
ORIGINAL ARTICLE
IMPLICATIONS OF THE COMPUTERIZATION OF RISK PREDICTION SCALES ON NURSING PROCESS RECORDS*
Betina Franco1, Maia Silvia da Silva Fredriksson2, Thiane Mergen3, Náthalli Cristina Paim Alves4, Ninon Girardon da Rosa5, Amália de Fátima Lucena6
1 Hospital de Clínicas de Porto Alegre, Nursing Process Commission. Porto Alegre, RS, Brazil. ORCID: 0000-0003-0503-5045. E-mail: bfranco@hcpa.edu.br
2 Hospital de Clínicas de Porto Alegre. Porto Alegre, RS, Brazil. ORCID: 0009-0000-2922-2852. E-mail: mfredriksson@hcpa.edu.br
3 Hospital de Clínicas de Porto Alegre, Nursing Process Commission. Porto Alegre, RS, Brazil. ORCID: 0000-0001-5603-905X. E-mail: tmergen@hcpa.edu.br
4 Federal University of Rio Grande do Sul, Nursing School. Porto Alegre, RS, Brazil. ORCID: 0009-0004-2786-8544. E-mail: nathalves9720@gmail.com
5 Federal University of Rio Grande do Sul, Graduate Program in Nursing. Porto Alegre, RS, Brazil. ORCID: 0000-0001-5701-0494. E-mail: ngrosa@hcpa.edu.br
6 Federal University of Rio Grande do Sul, Nursing School. Porto Alegre, RS, Brazil. ORCID: 0000-0002-9068-7189. E-mail: afatimalucena@gmail.com
ABSTRACT
Objective: To evaluate the implications of the computerization of risk prediction scales for pressure injury and falls in nursing process records, considering the stages of patient assessment, diagnosis, and progress notes. Method: This quantitative, observational, and retrospective study analyzed the computerization of risk prediction scales in a university hospital in the southern region of Brazil. Data were obtained from the electronic patient record. The sample consisted of 764 medical records of adult patients hospitalized in clinical and surgical units, including 382 records from the period prior to and 382 from the period after the computerization of the scales. Data analysis was performed using descriptive statistics with IBM SPSS Statistics for Windows software. Results: A significant improvement was observed in the recording of scores from the pressure injury and falls risk prediction scales in the assessment, diagnosis, and progress stages of the nursing process in the period after computerization. The nursing diagnoses identified in the records were related to the final scores of the predictive scales. Conclusion: The computerization of risk prediction scales was associated with an increase in records across the stages of the nursing process and may contribute to the safety and quality of care provided to patients.
Descriptors: Nursing Informatics; Nursing Records; Nursing Process; Risk Measurement.
|
How to cite: Franco B, Fredriksson MSS, Mergen T, Alves NCP, Rosa NG, Lucena AF. Implications of the computerization of risk prediction scales on nursing process records. Online Braz J Nurs. 2026;25(1):e20266861. https://doi.org/10.17665/1676-4285.20266861 |
What is already known:
Pressure injury and fall risk prediction scales support the nursing process, but when used on paper forms, they remain disconnected from the steps documented in the patient’s electronic medical record.
Real-time electronic recording increases the visibility of clinical data for the multidisciplinary team, facilitating decision-making and reducing adverse events.
Clinical decision support systems integrated into the electronic medical record have the potential to strengthen diagnostic reasoning and improve the planning of nursing care.
What this article adds:
The computerization of the Braden and SAK scales in the AGHUse® system significantly increased the recording of predictive scores during the assessment and progress stages of the Nursing Process.
Following computerization, greater alignment was observed between risk scores and established nursing diagnoses, with a significant increase in “Risk of pressure injury” and “Risk of falls.”
The integration of the scales into the electronic medical record contributed to patient safety and quality of care by promoting diagnostic accuracy and individualized planning of preventive measures.
INTRODUCTION
Risk prediction scales are tools developed to provide health professionals with an objective assessment of the probability that a given outcome will affect a patient. Their use allows systematic and accurate evaluations, supporting decision-making and care planning by the multidisciplinary team(1). In the context of nursing, risk prediction scales support the nursing process (NP), contributing both to the initial assessment and to monitoring the patient’s clinical progression. In addition, they favor clinical reasoning aimed at establishing diagnoses, planning care, and making decisions, with the goal of achieving the best possible outcomes and promoting safer and more qualified care(2-3). These tools can also improve the documentation of nursing records in the electronic patient record (EPR), whether in physical or electronic format, by demonstrating the care provided according to the identified problems and the risk factors presented(2).
In the institution where this study was conducted, the NP is developed based on standardized language systems integrated into the EPR, in accordance with theoretical frameworks(4-6) and Brazilian professional legislation(2,7-9). However, until 2019, risk prediction scales were applied using printed forms, separately from the stages of the NP and, consequently, from the EPR. This reality, also observed in other institutions, may be associated with weaknesses in health records and possible harm to the safety and quality of care. Among the limitations of manual documentation is the time required for information to become available to the care team. In contrast, recording data in the EPR, when performed in real time, facilitates the rapid availability of information to health professionals, contributing to decision-making and reducing the likelihood of errors, incidents, and adverse events with potential negative impact on the patient(9).
