
EXPERIENCE REPORT
IMPLEMENTATION OF A NAVIGATION PROGRAM FOR PATIENTS UNDERGOING COMPLEX SPINAL SURGERY: AN EXPERIENCE REPORT
Giovana Loreto Nunes1, Daniela Corrêa da Silva de Farias2, Fernanda Felipe Pautasso3, Amanda Kohn4, Bárbara Ribeiro Waengertner5, Rita Catalina Aquino Caregnato6
1 Universidade Federal de Ciências da Saúde de Porto Alegre. Porto Alegre, RS, Brazil. ORCID: 0000-0002-4704-6335. E-mail: giovanaloreton@gmail.com
2 Santa Casa de Porto Alegre. Porto Alegre, RS, Brazil. ORCID: 0009-0003-4142-5419. E-mail: farias_daniela@hotmail.com
3 Santa Casa de Porto Alegre. Porto Alegre, RS, Brazil. ORCID: 0000-0001-8791-9308. E-mail: nursepautasso@outlook.com
4 Universidade Federal de Ciências da Saúde de Porto Alegre. Porto Alegre, RS, Brazil. ORCID: 0009-0007-9602-5665. E-mail: enfamandakohn@gmail.com
5 Universidade Federal de Ciências da Saúde de Porto Alegre. Porto Alegre, RS, Brazil. ORCID: 0009-0004-3572-0590. E-mail: barbarawaen@outlook.com
6 Universidade Federal de Ciências da Saúde de Porto Alegre. Porto Alegre, RS, Brazil. ORCID: 0000-0001-7929-7676. E-mail: ritac@ufcspa.edu.br
ABSTRACT
Objective: To describe the trajectory for the implementation of a Navigation Program for patients undergoing complex spinal surgery. Method: Descriptive study, an experience report, carried out in a large hospital located in Southern Brazil. Results: Implementation took place between September 2023 and February 2024. The trajectory included the structuring of workflows, training of the navigator nurse, and adherence to institutional policy. Central strategies involved conducting multidisciplinary boards for the individualization of patient care. We observed improved rehabilitation, pain control, and reduction of postoperative complications. Early detection of risks increased the perception of safety among navigated patients. Conclusion: The implementation of the Navigation Program in complex spinal surgeries has proven to be an effective strategy in organizing care and ensuring perioperative patient safety. The experience demonstrates that the nurse's leadership, combined with managerial and clinical competencies, is the key element for the program's sustainability and for integrated care centered on the patient's individuality. The model proves to be applicable and inspiring for the development of new initiatives in highly complex care pathways.
Descriptors: Patient Navigation; Nurses; Program; Surgical Procedures; Orthopedic Procedures.
|
How to cite: Nunes GL, Farias DCS, Pautasso FF, Kohn A, Waengertner BR, Caregnato RCA. Implementation of a navigation program for patients undergoing complex spinal surgery: an experience report. Online Braz J Nurs. 2026;25(1):e20266863. https://doi.org/10.17665/1676-4285.20266863 |
What is already known:
Major procedures, such as complex spinal surgery, involve complex processes ranging from the management of special materials to rigorous clinical management, which can lead to communication failures and delays in the surgical workflow.
International literature and national studies demonstrate that patient navigation reduces care barriers, decreases waiting time for treatment, and improves patient satisfaction through coordinated care.
Patient navigation is recognized as a nursing competency in Brazil, consolidated by COFEN Resolution No. 735/2024, which defines the responsibilities of the nurse navigator in managing the patient's journey across different care pathways.
What does this article add:
The report describes the practical application of navigation in a non-oncological care pathway, demonstrating the versatility of the model and its ability to optimize outcomes in highly complex surgical specialties.
The study details the use of multidisciplinary meetings as a central management tool, allowing for the individualization of the care plan for complex cases and the anticipation of operative risks.
The article highlights that the nurse navigator's role not only improves clinical indicators but also ensures the sustainability of the program through the fluidity of institutional processes and their leading role in care management.
INTRODUCTION
Internationally, Patient navigation has been used to achieve better clinical outcomes. Patient navigation is an evidence-based practice developed in the United States in 1990 by physician Harold Freeman at Harlem Hospital in New York(1, 2). It is defined as a systematized process that assesses patient needs, planning and implementing actions to promote care focused on helping patients overcome barriers that hinder their access to healthcare. This process is carried out by a professional called a patient navigator, often nurses(3).
