to the mode of delivery and structural factors within the institution, which act synergistically to exacerbate the problem.
From the Correspondence Factor Analysis (CFA), it was possible to observe that Classes 1, 2, and 3 were positioned in distinct planes, unlike in the Descending Hierarchical Classification (DHC), where only Class 1 showed differentiation. This spatial separation reflects a clear lexical distinction along the X and Y axes in the factorial plane, allowing for more precise thematic interpretation.
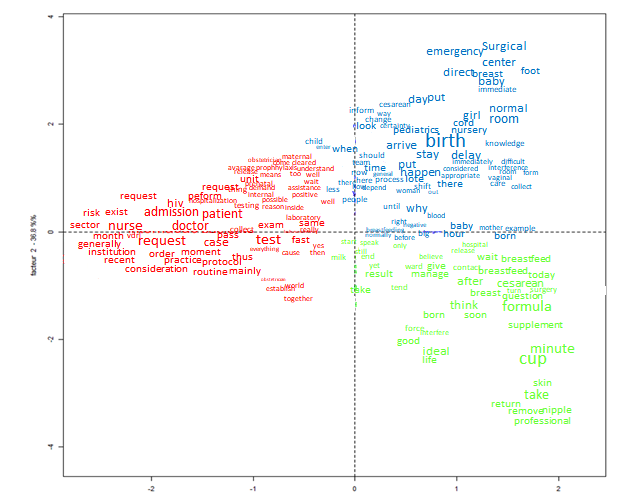
Source: IRAMUTEQ, 2025.
Figure 4 - Correspondence factor analysis (CFA) of the textual corpus. Rio das Ostras, RJ, Brazil, 2025
In the first and third quadrants, the color red stood out, representing the healthcare professionals as well as the flow of anti-HIV test requests, incorporated as part of the institutional routine of the studied unit. This routine sometimes delays the initiation of breastfeeding, confirming the findings previously described. In the second quadrant, the color blue was prominent, associated with deliveries performed in the operating room, regardless of the mode of birth, reflecting the lack of adequate hospital infrastructure for vaginal deliveries, in addition to pediatric practices adopted immediately after birth, which interfere with breastfeeding during the first hour of life. In the fourth quadrant, the color green highlighted the delay in initiating breastfeeding, which resulted in the use of complementary nutrition through infant formula.
DISCUSSION
The results demonstrated that anti-HIV testing during hospital admission for childbirth directly interferes with breastfeeding within the first hour of life by causing delays in the initiation of this practice. One contributing factor to this delay is the variation in practices among on-duty professionals: while some perform rapid tests immediately, with results available within 30 minutes, others wait for a physician to request a laboratory test, which may take up to three hours depending on laboratory workflow. A Brazilian study corroborates these findings, highlighting discrepancies in clinical practices that affect the initiation of breastfeeding(19).
Despite the prioritization of rapid testing by some nurses during labor, the scarcity of resources, such as the tests themselves, represents a frequent obstacle. Accordingly, international evidence emphasizes that recognizing barriers to testing is an essential step toward overcoming them, aiming to improve anti-HIV testing coverage across diverse settings(20), including maternity wards, ensuring safe and timely care.
In the absence of rapid testing, an efficient laboratory workflow becomes crucial to guarantee timely care. Rapid tests provide the advantage of immediate results without requiring laboratory processing; therefore, when available, it is imperative that healthcare professionals integrate them into routine practice as a valuable tool for early detection of infections(21).
Because the institution only authorizes breastfeeding after the negative result is attached to the patient’s record, the initial mother–baby bonding may be compromised, leading to delayed breastfeeding beyond the first hour of life. A study conducted in the same maternity ward showed that all mothers interviewed had “non-reactive” results, and while awaiting authorization to breastfeed, the newborns were fed formula using a cup(11). However, receiving alternative milk in the maternity ward is associated with a fourfold increased risk of early weaning compared to exclusively breastfed infants, as reported in a study conducted in Bahia(22).