Thus, in 2019 the institution implemented the computerization of the risk prediction scales used by nursing in the AGHUse® system, an open-source EPR software with an integrated management system capable of generating results that support the transformation of healthcare management(10). This initiative enabled the integration of risk prediction scores into the stages of the NP, especially with regard to assessment, nursing diagnoses, and nursing progress notes. Such integration began to stimulate critical thinking, improve diagnostic accuracy, expand the implementation of preventive measures in response to adverse events, and improve the monitoring of these events.
Among the computerized scales implemented at the institution are the Braden Scale, used to assess the risk of pressure injury (PI) in adult patients(11), and the Severo-Almeida-Kuchenbecker (SAK) Scale, intended to assess the risk of falls in hospitalized adult patients(12). SAK replaced the Morse Fall Scale(13), which had previously been used since 2000 in a printed form. The computerization represented a relevant advancement in the work process by improving care practices, strengthening communication among the multidisciplinary team, and ensuring the visibility of data recorded in real time in the EPR in a clear and standardized manner.
Despite the observed advances, the need was identified to evaluate the use of this new functionality developed in AGHUse®, which makes it possible to relate risk prediction scales to the computerized NP. In this context, the following guiding question was formulated: did the computerization of risk prediction scales applied by nursing improve the recording of NP stages?
The present study aimed to evaluate the implications of the computerization of risk prediction scales for PI and falls on NP records, considering the stages of patient assessment, nursing diagnosis, and nursing progress notes.
METHOD
This was a quantitative, observational, and retrospective study that analyzed the computerization of risk prediction scales for PI and falls. The conduct of the study was guided by the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD)(14-15).
The study was conducted in 2023 at a federal public university hospital in the southern region of Brazil. Retrospective data were used from the second half of 2018, the period immediately preceding the beginning of the computerization process of the risk prediction scales for PI (Braden)(11) and falls (Morse Fall Scale)(13), and from the second half of 2019, the period immediately following the completion of the computerization of the Braden (predictive for PI)(11) and SAK (predictive for falls)(12) scales.
The study population consisted of data from EPRs of patients hospitalized in the institution’s clinical and surgical units. The sample size was calculated to detect differences between the proportions of patients with and without risk of PI and with and without risk of falls, using the PSS Health online tool. The final sample consisted of 764 EPRs, including 382 from the period prior to and 382 from the period after the computerization of the scales, encompassing the assessment of PI and falls risk using their respective predictive scales.
EPRs of adult patients aged 18 years or older, of both sexes, hospitalized in clinical and surgical units, who were assessed using the Braden and Morse Fall Scale in the second half of 2018 and the Braden and SAK scales in the second half of 2019 were included. An additional inclusion criterion was that the first assessment using the scales had been performed within the first 24 hours of hospital admission. EPRs of patients without a nursing assessment record in the EPR at the time of hospital admission were excluded.
Data collection logistics were organized into four stages. The first stage consisted of selecting EPRs of hospitalized patients obtained through queries, a process of extracting information from the AGHUse® database requested from the Informatized Medical Records Archive Service (SAMIS, in Portuguese). These queries identified 7,288 EPRs of patients hospitalized between 07/01/2018 and 12/31/2018 and between 07/01/2019 and 12/31/2019, regardless of the hospitalization unit, a number higher than the calculated sample size of 764 EPRs.
Randomization was performed to select the sample in each period using Microsoft Excel through the “RANDBETWEEN” function in order to compose 382 EPRs for each group, before and after computerization (Figure 1).
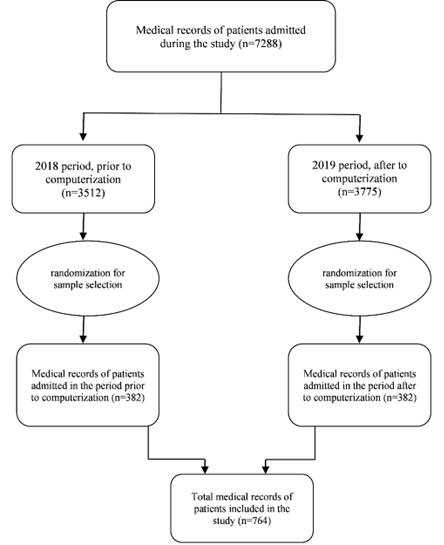
Figure 1 - Flowchart of selection and inclusion of patient records. Porto Alegre, RS, Brazil, 2023
Source: prepared by the authors, 2023.
In the second stage, after selecting the eligible EPRs, a new query was requested from SAMIS to obtain data related to sample characterization. Sociodemographic and clinical variables of the patients were collected and subsequently organized into a secondary database specific to the study.