Considered recent in Latin America, the first study published in Portuguese was only in 2018. A Navigation Program for patients with head and neck cancer was structured for the Brazilian reality, along with the Navigation Needs Assessment Scale (NNAS), and had its first article published in 2020(4). Through the approval of Law No. 14,450, in September 2022, which created the “National Patient Navigation Program for People with Malignant Breast Neoplasms”, patient navigation was regulated(5). Law No. 14,758, in December 19th, 2023, established the National Policy for Cancer Prevention and Control within the scope of the Unified Health System (SUS) and the National Program for Navigation of People Diagnosed with Cancer, covering navigation for different types of cancer(6) and, on February 4th, 2025, Ordinance GM/MS No. 6,592 was published, expanding navigation to patients suspected of having cancer and not just those already diagnosed, within the scope of the SUS(7).
Back pain is common and affects most people at some point in their lives, becoming a frequent health problem(8,9). According to the Ministry of Health, pain is an unpleasant sensation that arises from actual tissue damage or the threat of possible damage, considered subjective as it can be both physical and emotional, and each individual is different based on previous experiences(10). Back pain is one of the main causes of work absenteeism, disability and reduced functionality, precisely because it generates a decrease in mobility(8, 9). Therefore, chronic back pain should be monitored, as in addition to being a health problem, it negatively influences work, the economy, quality of life and health services(11).
Depending on the diagnosis, the patient may be directed to conservative treatment, with lifestyle modifications, physiotherapy and medication, however, when this treatment does not show significant results, causing chronic pain or when there is a progressive neurological deficit, surgical intervention becomes an option(8, 12). Spinal surgery has different types of approaches and different degrees of invasiveness, ranging from simple surgeries to highly complex surgeries(13). Spinal fusion, a surgical procedure that aims to stabilize segments of the vertebral column by fusing two or more vertebrae, has a record of 98,798 surgeries performed by the SUS between 2015 and 2024(14). Among the spinal fusions, there are those that are considered complex surgeries, but literature has not provided an exact number of how many there are.
Studies indicate that patients undergoing minimally invasive surgeries experience less pain in the immediate postoperative period and a faster recovery of mobility(15). Considering the complexity of spinal surgeries, it is important that the patient receives adequate guidance and follow-up for their best recovery, regardless of the type of surgical approach they have undergone.
In the search conducted on the navigation of patients undergoing spinal surgery, only one study published, in 2021 in the United States, was found, which briefly addresses the navigation of patients undergoing this type of surgery, not focusing on cancer patients(16). Given that patient navigation has been implemented in Brazil, even though its focus is on cancer patients, the need for navigation for patients undergoing complex spinal surgery has been observed, due to the need to understand the patient as a whole, providing adequate and individualized pre- and post-operative care, enabling a rapid recovery for a timely return to work(17). Therefore, the objective of this article is to describe the trajectory for the implementation of a Navigation Program for patients undergoing complex spinal surgery.
METHOD
This is a descriptive study, an experience report, presenting a lived experience expressed in written form(18). The field of action was a large hospital located in Porto Alegre, Rio Grande do Sul, Brazil, which serves patients from the Unified Health System, Complementary Health System and private patients. The implementation of the Navigation Program for patients undergoing complex spinal surgery was developed from September 2023 to February 2024, and it continues happening up to the present.
This study describes the professional experience of one of the authors of this article. The results are described in stages, maintaining the chronological order of events and respecting the description of processes and workflows. As this is a report of professional experience, which did not involve direct data collection from human beings for research purposes, intervention or exposure of identifiable information of participants, submission to the Research Ethics Committee was waived, in accordance with the provisions of CNS Resolution No. 510, of April 7, 2016(19).
RESULTS
The implementation process for patient navigation for those undergoing complex spinal surgery took place in a hospital where patient navigation has been a reality since 2022, with programs directed towards oncology care pathways, namely: breast cancer, lung cancer, prostate cancer, hepatocellular carcinoma, and oncology patients undergoing chemotherapy. Therefore, patient navigation programs in the hospital units should follow the basic structure of the Institutional Navigation Program policy, as shown in Figure 1.

Figure 1 – Institutional Navigation Program. Porto Alegre, RS, Brazil, 2025
Source: prepared by the authors, 2025.