Another relevant factor was the mode of delivery, as cesarean sections emerged as an additional barrier to breastfeeding in the first hour of life. Supporting this finding, an Ethiopian meta-analysis indicated that cesarean delivery is associated with approximately a 79% reduction in early breastfeeding initiation compared to vaginal birth(23). A study conducted in Recife found that cesarean delivery hinders the initiation of breastfeeding due to anesthesia, postoperative care, and delays in skin-to-skin contact and transfer to the maternity ward(24). When combined with delays in obtaining anti-HIV test results, these factors further exacerbate delayed early breastfeeding, highlighting the importance of timely testing and organized care flows.
Management changes led to the adoption of new institutional routines, such as the partial implementation of rapid testing during the study period. This variability demonstrated that different workflows may coexist even within a single service. Therefore, protocols and training are needed to standardize professional practices, given that a Brazilian study identified the main risk factor for not initiating breastfeeding within the first hour as receiving the rapid test result after delivery(25), a situation that requires revision.
When laboratory testing is used, it is essential that results are made available promptly to avoid compromising the early initiation of antiretroviral therapy and breastfeeding, when indicated(5). Thus, anti-HIV testing, while a best practice, should not limit another equally essential practice: breastfeeding within the first hour of life, as recommended by the fourth step of the Baby-Friendly Hospital Initiative, which advises immediate skin-to-skin contact between mother and infant for at least one hour after birth(26).
As this was a qualitative investigation with a convenience sample, the results cannot be generalized, as they reflect the experiences of participants from a single maternity ward, which constitutes a limitation of the study. Furthermore, the absence of transcript feedback to participants, due to operational constraints, limited validation of the statements. To minimize these limitations, efforts were made to ensure the greatest possible diversity of participant profiles, as well as rigor in the conduct, transcription, processing, and analysis of the interviews, aiming to enhance the depth, credibility, and legitimacy of the findings within the qualitative framework. The entire process was mediated through researcher validation, ensuring a comprehensive understanding of the phenomenon under investigation.
The findings of this study revealed that anti-HIV testing during hospital admission for childbirth directly interferes with breastfeeding within the first hour of life, causing delays in the initiation of this practice. Although it constitutes an institutional routine, its implementation varies according to the practices adopted by healthcare professionals and the type of test used (rapid or laboratory) and is sometimes affected by the scarcity of material resources. This dynamic hinders early breastfeeding, often resulting in the use of formula milk.
It is necessary to rethink care flows so that anti-HIV testing during admission for childbirth does not become a barrier to breastfeeding within the first hour of life, allowing both practices to occur in an integrated, safe, and timely manner. In this way, the study contributes to nursing practice by emphasizing the need for critical and proactive engagement of nurses in the perinatal context, particularly regarding the planning and implementation of rapid testing at admission, ensuring both HIV prevention and the promotion of early breastfeeding.
CONFLICT OF INTERESTS
The authors declare no conflict of interest.