In the third stage, a data collection instrument was applied to identify the presence of records of risk prediction scores from the Braden, Morse Fall Scale, and SAK scales in the stages of the NP. The instrument was developed by the researchers using the Google Forms platform and structured into two sections: the first focused on the evaluation of EPRs regarding PI risk prediction (Braden), and the second referred to falls risk prediction (Morse Fall Scale or SAK). Its construction was based on the stages of the computerized NP in the AGHUse® system (nursing assessment and nursing progress notes) and on nursing diagnoses (NDs) related to the investigated phenomena — PI and falls — according to the diagnostic taxonomy of NANDA International (NANDA-I)(6). The instrument underwent a pilot test with a previously trained team to ensure the quality and agreement of the collected data.
The fourth stage consisted of identifying the NDs recorded in the 764 EPRs included in the sample through a new query requested from SAMIS. NDs related to psychosocial and spiritual needs were excluded because they were not the focus of the study, and only those associated with psychobiological needs were retained(4). The analysis was performed by the principal investigator under the supervision of the advisor, based on the NANDA-I taxonomy, considering definitions, risk factors, related factors, and defining characteristics relevant to PI and falls events(6).
Data were stored in an institutional drive with restricted access to the researchers. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, N.Y., USA). Continuous variables with asymmetric distribution were expressed as median and interquartile range according to the assessment of normality using the Kolmogorov-Smirnov test. Categorical variables were presented as absolute numbers and percentages. To analyze associations between the periods before and after the computerization of the risk prediction scales, the chi-square test and/or Fisher’s exact test were used for categorical variables. The significance level adopted was 5% (p < 0.05).
The study was conducted in accordance with national ethical guidelines and was approved by the institution’s research ethics committee under CAAE no. 66618123.1.0000.5327 and opinion no. 5.992.572. The researchers declared that they were aware of and complied with the requirements of the Brazilian General Data Protection Law(16). Patient consent was waived because this study used exclusively retrospective data from the EPR, and contacting all potential participants was not feasible due to incomplete or outdated records, occurrence of deaths, and possible risks or discomfort associated with contacting individuals to obtain consent.
RESULTS
Among the 764 EPRs of hospitalized patients analyzed, 402 (52.6%) corresponded to women. The median age was 61 [49-71] years, and most hospitalizations occurred in surgical units (n = 647; 84.7%). The median length of stay was 5 [3-11] days.
Regarding educational level, 271 (35.5%) patients had incomplete elementary education, and 301 (39.4%) were from the city of Porto Alegre, Rio Grande do Sul. According to the International Classification of Diseases and Related Health Problems, the main reasons for hospitalization were neoplasms (n = 221; 27.6%), diseases of the circulatory system (n = 119; 15.6%), and diseases of the genitourinary system (n = 110; 14.4%) (Table 1).
Table 1 - Sociodemographic and clinical characteristics of patients described in the electronic patient record, before and after the computerization of risk prediction scales in the AGHUse® system. Porto Alegre, RS, Brazil, 2023
|
Variable |
Before computerization (n = 382) |
After computerization (n = 382) |
Total (n = 764) |
|
Age, years* |
60 [16-92] |
63 [18-99] |
61 [49-71] |
|
Female sex† |
197 (51.6) |
205 (53.7) |
402 (52.6) |
|
Area of hospitalization |
|
|
|
|
Surgical units |
322 (84.3) |
325 (85.1) |
647 (84.7) |
|
Clinical units |
60 (15.7) |
57 (14.9) |
117 (15.3) |
|
Total length of stay, days* |
5 [1-140] |
4 [1-56] |
5 [3-11] |
|
Length of stay in surgical units (days)* |
5 [3-10] |
4 [2-9] |
5 [3-10] |
|
Length of stay in clinical units (days)* |
5 [2-12] |
4 [2-8] |
5 [2-10] |
|
Place of origin† |
|
|
|
|
City of Porto Alegre |
151 (39.5) |
150 (39.3) |
301 (39.4) |
|
Countryside of the state of Rio Grande do Sul |
133 (34.8) |
141 (36.9) |
274 (35.9) |
|
Metropolitan region of Porto Alegre |
98 (25.7) |
91 (23.8) |
189 (24.7) |
|
Education† |
|
|
|
|
Incomplete elementary education |
151 (39.5) |
120 (31.4) |
271 (35.5) |
|
Reason for hospitalization/ICD† |
|
|
|
|
Neoplasms (tumors) |
100 (26,2) |
111 (29.1) |
221 (27.6) |
|
Diseases of the circulatory system |
57 (14.9) |
62 (16.2) |
119 (15.6) |
|
Diseases of the genitourinary system |
53 (13.9) |
57 (14.9) |
110 (14.4) |
|
Diseases of the digestive system |
25 (6.5) |
35 (9.2) |
60 (7.9) |
|
Diseases of the musculoskeletal system/connective tissue |
30 (7.9) |
24 (6.3) |
54 (7.1) |
|
Endocrine, nutritional/metabolic diseases |
24 (6.3) |
12 (3.1) |
36 (4.7) |
|
Other |
93 (24.3) |
81 (21.1) |
164 (21.4) |
Source: prepared by the authors, 2023.