In addition to following basic institutional policy, the Navigation Program should follow the navigation process, which consists of: assessment of patient needs; development of the navigation plan; implementation of the navigation plan; follow-up; reassessment of needs with adjustments to the plan; and discharge from the navigation program. In this way, there was a basis for implementing navigation for patients undergoing complex spinal surgeries(20).
For the inclusion of patients in the navigation program, the following criteria were defined: patients eligible for complex spinal surgical procedures, with all treatment being carried out at the institution where navigation would take place. Complex spinal procedures were considered to be: surgeries with three or more levels of fusion, spinal deformities (reconstructive surgery), tumors, severe myelopathies (mJOA > 12), significant comorbidities, or cases that the surgeon considered complex.
It was defined that the NNAS would be used to assess patients' need for navigation, an instrument that allows patients to be classified into navigation levels, based on six biopsychosocial and cultural criteria that indicate a greater or lesser need for accompaniment(4) Applied by the nurse navigator in the first care of patients undergoing complex spinal surgery, its objective is to identify the real need for recommended support, providing a basis for the development of the individualized navigation plan by the nurse navigator(4).
The nurse navigator responsible for these patients underwent institutional training before starting her work in this program. In this sense, the training took place gradually, combining theoretical and practical moments, since she did not have practical experience in this area. Thus, the theoretical stage covered the principles of patient navigation, the duties of the nurse navigator and the use of the program's instruments in the navigation process. Then, the practical stage was carried out through direct accompaniment by a nurse navigator already working in oncology line programs, in field activities, for 30 days. This allowed for greater familiarity with the care routine and favored the consolidation of learning in practice.
The development of the Navigation Program for this audience took into account the need to retain patients served through health insurance plans and to equalize care for patients served by the SUS (Brazilian Public Health System). In addition, neurosurgery, which includes spinal surgeries, is one of the institution's strategic care lines, included in outcome monitoring.
For a better discussion of these cases, boards for complex cases were created, developed from the need to improve the outcomes of complex spinal surgeries performed at the hospital in question. The boards consist of meetings that occur with some regularity, with the objective of defining the best treatment strategy for the patient. In these meetings, specialists from various health areas analyze the clinical picture, taking into account each particularity. The multidisciplinary approach is essential, especially for complex cases that do not align with standard protocols. Through this discussion, the group is able to determine a more effective course of action and personalize the treatment, optimizing the combination of interventions, always respecting the patient's history and individual choices(21).
The boards developed for complex spinal cases involved a multidisciplinary group, composed of pain specialists, anesthesiologists, infectious disease specialists, general practitioners, neurosurgeons, nurses, physical therapists, and social workers. The meetings were held monthly, with the first meeting on September 21, 2023, each lasting an average of 50 minutes, in which complex spinal cases were discussed, including a multidisciplinary assessment of surgical risks, review of the surgical plan, perioperative care, multidisciplinary management before hospitalization, and discussion of the outcomes of cases that were operated on in the previous month. The boards were held with a frequency of one meeting per month, with the last meeting held on February 29, 2024, and 24 complex spinal cases were discussed.
Concurrently with the boards, meetings were held to structure the program, as shown in Figure 2. The first meeting consisted of a general organization of the program and definition of the next meetings. Among the training activities, defined in the second meeting, was the accompaniment of the nurse, along with neurosurgeons and residents, in outpatient consultations and postoperative visits, both in inpatient units and in ICUs, in addition, case discussions were held. This training took place during the month of October of 2023. In the third meeting, a flyer on postoperative care was developed and there was a discussion about the pain protocol.
In the fourth meeting, the first discussion on complications arising from complex spinal surgeries took place, in which the importance of systematic monitoring of possible complications, the need for adequate symptom management and early assessment of these events was discussed, focusing on reducing risks and favoring interventions for timely outcomes. The role and importance of the nurse navigator in this process was also highlighted, evidencing the benefits of their continuous monitoring for patient safety, early identification of complications and the qualification of care throughout, especially, the postoperative period. At that time, it was also agreed how the information feed flow would work in REDCap, a digital platform for collecting, managing, and disseminating research data. This platform contains information about complications that could occur at three points: intraoperatively; during hospitalization, understood as the period after surgery until the time of hospital discharge; and from the time of hospital discharge until three months after that.
In the fifth meeting, in which aspects related to the care and integration of the multidisciplinary team were discussed, it was agreed that the nurse would signal to the physiotherapist the patients who needed evaluation. In this way, patients would have an early referral for the preparation of their postoperative rehabilitation.
