
REVIEW ARTICLE
CONFIGURATIONS OF COMPASSIONATE COMMUNITIES FOR THE PROVISION OF PALLIATIVE CARE: A SCOPING REVIEW
Matheus Rodrigues Martins1, Alexandre Ernesto Silva2, Ana Luiza Antunes de Lima3, Maria Luiza Carvalho dos Santos Recla de Jesus4, Enzo Pace Raizaro5, Kênia Lara Silva6
1 Federal University of Minas Gerais, UFMG School of Nursing. Belo Horizonte, Minas Gerais, Brazil. ORCID: 0000-0002-3739-6921. Email: matheusrodrigues355@gmail.com
2 Federal University of Minas Gerais, UFMG School of Nursing. Belo Horizonte, Minas Gerais, Brazil. ORCID: 0000-0001-9988-144X. Email: alexandresilva@ufsj.edu.br
3 Federal University of São João del-Rei, Campos Central-West Dona Lindu. Divinópolis, Minas Gerais, Brazil. ORCID: 0009-0004-5554-0466. Email: aanaluizantunes@gmail.com
4 Federal University of São João del-Rei, Campos Central-West Dona Lindu. Divinópolis, Minas Gerais, Brazil. ORCID: 0009-0004-5499-0203. Email: marialuizarecla@gmail.com
5 Federal University of São João del-Rei, Campos Central-West Dona Lindu. Divinópolis, Minas Gerais, Brazil. ORCID: 0000-0001-8229-9621. Email: enzoraizaro@hotmail.com
6 Federal University of Minas Gerais, UFMG School of Nursing. Belo Horizonte, Minas Gerais, Brazil. ORCID: 0000-0003-3924-2122. Email: kenialara17@gmail.com
ABSTRACT
Objective: To map the scientific evidence on the configurations of compassionate communities aimed at the care of patients, families, and caregivers with palliative care needs. Method: This is a scoping review conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) and JBI guidelines. The search was performed in the VHL, MEDLINE, SCOPUS, and Web of Science databases using terms related to "Compassionate Communities”. Quantitative and qualitative studies were included, with no language or year of publication restrictions. The selection process was carried out using Rayyan software, and R software was used for bibliometric analysis. Results: The search identified 667 studies, of which 30 were included after screening. The publications, dated between 2013 and 2025, peaked in 2024, with Spain leading the number of studies (n=7). Allan Kellehear is the main theoretical reference. A total of 41 actions were identified, distributed among cultural/educational activities (34.2%), clinical activities (26.3%), and normative, intersectoral articulation, and community mobilization actions (13.1% each). Conclusion: Compassionate communities promote the discussion of death, grief, and palliative care, emphasizing health promotion activities as a central element. They strengthen community support networks for more inclusive and equitable palliative approaches.
Descriptors: Palliative Care; Community Participation; Equity.
|
How to cite: Martins MR, Silva AE, Lima ALA, Jesus MLCSR, Raizaro EP, Silva KL. Configurations of compassionate communities for the provision of palliative care: a scoping review. Online Braz J Nurs. 2025;24(Suppl 2):e20256858. https://doi.org/10.17665/1676-4285.20256858 |
What is already known:
Compassionate communities propose extending palliative care beyond formal health services by integrating community-based actions;
Education on death, dying, grief, and palliative care is a frequent strategy within the scope of compassionate communities;
There are still gaps in the structured provision of bereavement support, especially for individuals not covered by specialized teams.
What this article adds:
Most of the mapped interventions focus on community education and strengthening support networks for care in vulnerable contexts;
Nurses play a central role in care coordination and intersectoral articulation, expanding access to and continuity of palliative care;
Compassionate practices are being incorporated into institutional policies in universities and companies, including benefits for employees and students.
INTRODUCTION
Compassionate communities are developed to support patients, families, and caregivers experiencing illness processes or life-threatening conditions. This movement offers community-based palliative care, with a primary focus on those requiring end-of-life assistance, also extending to issues related to death and bereavement(1-2).