REFERENCES
1. Clausen M. Brjóstagjöf og brjóstamjólk er heilsuávinningur fyrir móður og barn. Laeknabladid. 2023;109(12):549. https://doi.org/10.17992/lbl.2023.12.770
2. Lucchese I, Góes FGB, Soares IA de A, Goulart M de C e L, Silva ACSS da, Pereira-Ávila FMV. Breastfeeding in the first hour of life in a city in the countryside of Rio de Janeiro: associated factors. Esc Anna Nery. 2023;27:e20220346. https://doi.org/10.1590/2177-9465-EAN-2022-0346en
3. Brasil. Senado Federal. Estatuto da Criança e do Adolescente: Lei nº 8.069/1990 [Internet]. 8. ed. Brasília (DF): Senado Federal, Coordenação de Edições Técnicas; 2025 [cited 2025 Jul 20]. Available from: https://www2.senado.leg.br/bdsf/bitstream/handle/id/696197/Estatuto_crianca_adolescente_8ed_2025.pdf
4. Nachman S, Aldrovandi G. Breastfeeding in the United States Among Women With HIV: Con Viewpoint. Clin Infect Dis. 2024;78(6):1629-1631. https://doi.org/10.1093/cid/ciad778
5. Brasil. Ministério da Saúde. Protocolo clinico e diretrizes terapêuticas para prevenção da transmissão vertical de HIV, sífilis e hepatites virais [Internet]. Brasília (DF): Ministério da Saúde; 2022 [cited 2025 Jul 20]. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_clinico_hiv_sifilis_hepatites.pdf
6. Brasil. Ministério da Saúde. Manual técnico para o diagnóstico da infecção pelo HIV em adultos e crianças. Ministério da Saúde [Internet]. Brasília (DF): Ministério da Saúde; 2018 [cited 2025 Jul 20]. Available from: https://www.gov.br/aids/pt-br/central-de-conteudo/publicacoes/2018/manual_tecnico_hiv_27_11_2018_web.pdf
7. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde e Ambiente. Boletim Epidemiológico HIV/Aids 2024 [Internet]. Brasília: Ministério da Saúde; 2024 [cited 2025 Jul 20]. Available from: https://www.gov.br/aids/pt-br/central-de-conteudo/boletins-epidemiologicos/2024/boletim_hiv_aids_2024e.pdf
8. Sundar KG, Yang LZ, Cambou MC, Varella IRS, Melo MG, Segura ER, et al. Prompt Initiation of Maternal Antiretroviral Therapy After HIV Seroconversion in Pregnancy Effectively Prevents Vertical Transmission and Other Adverse Infant Outcomes. Pediatr Infect Dis J. 2025;44(1):40-43. https://doi.org/10.1097/INF.0000000000004562
9. Veiga AC da, Medeiros L da S de, Backes DS, Sousa FGM de, Hämel K, Kruel CS, et al. Interprofessional qualification of prenatal care in the context of primary health care. Cien Saude Colet. 2023;28(4):993-1002. https://doi.org/10.1590/1413-81232023284.14402022EN
10. Monteiro JV, Costa LMO, Viana ILR de S, Souza MV de C, Ferreira LE da C, Silva JLA. Assistência pré-natal como ferramenta profilática de intercorrências obstétricas: uma revisão integrativa. Saberes Plur. 2023;7(2):e132691. https://doi.org/10.54909/sp.v7i2.132691
11. Góes FGB, Sá ACS de, Souza AN, Soares IA de A, Lucchese I, Terra NO. Factors intervening in breastfeeding in the first hour of life on the maternity ward. Rev. Enferm. UERJ. 2022;30(1):e698387. https://doi.org/10.12957/reuerj.2022.69838
12. Minayo MC de S. Qualitative analysis: theory, steps and reliability. Cien Saude Colet. 2012;17(3):621-626. https://doi.org/10.1590/S1413-81232012000300007
13. Souza VR dos S, Marziale MHP, Silva GTR, Nascimento PL. Translation and validation into Brazilian Portuguese and assessment of the COREQ checklist. Acta Paul Enferm. 2021;34:eAPE02631. https://doi.org/10.37689/acta-ape/2021AO02631
14. Nascimento L de CN, Souza TV de, Oliveira IC dos S, Moraes JRMM de, Aguiar RCB de, Silva LF da. Theoretical saturation in qualitative research: an experience report in interview with schoolchildren. Rev Bras Enferm. 2018;71(1):228-233. https://doi.org/10.1590/0034-7167-2016-0616
15. Falqueto JMZ, Hoffmann VE, Farias JS. Saturação teórica em pesquisas qualitativas: relato de uma experiência de aplicação em estudo na área de administração. Revista de Ciências da Administração. 2018;20(52):40-53. https://doi.org/10.5007/2175-8077.2018V20n52p40
16. Góes FGB, Santos AST dos, Campos BL, Silva ACSS da, Silva LF da, França LCM. Utilização do software IRAMUTEQ em pesquisa de abordagem qualitativa: relato de experiência. Rev. enferm. UFSM. 2021;11:e63. https://doi.org/10.5902/2179769264425
17. Minayo MC de S. O desafio do conhecimento: pesquisa qualitativa em saúde. 14. ed. São Paulo: Hucitec; 2014.
18. Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Resolução nº 466, de 12 de dezembro de 2012. Aprova as diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Diário Oficial da União. 2018; Jul. 16.