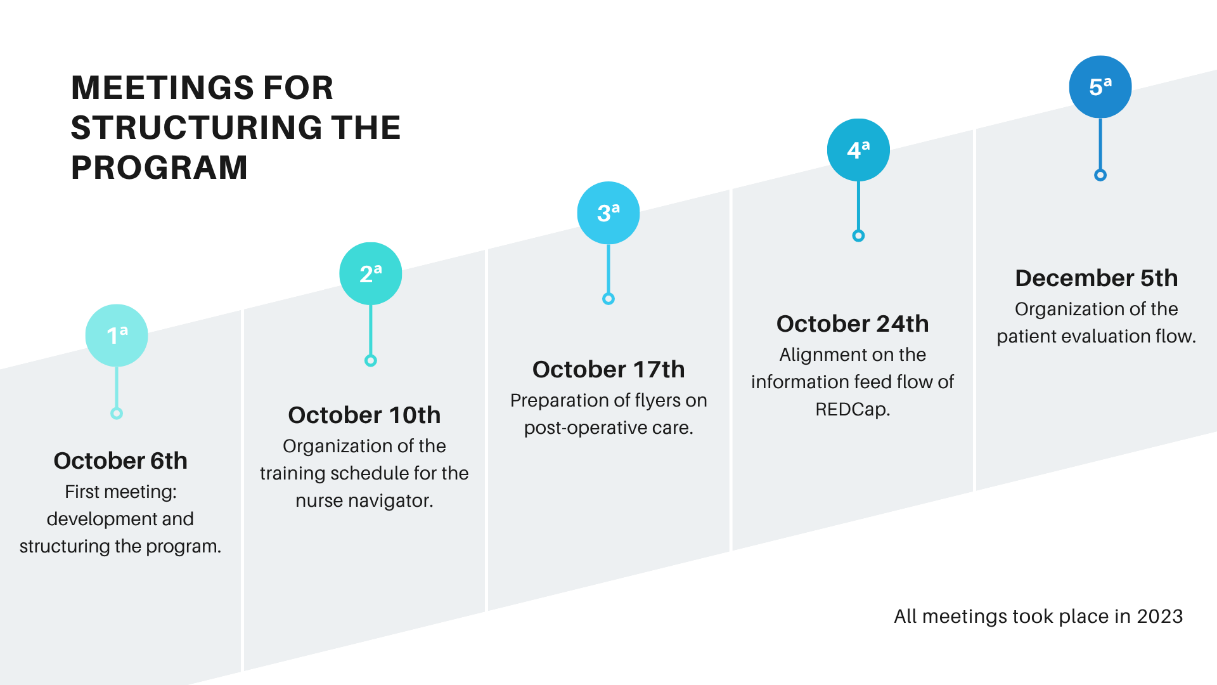
Figure 2 – Chronology of the Meetings for Structuring the Navigation Program. Porto Alegre, RS, Brazil, 2025
Source: prepared by the authors, 2025.
Following the alignment and planning meetings, the inclusion of patients in the Navigation Program and the navigation flow proceeded as shown in Figure 3. The navigation flow consists of six steps: the attending physician's indication of a potential patient to be navigated; the first contact between the Nursing Navigator and the patient indicated by the physician, in order to understand and assess the need for navigation; application of the NNAS scale when the surgical procedure is scheduled and the definitive inclusion of the patient in the care pathway; the actual navigation of the patient, both before and after surgery; the patient is discharged from the hospital by the medical team and continues in the Navigation Program; and finally, the discharge from the Navigation Program by the Nurse Navigator, which varies in time according to the individual needs of each patient.