*Asymmetric variables presented as median and interquartile range.
†Categorical variables expressed as n (%).
ICD: International Classification of Diseases and Related Health Problems.
With respect to records of the PI risk score, the comparison between the periods before and after computerization showed a significant increase in the frequency of recording the Braden score in the nursing assessment (p < 0.001). This increase was also observed in nursing progress notes performed within the first 24 hours of hospital admission (n = 368; 96.8%), with a statistically significant difference (p < 0.001) (Table 2).
Similarly, when analyzing the presence of the falls risk score (Morse Fall Scale; SAK) in nursing assessment records, a significant increase in frequency was observed after computerization (p < 0.001). There was also a significant increase in the recording of these scores in nursing progress notes performed within the first 24 hours of hospitalization (p < 0.001) (Table 2).
Table 2 - Frequency of records in the patient record of the risk score for pressure injury and falls in nursing assessment and nursing progress notes, before and after the computerization of the scales in the AGHUse® system. Porto Alegre, RS, Brazil, 2023
|
Presence of risk score record in NP stages |
Before computerization (n = 382) |
After computerization (n = 382) |
p-value |
|
Pressure injury risk score |
|||
|
Nursing Assessment |
|||
|
Braden score |
365 (95.5) |
378 (99.0) |
< 0.001* |
|
Progress notes within the first 24h |
|||
|
Braden score |
315 (83.3) |
368 (96.8) |
< 0.001* |
|
Falls risk score |
|||
|
Nursing Assessment |
|||
|
Risk prediction score |
366 (95.8) |
378 (99.0) |
< 0.001* |
|
Progress notes within the first 24h |
|||
|
Risk prediction score |
335 (87.7) |
376 (98.4) |
< 0.001* |
Source: prepared by the authors, 2023.
Categorical variables expressed as n (%). Statistical significance considered for p ≤ 0.05.
*Pearson’s chi-square test.
Regarding the NDs established for the 764 patients evaluated, 13 distinct NDs were identified, classified as actual or risk diagnoses. Among patients at risk for PI according to the Braden scale, the most frequent NDs were “Risk for perioperative positioning injury” (n = 396; 35.3%) and “Impaired tissue integrity” (n = 139; 18.7%). When comparing the periods, a significant increase was observed in the frequency of the ND “Risk for pressure injury” after computerization (p = 0.001) (Table 3).
Table 3 - Nursing diagnoses established for patients evaluated regarding their PI risk score using the Braden scale, identified in records before and after the computerization of the scales in the AGHUse® system. Porto Alegre, RS, Brazil, 2023
|
Nursing diagnosis** |
Before computerization*** (n = 354) |
After computerization*** (n = 388) |
Total (n = 742) |
p-value |
|
Risk for perioperative positioning injury |
190 (53.7) |
206 (53.1) |
396 (53.4) |
0.87* |
|
Impaired tissue integrity |
67 (18.9) |
72 (18.6) |
139 (18.7) |
0.89* |
|
Risk for pressure injury |
14 (4.0) |
51 (13.1) |
65 (8.8) |
0.00* |
|
Impaired physical mobility |
20 (5.6) |
16 (4.1) |
36 (4.9) |
0.33* |
|
Decreased self-care ability syndrome |
23 (6.5) |
10 (2.6) |
33 (4.4) |
0.01* |
|
Acute pain |
14 (4.0) |
12 (3.1) |
26 (3.5) |
0.52* |
|
Decreased grooming abilities |
10 (2.8) |
6 (1.5) |
16 (2.2) |
0.23* |
|
Impaired skin integrity |
6 (1.7) |
5 (1.3) |
11 (1.5) |
0.64* |
|
Risk for impaired skin integrity |
7 (2.0) |
4 (1.0) |
11 (1.5) |
0.28* |
|
Risk for infection |
3 (0.8) |
5 (1.3) |
8 (1.1) |
0.56* |
|
Chronic pain |
— |
1 (0.3) |
1 (0.1) |
0.33* |
Source: prepared by the authors, 2023.
Categorical variables expressed as n (%). Statistical significance considered for p ≤ 0.05.
*Pearson’s chi-square test.
**Patients presented one or more nursing diagnoses.
***Number of times the nursing diagnosis was established.
In the EPRs of patients at risk of falls, five NDs related to the event were identified, the most frequent being “Risk for falls” (n = 297; 73.3%). When comparing the periods before and after computerization, a significant increase in the frequency of this ND was observed (p = 0.05). Conversely, the ND “Risk for bleeding” showed a significant reduction after the computerization of the risk prediction scales (p = 0.04) (Table 4).