19. Oliveira MIC, Silva KS, Gomes DM. Factors associated with submission to HIV rapid test in childbirth care. Cien Saude Colet. 2018;23(2):575-584. https://doi.org/10.1590/1413-81232018232.11612016
20. Wong NS, Tang W, Miller WC, Ong JJ, Lee SS. Expanded HIV testing in non-key populations – the neglected strategy for minimising late diagnosis. Int J Infect Dis. 2024;138:38-40. https://doi.org/10.1016/j.ijid.2023.11.034
21. Barbosa GAR de M, Dias PC, Silveira GC, Lopes A. A importância da enfermagem na utilização de testes rápidos para diagnóstico de doenças infectocontagiosas. Revista InterSaúde. 2021 [cited 2025 Jul 20];1(4):47-58. Available from: http://portal.fundacaojau.edu.br:8077/journal/index.php/revistasanteriores/article/view/435
22. Unfried AGC, Paixão GP do N, Fraga CD de S, Oliveira JD, Cavalcante Neto JL. Neonatal factors associated with early weaning in a municipality in Bahia, Brazil: a cross-sectional study. Rev Esc Enferm USP. 2024;58:e20240091. https://doi.org/10.1590/1980-220X-REEUSP-2024-0091en
23. Getaneh T, Negesse A, Dessie G, Desta M, Temesgen H, Getu T, et al. Impact of cesarean section on timely initiation of breastfeeding in Ethiopia: a systematic review and meta-analysis. Int Breastfeed J. 2021;16(1):51. https://doi.org/10.1186/s13006-021-00399-9
24. Silva JLP da, Linhares FMP, Barros A de A, Souza AG de, Alves DS, Andrade P de ON. Factors associated with breastfeeding in the first hour of life in a baby-friendly hospital. Texto & Contexto Enferm. 2018;27(4):e4190017. https://doi.org/10.1590/0104-07072018004190017
25. Oliveira MIC de, Silva KS da, Gomes Junior SC, Fonseca VM. Delivering rapid HIV tests results after delivery: a threat to breastfeeding at birth. Rev Saude Publica. 2010;44(1):60-69. https://doi.org/10.1590/s0034-89102010000100007
26. Santos FS, Ribeiro NG, Siqueira LS, Aragão FBA, Pascoal LM, Santos Neto M. A prática do quarto passo da iniciativa hospital amigo da criança em maternidade de referência. Enferm. actual Costa Rica (Online). 2021;(40). https://doi.org/10.15517/revenf.v0i40.42546
Submission: 20-Jul-2025
Approved: 12-Aug-2025
Editors:
Rosimere Ferreira Santana (ORCID: 0000-0002-4593-3715)
Geilsa Soraia Cavalcanti Valente (ORCID: 0000-0003-4488-4912)
Diego Pereira Rodrigues (ORCID: 0000-0001-8383-7663)
Corresponding author: Mariana Viana Toledo (marianavianatoledo@id.uff.br)
Publisher:
Escola de Enfermagem Aurora de Afonso Costa – UFF
Rua Dr. Celestino, 74 – Centro, CEP: 24020-091 – Niterói, RJ, Brazil
Journal email: objn.cme@id.uff.br
|
AUTHORSHIP CONTRIBUTIONS |
|
Study conception: Toledo MV, Góes FGB. Data acquisition: Toledo MV, Góes FGB. Data analysis: Toledo MV, Góes FGB, Ávila FMVP, Silva MA, Nunes NGF, Silvério LZA. Data interpretation: Toledo MV, Góes FGB, Ávila FMVP, Silva MA, Nunes NGF, Silvério LZA. All authors are responsible for drafting the manuscript, critically revising its intellectual content for the final published version, and ensuring the study’s accuracy and integrity with regard to ethical, legal, and scientific aspects. |