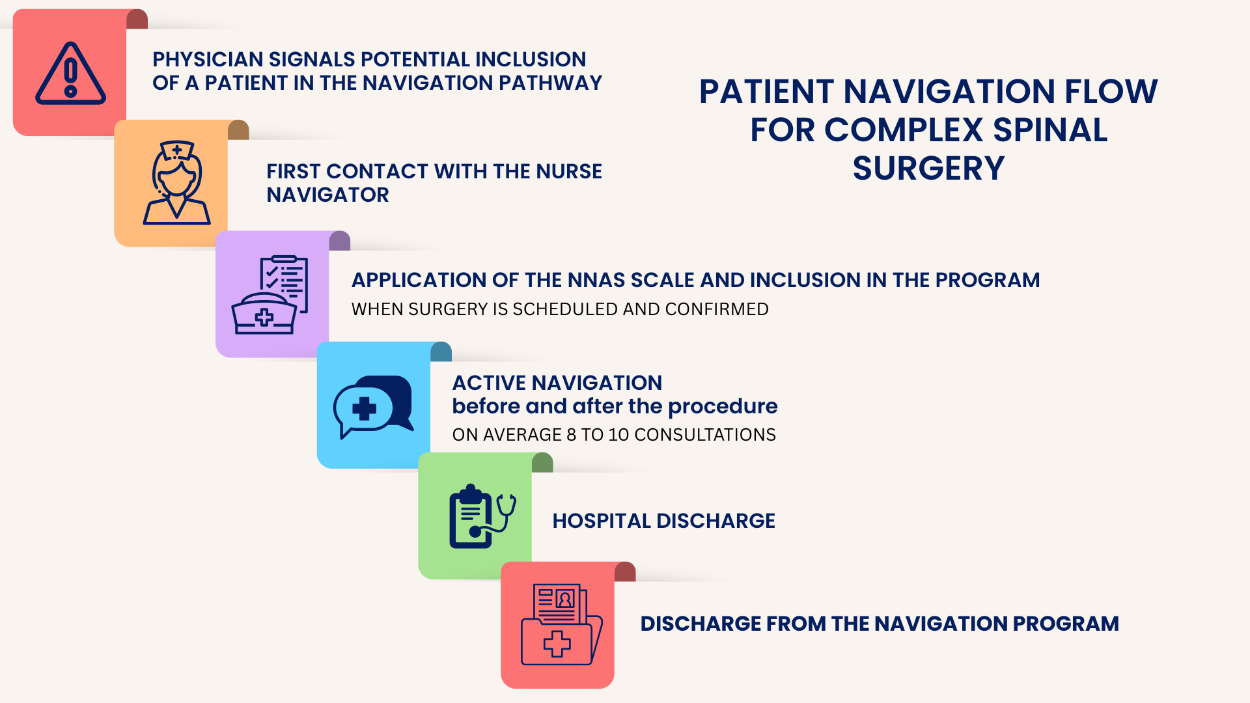
Figure 3 – Flowchart of the Navigation Program for a patient undergoing complex spinal surgery. Porto Alegre, RS, Brazil, 2025
Source: prepared by the authors, 2025.
With the implementation of navigation for patients undergoing complex spinal surgery, it was possible to: observe better postoperative rehabilitation; reduce complications; improve pain control; and detect risks early. In this way, nurses can assist patients in decision-making, which has reduced emergency room visits, generating a greater sense of security and confidence in these patients.
DISCUSSION
A recent study demonstrated that distinct areas of oncology are also conducting patient navigation, such as navigating patients with chronic communicable diseases (HCV and HIV+), chronic non-communicable diseases (diabetes, inflammatory bowel disease, and other complex chronic diseases), and care transition(22,23). Thus, the inclusion of the Navigation Program for patients undergoing complex spinal surgery is a promising investment for the institution, considering that navigation aims to reduce or even eliminate inconsistencies in access and treatments. Through the multidisciplinary team, the patient receives a more critical and individualized look, making it possible to identify the difficulties these patients were facing.
With the structuring of the navigation program, the care focus was directed towards improving the quality of care, ensuring effective reception and comprehensive support throughout the patient's entire therapeutic journey. The structuring of the program aligns with the literature, which indicates the need to establish policies, procedures, guidelines, and processes to ensure the formalization and effectiveness of the Navigation Program in health institutions(24). The Navigation Program for spinal surgery patients can be an impetus for other programs to be created and developed. Patient navigation in different areas and specialties of health can provide several benefits for the patient and the health institution, for this reason, the implementation of navigation and the development of studies on the subject should continue.
Patient navigation can be done by any professional and even by lay people, but it is of utmost importance that the navigator is someone trained and who has an appropriate profile to deal with the demands and responsibilities that this position requires(25). But patient navigation, with the nurse as the main navigator, has demonstrated effectiveness in the care and assistance provided to the patient, making this care individualized and coordinated, ensuring that their peculiarities and needs are met and valued. Thus, obtaining positive results for those patients included in the navigation program, aligns with the literature showing that nurse-led navigation programs are on the rise(26).