Table 4 - Nursing diagnoses established for patients evaluated regarding the falls risk score using the Morse and SAK scales, identified in records before and after the computerization of the scales in the AGHUse® system. Porto Alegre, RS, Brazil, 2023
|
Nursing diagnosis** |
Before computerization*** (n = 204) |
After computerization*** (n = 201) |
Total (n = 405) |
p-value |
|
Risk for falls |
141 (69.1) |
156 (77.6) |
297 (73.3) |
0.05* |
|
Impaired physical mobility |
24 (11.8) |
20 (10.0) |
44 (10.9) |
0.55* |
|
Decreased self-care ability syndrome |
22 (10.8) |
19 (9.5) |
41 (10.1) |
0.65* |
|
Risk for bleeding |
6 (3.0) |
21 (5.2) |
0.04* |
|
|
Decreased grooming abilities |
2 (1.0) |
— |
2 (0.5) |
0.15* |
Source: prepared by the authors, 2023.
Categorical variables expressed as n (%). Statistical significance considered for p ≤ 0.05.
*Pearson’s chi-square test.
**Patients presented one or more nursing diagnoses.
***Number of times the nursing diagnosis was established.
DISCUSSION
The computerization of risk prediction scales for PI and falls demonstrated a positive and statistically significant impact on the records of NP stages in the studied institution. This finding reinforces the relevance of the technological advancement implemented and the innovative nature of the study, particularly due to the integration of the scales into the EPR.
Improvement was observed in the records of PI and falls risk scores in the nursing assessment stage when compared with the period before computerization. In this stage, the nurse establishes rapport with the patient and performs a physical examination to identify clinical evidence and risk factors that support the identification of NDs and decision-making regarding the necessary interventions(6,17). The incorporation of predictive scores into this stage strengthens patient safety by increasing the objectivity of clinical assessment. Computerization enabled the automation of these records, promoting more comprehensive assessments and supporting the establishment of more accurate NDs, with a direct impact on care planning(18-20).
In the nursing progress stage, a significant improvement in the presence of scores was also identified after computerization for both patients at risk of PI and those at risk of falls. This result is partly due to the automation of records, since the scores applied during assessment began to migrate automatically to the progress note field, providing greater visibility of the identified risks(21). However, the nurse remains responsible for the daily validation of these scores, ensuring safe and updated documentation in the EPR.
The automation of scores increased the visibility of information related to PI and falls risks for the entire multidisciplinary team, supporting the adoption of safer care practices. Integrated record systems and clinical decision support tools have been associated with improved care efficiency, increased patient safety, and greater satisfaction among healthcare professionals. These systems play an important role in reducing adverse events by signaling critical points that require clinical attention(22).
Among the NDs established for patients evaluated for PI risk, the most frequent was “Risk for perioperative positioning injury”(6), regardless of the analyzed period. This finding is directly related to the profile of the sample, which consisted predominantly of surgical patients (84.7%). The literature highlights the importance of care related to PI risk associated with surgical positioning(23-24). The high frequency of this ND may reflect the recognition of intrinsic and extrinsic factors as well as the expertise of nurses in associating predictive factors with the establishment of more accurate NDs(25-26).
The ND “Impaired tissue integrity”(6) also showed high frequency. Considering the predominance of surgical patients, it is plausible that this ND is related to mechanical trauma resulting from surgical or invasive procedures rather than necessarily to the occurrence of PI.
The ND “Adult pressure injury”(6) showed a significant increase after computerization. According to the NANDA-I taxonomy(6), this is the most appropriate ND for patients classified as high risk according to the Braden score. The functionality implemented in AGHUse® began to provide clinical decision support by suggesting the opening of this ND when a higher risk was identified. This mechanism likely contributed to the increase in its frequency and to greater diagnostic accuracy after computerization(27-29).
Regarding the identification of NDs related to falls risk, the most frequent was “Risk for falls”(6). This finding is consistent with the literature, as demonstrated in a study conducted with adult patients hospitalized in clinical and surgical units, which also identified this ND among the most prevalent(30). Another study conducted with 80 patients hospitalized in surgical units found that 86.25% presented the ND “Risk for falls”(31). It was also observed that, after the computerization of the scales, this ND remained the most frequent, indicating that the functionality developed in the AGHUse® system to increase diagnostic accuracy, similar to that implemented for patients at risk of PI, began to provide clinical decision support. Thus, the system began to signal to the nurse the need to establish the ND “Risk for falls” according to the identified risk stratification.
The development and use of clinical decision support systems focused on nursing represent tools that assist the care work process. Although they do not replace the professional’s clinical reasoning, these systems contribute to increasing decision-making accuracy(27-28). In addition, clinical decision support encourages nursing staff adherence to new functionalities by providing greater confidence for the professionals involved. It also contributes to building an environment conducive to digital transformation by promoting integration between healthcare professionals and information technology professionals, who share multidisciplinary knowledge and produce new evidence to improve care quality(32).