The nurse navigator is the professional who is in constant contact with the patient, he or she is the one who makes the multidisciplinary contact with other health professionals, providing effective management of care in all phases of patient care(4) thus highlighting the leading role and the need for the nurse navigator to be trained and master the care pathway of the Navigation Program in which he or she works. COFEN Resolution No. 735 of January 17th, 2024(27) regulates the performance of the nurse navigator and makes mandatory the minimum three years of experience in the area in which he or she will work as a navigator as well as the completion of residency, specialization or postgraduate studies in the area in which he or she will work.
The Navigation Program adapts to the reality of each health service and in most cases, they are divided by care pathways or by specific diseases(28), which reinforces the need for the nurse navigator to receive training on how to perform patient navigation, as well as having the necessary knowledge of the pathway in which he or she will work as a navigator.
The use of the NNAS scale to assess patients' navigation needs, applied by the nurse navigator, made it possible to identify the main barriers faced by patients, which can be discussed with the multidisciplinary team in order to find ways to minimize them, enabling health education to be practiced with patients in an individualized way. As reported in the literature, navigation performed by the nurse occurs in a diversified, integrated and complex manner, demonstrating the capacity and potential of navigation performed by this professional(29).
The literature shows that navigated patients demonstrate less anxiety, better symptom control, improved care and quality of life(28), which is consistent with what was observed during the implementation of navigation, such as better preoperative planning, reduction of postoperative complications, and early detection of risks.
One limitation of this study is that it is a case report of a specific event that occurred in a large hospital where patient navigation had been previously implemented within other care pathways. This fact makes it difficult to implement the program in different institutional settings, especially those where patient navigation does not exist and where there is no appropriate space or experienced team for this type of care. However, the study is believed to be innovative and has the potential to encourage the implementation of new navigation programs, with nurses as key players in this promising area of practice.
CONCLUSION
The reported experience described the trajectory for the implementation of a Navigation Program for patients undergoing complex spinal surgery. The process lasted around six months, with the nurse navigator as the protagonist of the activities carried out, counting on the support of the multidisciplinary team. The results indicate benefits related to better pain control and a decrease in postoperative complications.
It was evident that the prior existence of an institutional navigation culture for other lines of care favored the fluidity of the implementation process of the Navigation Program, although the consolidation of the Program required technical commitment and continuous dedication from those involved. It is concluded that the success of the model lies in its person-centered nature, respecting the individuality of the patient in a highly complex scenario.
This report demonstrates the applicability of patient navigation as a tool for improving care and ratifies the nurse as a key player in the management of these programs. To this end, it reinforces the need for the professional to combine solid clinical and managerial skills, ensuring the effectiveness and sustainability of navigation in the health system.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
REFERENCES
1. Freeman HP. The origin, evolution, and principles of patient navigation. Cancer Epidemiol Biomarkers Prev. 2012;21(10):1614-7. https://doi.org/10.1158/1055-9965.EPI-12-0982. PMID: 23045534.
2. Kelly KJ, Doucet S, Luke A. Exploring the roles, functions, and background of patient navigators and case managers: A scoping review. Int J Nurs Stud. 2019;98:27-47. https://doi.org/10.1016/j.ijnurstu.2019.05.016. PMID: 31271977.
3. Johnson F. The Process of Oncology Nurse Practitioner Patient Navigation: A Pilot Study. Clin J Oncol Nurs. 2016;20(2):207-10. https://doi.org/10.1188/16.CJON.207-210. PMID: 26991716.
4. Pautasso FF, Lobo TC, Flores CD, Caregnato RCA. Nurse Navigator: development of a program for Brazil. Rev Lat Am Enfermagem. 2020;28:e3275. https://doi.org/10.1590/1518-8345.3258.3275. PMID: 32491120.
5. Brasil. Lei nº 14.450, de 21 de setembro de 2022. Cria o Programa Nacional de Navegação de Pacientes para Pessoas com Neoplasia Maligna de Mama [Internet]. Brasília: Presidência da República; 2022 [cited 2025 Oct 26]. Available from: https://www2.camara.leg.br/legin/fed/lei/2022/lei-14450-21-setembro-2022-793228-publicacaooriginal-166091-pl.html.
6. Brasil. Lei nº 14.758, de 19 de dezembro de 2023. Institui a Política Nacional de Prevenção e Controle do Câncer no âmbito do Sistema Único de Saúde (SUS) e o Programa Nacional de Navegação da Pessoa com Diagnóstico de Câncer; e altera a Lei nº 8.080, de 19 de setembro de 1990 (Lei Orgânica da Saúde) [Internet]. Brasília: Presidência da República; 2023 [cited 2025 Oct 26]. Available from: https://www.planalto.gov.br/ccivil_03/_ato2023-2026/2023/lei/l14758.htm.
7. Ministério da Saúde (BR). Portaria GM/MS Nº 6.592, de 4 de fevereiro de 2025. Altera a Portaria de Consolidação nº 5, de 28 de setembro de 2017, para instituir o Programa de navegação da pessoa com diagnóstico de câncer, no âmbito do Sistema Único de Saúde – SUS [Internet]. Brasília: Ministério da Saúde; 2025 [cited 2025 Oct 25]. Available from: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2025/prt6592_07_02_2025.html.
8. Malta DC, Bernal RTI, Ribeiro EG, Ferreira E de MR, Pinto RZ, Pereira CA. Chronic back pain among Brazilian adults: data from the 2019 National Health Survey. Rev Bras Epidemiol. 2022;25:e220032. https://doi.org/10.1590/1980-549720220032.2. PMID: 36287518.
9. Evans L, O'Donohoe T, Morokoff A, Drummond K. The role of spinal surgery in the treatment of low back pain. Med J Aust. 2023;218(1):40-5. https://doi.org/10.5694/mja2.51788. PMID: 36502448.
10. Ministério da Saúde (BR). Protocolo Clínico e Diretrizes Terapêuticas da Dor Crônica [Internet]. Brasília: Ministério da Saúde; 2024 [cited 2025 Oct 23]. Available from: https://www.gov.br/conitec/pt-br/midias/protocolos/dorcronica-1.pdf.
11. Silva DR, Werneck AO, Malta DC, Romero D, Souza-Júnior PRB, Azevedo LO, et al. Changes in movement behaviors and back pain during the first wave of the COVID-19 pandemic in Brazil. Braz J Phys Ther. 2021;25(6):819-25. https://doi.org/10.1016/j.bjpt.2021.07.006. PMID: 34548211.
12. Nunes PR, Maciel JV de S, Silva ACG, Barros PMB, Souza VC, Souza RM, et al. Hérnia discal lombar: revisão das abordagens cirúrgicas minimamente invasivas. Res Soc Dev. 2025;14(4):e3314448594. https://doi.org/10.33448/rsd-v14i4.48594.
13. Zanirato A, Damilano M, Formica M, Piazzolla A, Lovi A, Villafañe JH, et al. Complications in adult spine deformity surgery: a systematic review of the recent literature with reporting of aggregated incidences. Eur Spine J. 2018;27(9):2272-84. https://doi.org/10.1007/s00586-018-5535-y. PMID: 29497853.
14. Almeida CM, Harrop TA, Santos KMC, Costa WA, Sousa JS, Lopes ARP, et al Análise epidemiológica das artrodeses de coluna realizadas no Sistema Único de Saúde no Brasil de 2015 a 2024. Rev Ibero-Am Hum Ciênc Educ. 2024;10(11):4915-29. https://doi.org/10.51891/rease.v10i11.16848.
15. Galieri G, Orlando V, Altieri R, Barbarisi M, Olivi A, Sabatino G, et al. Current Trends and Future Directions in Lumbar Spine Surgery: a Review of Emerging Techniques and Evolving Management Paradigms. J Clin Med. 2025;14(10):3390. https://doi.org/10.3390/jcm14103390. PMID: 40429385.
16. Turcotte J, Menon N, Andersen K, Stone D, Patton C. The Impact of Nurse Navigator-Led Preoperative Education on Hospital Outcomes Following Posterolateral Lumbar Fusion Surgery. Orthop Nurs. 2021;40(5):281-9. https://doi.org/10.1097/NOR.0000000000000787. PMID: 34583373.
17. Silva AC, Alcantara T. Minimally invasive spine surgery: evaluation of clinical and functional outcomes and their correlation with the return to work. Rev Bras Med Trab. 2020;18(2):177-184. https://doi.org/10.47626/1679-4435-2020-518. PMID: 33324459.
18. Mussi RF de F, Flores FF, Almeida CB de. Pressupostos para a elaboração de relato de experiência como conhecimento científico. RPE. 2021;17(48):60-77. https://doi.org/10.22481/praxisedu.v17i48.9010.