Another ND frequently identified among patients at risk of falls was “Risk for bleeding”(6). Although it was recorded more frequently before the computerization of the prediction scales and does not present a direct relationship with predictive falls scores, it is important to consider that, in the institution where the study was conducted, patients with critical results in prothrombin time, activated partial thromboplastin time, and/or platelet count must have this ND established. In such cases, the prescription of nursing care is also recommended, with special attention to falls prevention measures, since this type of adverse event may result in severe complications in patients with increased bleeding risk(33).
Overall, the study results indicate that the computerization of risk prediction scales positively affected the records of NP stages, particularly due to the systematic presence of risk scores. This integration enabled more detailed monitoring of health risks, supported clinical decision-making, and generated automated alerts that facilitate the establishment of more accurate nursing actions. These actions have the potential to prevent or mitigate adverse events, contributing to reduced hospital length of stay and associated costs(34).
Despite the observed advances, expanding the use of nursing informatics still faces important challenges, mainly related to limited financial resources and the need for professional training. Nevertheless, the computerization of risk prediction scales may represent a strategic investment for transforming care by contributing to the mitigation of adverse events and to the reduction of care-related costs resulting from these events(35).
Among the study limitations, it is important to highlight that sample selection was performed through simple randomization without stratification by groups, such as clinical and surgical patients. This resulted in a greater number of EPRs from patients hospitalized in surgical units, which present higher turnover in the studied institution. Another limitation refers to the replacement of the Morse Fall Scale with the SAK scale during the same period in which the computerization of the scales occurred. However, this situation is not considered to have introduced bias in the results, since the study did not compare the items of the scales but rather analyzed the impact of recording their scores on NP stages.
CONCLUSION
There was a significant increase in the frequency of recording predictive scores for PI and falls in the nursing assessment and nursing progress stages of the NP after the computerization of the risk prediction scales.
In the ND stage, greater alignment was observed between risk stratification and the establishment of NDs, which may have contributed to improvements in the care provided to patients. In addition, although not a specific focus of investigation in this study, advances related to agility, connectivity, and institutional sustainability were observed, particularly due to the reduction in the use of paper forms.
Thus, the computerization of risk prediction scales proved to be relevant for care practice by improving NP records, strengthening nurses’ clinical reasoning, and facilitating risk identification. This process contributes to more precise and individualized targeting of preventive actions and promotes greater safety in patient care.
*Article derived from the doctoral dissertation entitled “Evaluation of the impact of the informatization of risk prediction scales on the quality of nursing records: a before-and-after study,” presented to the Graduate Program in Nursing at the Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil, in 2024.
ACKNOWLEDGMENTS
To the Nursing Directorate and the Coordination of Information and Communication Technology Management (CGTIC) of the Hospital de Clínicas de Porto Alegre for their valuable support in the development and implementation of this project.
CONFLICT OF INTERESTS
The authors declare no conflict of interests.
FUNDING
This study was supported by the National Council for Scientific and Technological Development (CNPq) of Brazil (Research Productivity Grant–PQ). Grant No. 311604/2021-8.
REFERENCES
1. Anstey KJ, Zheng L, Peters R, Kootar S, Barbera M, Stephen R, et al. Dementia Risk Scores and Their Role in the Implementation of Risk Reduction Guidelines. Front Neurol. 2021;12:765454. https://doi.org/10.3389/fneur.2021.765454. PMID: 35058873.
2. Franco B, Moura DS de, Rosa NG da, Mergen T, Dora JM, Lucena A de F. Computerization of risk prediction scale: strategy for safety and quality of care. Rev Gaucha Enferm. 2023;44:e20220248. https://doi.org/10.1590/1983-1447.2023.20220248.en. PMID: 37585959.
3. Conselho Federal de Enfermagem (BR). Resolução COFEN nº 736, 23 de janeiro de 2024. Dispõe sobre a implementação do Processo de Enfermagem em todo contexto socioambiental onde ocorre o cuidado de enfermagem [Internet]. Rio de Janeiro: COFEN; 2024 [cited 2024 Mar 23]. Available from: https://www.cofen.gov.br/resolucao-cofen-no-736-de-17-de-janeiro-de-2024/.
4. Horta W de A. A metodologia do processo de enfermagem [Internet]. Rev Bras Enferm [Internet]. 1971 [cited 2024 Jun 19];24(6):81-95. Available from: https://pesquisa.bvsalud.org/portal/resource/pt/bde-4212.
5. Wagner CM, Butcher HK, Clarke MF. NIC – Classificação das Intervenções de Enfermagem. 8. ed. Rio de Janeiro: Guanabara Koogan; 2025.
6. Herdman TH, Kamitsuru S, Lopes CT. NANDA International Nursing Diagnoses: Definitions and Classification, 2024–2026. 13. ed. Porto Alegre: Artmed; 2024.
7. Barros ALBL de, Lucena A de F, Almeida M de A, Brandão MAG, Santana RF, Cunha ICKO, et al. The advancement of knowledge and the new Cofen resolution on the Nursing Process. Rev Gaucha Enferm. 2024;45:e20240083. https://doi.org/10.1590/1983-1447.2024.20240083.en. PMID: 38896697.
8. Conselho Federal de Enfermagem. Resolução COFEN nº 754, 16 de maio de 2024. Normatiza o uso do prontuário eletrônico e plataformas digitais no âmbito da Enfermagem: digitalização, utilização de sistemas informatizados para guarda e armazenamento nesta tecnologia [Internet]. Rio de Janeiro: COFEN; 2024 [cited 2025 Oct 12]. Available from: https://www.cofen.gov.br/resolucao-cofen-no-754-de-16-de-maio-de-2024/.
9. Shafiee M, Shanbehzadeh M, Nassari Z, Kazemi-Arpanahi H. Development and evaluation of an electronic nursing documentation system. BMC Nurs. 2022;21(1):15. https://doi.org/10.1186/s12912-021-00790-1. PMID: 35012513.
10. Comunidade AGHUse. Sobre o AGHUse [Internet]. Porto Alegre: Hospital de Clínicas de Porto Alegre; 2022 [cited 2024 Mar 23]. Available from: https://sites.google.com/hcpa.edu.br/aghuse/sobre-o-aghuse.
11. Paranhos WY, Santos VLC de G. Avaliação de risco para úlceras de pressão por meio da Escala de Braden, na língua portuguesa. Rev Esc Enferm USP [Internet]. 1999 [cited 2024 Mar 21];33(n. esp.):191-206. Available from: http://www2.ee.usp.br/reeusp/upload/pdf/799.pdf.
12. Severo IM, Kuchenbecker R, Vieira DFVB, Pinto LRC, Hervé M e W, Lucena AF, et al. A predictive model for fall risk in hospitalized adults: a case-control study. J Adv Nurs. 2019;75(3):563-72. https://doi.org/10.1111/jan.13882. PMID: 30334584.
13. Urbanetto J de S, Creutzberg M, Franz F, Ojeda BS, Gustavo A da S, Bittencourt HR, et al. Morse fall scale: translation and transcultural adaptation for the portuguese language. Rev Esc Enferm USP. 2013;47(3):569-75. https://doi.org/10.1590/s0080-623420130000300007.
14. Benchimol EI, Smeeth L, Guttmann A, Harron K, Moher D, Petersen I, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. https://doi.org/10.1371/journal.pmed.1001885. PMID: 26440803.
15. Zhao HJ, Ushcatz I, Walwyn C, Lowe MS, Kim KS, Benchimol EI, et al. Adherence to RECORD reporting guidelines among observational studies using routinely collected health data published in general medical journals: a meta-epidemiologic study. J Clin Epidemiol. 2025;185:111876. https://doi.org/10.1016/j.jclinepi.2025.111876. PMID: 40562253.
16. Brasil. Lei nº 13.709 de 14 de agosto de 2018. Lei Geral de Proteção de Dados Pessoais [Internet]. Brasília: Presidência da República; 2018 [cited 2025 Oct 12]. Available from: http://www.planalto.gov.br/ccivil_03/_ato2015-2018/2018/lei/l13709.htm.
17. Barros ALBL, Lucena A de F, Morais SCRV, Brandão MAG, Almeida M de A, Cubas MR, et al. Nursing Process in the Brazilian context: reflection on its concept and legislation. Rev Bras Enferm. 2022;75(6):e20210898. https://doi.org/10.1590/0034-7167-2021-0898. PMID: 35584516.
18. Adamy EK, Poltronieri P, Zanatta EA. Technologies for Nurses' Clinical Reasoning: Integrative Review. NTQR. 2022;13:e669. https://doi.org/10.36367/ntqr.13.2022.e669.
19. Luiz FS, Vasconcellos LJ, Barbosa ACS, Paiva A do CPC, Santos KB, Sanhudo NF, et al. Papel do pensamento crítico na tomada de decisão pelo enfermeiro: revisão integrativa. Acervo Saúde. 2020:e1763. https://doi.org/10.25248/reas.e1763.2020.
20. Negreiros FD da S, Moreira TR, Moreira TMM, Silva LMS, Freitas MC, Guedes MVC. The importance of logical thinking for clinical nursing care. Rev Gaucha Enferm. 2022;43:e20200473. https://doi.org/10.1590/1983-1447.2022.20200473.pt. PMID: 35920518.
21. Hernández-García V, Vázquez-Sánchez BG, Santiago-González N. Cumplimiento del registro clínico electrónico acorde al modelo del cuidado de enfermería. Rev Enferm Inst Mex Seguro Soc [Internet]. 2021 [cited 2024 Jun 19];29(3):166-73. Available from: https://revistaenfermeria.imss.gob.mx/index.php/revista_enfermeria/article/view/1201.
22. Santoro R da S, Marin H de F. Análise dos benefícios do sistema de apoio à decisão clínica em hospital para reduzir eventos adversos em casos de úlceras por pressão e quedas. J Health Inform [Internet]. 2020 [cited 2024 Jun 19];12(3). Available from: https://jhi.sbis.org.br/index.php/jhi-sbis/article/view/735.