19. Conselho Nacional de Saúde (BR). Resolução nº 510, de 7 de abril de 2016. Dispõe sobre as normas aplicáveis a pesquisas em Ciências Humanas e Sociais [Internet]. Brasília: CNS; 2016 [cited 2026 Feb 08]. Available from: https://www.gov.br/conselho-nacional-de-saude/pt-br/atos-normativos/resolucoes/2016/resolucao-no-510.pdf/view.
20. Pautasso FF, Trevilato DD, Caregnato RCA, Floriani MA, Pertile N de M, Pizzol Junior AD, et al. The path to implementing a patient navigation program in oncology: an experience report. Online Braz J Nurs. 2024;22(suppl 2):e20246691. https://doi.org/10.17665/1676-4285.20246.
21. Abreu AM, Oliveira SRC, Rocha BP, Nunes AS da S, Bastos VA, Pires TB, et al. Implementação do tumor board de enfermagem em onco-hematologia para aprimorar o cuidado centrado no paciente. Revft. 2025;29(147):4915-29. https://doi.org/10.69849/revistaft/pa10202506101904.
22. Maheshwari P, Bobb A, Stuart A, Dalessio S, Bernasko N, Tinsley A, et al. Impact of a nurse navigator on a dedicated inflammatory bowel disease-focused gastroenterology clinic. Ann Gastroenterol. 2021;34(5):675-9. https://doi.org/10.20524/aog.2021.0627. PMID: 34475738.
23. Siqueira SW de A, Fialho IR, Jaime M, Pautasso FF, Caregnato RCA. Atuação do enfermeiro navegador em diferentes áreas da saúde: revisão integrativa. Braz. J. Hea. Rev. 2022;5(5):20755-20770. https://doi.org/10.34119/bjhrv5n5-237.
24. International Society of Nurses in Cancer Care. Guide on How to Implement a Nurse Navigation Programme for Cancer Patients [Internet]. [place unknown]: ISNCC; 2021 [cited 2025 Oct 26]. Available from: https://citycancerchallenge.org/uploads/2023/02/How-to-Implement-a-Nurse-Navigation-Programme-for-Cancer-Patients-FINAL.pdf.
25. Siqueria SW de A da, Mattiello DP, Pautasso FF, Caregnato RCA. Private health plan operator: breast care navigation program and care line. Texto Contexto Enferm. 2023;32:e20230159. https://doi.org/10.1590/1980-265X-TCE-2023-0159en.
26. Uzunkaya Öztoprak P, Koç G. A Current Approach to Early Diagnosis and Treatment of Breast, Colorectal and Cervical Cancers in Women: “Nurse Navigation Program” and “Nurse Navigator”. J Educ Res Nurs. 2023;20(3):284-7. https://doi.org/10.14744/jern.2021.21186.
27. Conselho Federal de Enfermagem (BR). Resolução COFEN nº 735, de 17 de janeiro de 2024. Normatiza a atuação do Enfermeiro navegador e do Enfermeiro clínico especialista [Internet]. Brasília: COFEN; 2024 [cited 2026 Jan 06]. Available from: https://www.cofen.gov.br/resolucao-cofen-no-735-de-17-de-janeiro-de-2024/.
28. Pires JM, Rodrigues AB, Alencar MMS da C, Castro RCMB. Oncologic patient navigation by nurses: a scoping review. Rev Rene. 2024;25:e94027. http://doi.org/10.15253/2175-6783.20242594027.
29. Roque AC, Gonçalves IR, Popim RC. Experience of care nurses: approaches to the principles of navigation of cancer patients. Texto Contexto Enferm. 2023;32:e20230020. https://doi.org/10.1590/1980-265X-TCE-2023-0020en.
Submission: 07-Dec-2025
Editors:
Rosimere Ferreira Santana (ORCID: 0000-0002-4593-3715)
Geilsa Soraia Cavalcanti Valente (ORCID: 0000-0003-4488-4912)
Corresponding author: Giovana Loreto Nunes (giovanaloreton@gmail.com)
Publisher:
Escola de Enfermagem Aurora de Afonso Costa – UFF
Rua Dr. Celestino, 74 – Centro, CEP: 24020-091 – Niterói, RJ, Brazil
Journal email: objn.cme@id.uff.br