23. Gürer Z, Akansel N, Kahraman N. Pressure ulcer risk in patients undergoing cardiovascular surgery and their occurrence within 24 hours of the operation. Rev Esc Enferm USP. 2025;59:e20250081. https://doi.org/10.1590/1980-220X-REEUSP-2025-0081en. PMID: 40762991.
24. Silva TF da, Tristão FS, Echevarria-Guanilo ME, Zillmer JGV, Oliveira CM de. Cuidados para prevenção de lesão por pressão realizada por enfermeiros em um hospital de ensino. RUE. 2023;18(2):e2023v18n2a8. https://doi.org/10.33517/rue2023v18n2a8.
25. Bjorklund-Lima L, Müller-Staub M, Rejane Rabelo-Silva E. Knowledge translation for nursing care for patients with Risk of perioperative positioning injury: A case report. Int J Nurs Knowl. 2023;34(4):247-253. https://doi.org/10.1111/2047-3095.12398. PMID: 36151784.
26. Rodrigues AL, Torres FBG, Santos EAP, Cubas MR. Process modeling: technological innovation to control the risk for perioperative positioning injury. Rev Bras Enferm. 2021;74(suppl 6):e20200145. https://doi.org/10.1590/0034-7167-2020-0145. PMID: 34495212.
27. Oliveira NB, Peres HHC. Quality of the documentation of the Nursing process in clinical decision support systems. Rev Lat Am Enfermagem. 2021;29:e3426. https://doi.org/10.1590/1518-8345.4510.3426. PMID: 34037121.
28. Ortiz DR, Maia F de OM, Ortiz DCF, Peres HHC, Sousa PAF. Computerized clinical decision support system utilization in nursing: a scoping review protocol. JBI Database System Rev Implement Rep. 2017;15(11):2638-2644. https://doi.org/10.11124/JBISRIR-2016-003184. PMID: 29135746.
29. Mebrahtu TF, Bloor K, Ledward A, Keenan A, Andre D, Randell R, et al. Effects of computerised clinical decision support systems (CDSS) on nursing and allied health professional performance and patient outcomes: a systematic review of experimental and observational studies. Health Soc Care Deliv Res. 2024;12(40):95-96. https://doi.org/10.1002/14651858.CD014699. PMID: 39425942.
30. Luzia M de F, Victor MA de G, Lucena A de F. Nursing Diagnosis Risk for falls: prevalence and clinical profile of hospitalized patients. Rev Lat Am Enfermagem. 2014;22(2):262-268. https://doi.org/10.1590/0104-1169.3250.2411. PMID: 26107834.
31. Vitor AF, Moura LA, Fernandes A, Botarelli FR, Araújo JNM, Vitorino ICC. Risk for falls in patients in the postoperative period. Cogitare Enferm [Internet]. 2015 [cited 2024 Jun 19];20(1):29-37. Available from: https://docs.bvsalud.org/biblioref/2016/07/594/38509-151063-1-pb.pdf.
32. Zhao Y, Hu J, Gu Y, Wan Y, Liu F, Ye C, et al. Development and Implementation of a Pediatric Nursing-Clinical Decision Support System for Hyperthermia: A Pre- and Post-test. Comput Inform Nurs. 2021;40(2):131-137. https://doi.org/10.1097/CIN.0000000000000812. PMID: 34347639.
33. Lucena A de F, Laurent M do CR, Reich R, Pinto LRC, Carniel EL, Scotti L, et al. Nursing diagnosis risk for bleeding as an indicator of quality of care for patient safety. Rev Gaucha Enferm. 2019;40(spe):e20180322. https://doi.org/10.1590/1983-1447.2019.20180322. PMID: 31038603.
34. Igarashi MKW, Rodrigues MS, Ricci GP. Contribuições do prontuário eletrônico para a assistência de enfermagem sob a ótica da auditoria da qualidade. Res Soc Dev. 2022;11(14):e89111436001. https://doi.org/10.33448/rsd-v11i14.36001.
35. Fuchs D, Waibel AK, Karthan M, Seifert N, Örtl M, Bethge S, et al. CARE REGIO - Digital Transformation and Technology in Nursing Care. Stud Health Technol Inform. 2022;289:286-9. https://doi.org/10.3233/SHTI210915.
Submission: 28-Nov-2025
Editors:
Rosimere Ferreira Santana (ORCID: 0000-0002-4593-3715)
Geilsa Soraia Cavalcanti Valente (ORCID: 0000-0003-4488-4912)
Patricia dos Santos Claro Fuly (ORCID: 0000-0002-0644-6447)
Corresponding author: Amália de Fátima Lucena (afatimalucena@gmail.com)
Publisher:
Escola de Enfermagem Aurora de Afonso Costa – UFF
Rua Dr. Celestino, 74 – Centro, CEP: 24020-091 – Niterói, RJ, Brazil
Journal email: objn.cme@id.uff.br