The concept of compassionate communities, introduced by Allan Kellehear in Australia in the early 2000s, is based on the principle that health is a collective responsibility that transcends the exclusive role of health services. In this sense, just as it is fundamental to promote community initiatives aimed at disease prevention, it is also essential to foster palliative care, ensuring the correct identification and adequate treatment of multidimensional suffering(3).
This approach seeks to encourage reflections on the natural process of dying, recognizing it as an inevitable dimension of the human condition. However, it is emphasized that while death is a natural outcome, the unnecessary suffering associated with the course of illness can be prevented through compassionate interventions(4).
Thus, by stimulating initiatives that strengthen social mobilization, such as compassionate communities, residents of certain territories are enabled to actively participate in the construction of mutual care practices within their own communities. As an intersectoral model, compassionate communities encourage the collaboration of schools, community organizations, religious groups, health institutions, as well as patients, families, neighbors, and other citizens to create local support networks(5).
This collaborative movement has been gaining global prominence as an important element in ensuring access to palliative care. Research conducted by Rolston et al.(6) identified a significant increase in the production of studies on interventions related to compassionate communities, particularly in European countries such as the United Kingdom, Austria, Spain, Ireland, Sweden, Germany, Poland, and Portugal. A significant concentration of research was also observed in Canada and Australia. On a smaller scale, studies have been documented in locations such as Taiwan, India, Hong Kong, and Mexico.
Despite the increase in research on compassionate communities and the various interventions identified—including popular education actions in palliative care, cultural gatherings, volunteer initiatives, and clinical and multidimensional interventions(6)—gaps still persist in understanding how these practices can be implemented and adapted in different sociocultural and economic contexts, such as in developing countries and in areas of social vulnerability(5).
Corroborating this perspective, a scoping review aimed at describing the practical implementation of compassionate communities and analyzing the methods for evaluating the effectiveness of their actions highlighted that adaptation to the sociocultural context is the main barrier to their implementation. Among the identified obstacles are local perceptions about asking for and offering help at the end of life, as well as the need to align proposed activities with cultural specificities, such as the language used, religious beliefs, and the inclusion of ethnic minorities in the provision of this type of care(5).
In this context, this review is justified by the need to broaden the understanding of how compassionate communities are configured globally, considering the different economic, social, political, and cultural contexts. Considering these considerations, the following objective was defined: to map the scientific evidence on the configurations of compassionate communities aimed at the care of patients, families, and caregivers with palliative care needs.
METHOD
This is a scoping review developed according to the guidelines of the international guide Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR)(7) and JBI(8), with a protocol registered in the Open Science Framework (OSF).
The study was conducted between February and June 2025, following eight recommended methodological steps: (1) construction of the research protocol; (2) definition of the guiding question; (3) development of search strategies; (4) definition of inclusion criteria; (5) selection of evidence sources; (6) extraction of results; (7) analysis of the evidence; and (8) presentation of the synthesis of the evidence(8).
The research protocol was developed as part of the Scoping Review course offered by the stricto sensu Public Health Graduate Program at the School of Medicine of the Federal University of Minas Gerais. The purpose of the protocol was to define the methodological criteria and ensure the transparency and reproducibility of the review. It was registered with the OSF under the DOI identifier: 10.17605/OSF.IO/JVBP6.
For the definition of the guiding question, the elements of the PCC acronym—Population (P), Concept (C), and Context (C)—proposed for this type of review were used(7-9). Thus, the following research question was defined: "What are the configurations of compassionate communities, in a global context, for the care of patients, families, and caregivers with palliative care needs?" The components of the question were: Population - patients, families, and caregivers with palliative care needs; Concept - configurations of compassionate communities; and Context - global level.
Regarding the construction of the search strategy, the free terms "Comunidade Compassiva”, "Comunidades Compassivas”, "Compassionate Community”, and "Compassionate Communities" were used, combined with the Boolean operator "OR" (Chart 1), in the following databases: Virtual Health Library (VHL), USA National Library of Medicine (MEDLINE/PubMed), SCOPUS, and Web of Science.
Chart 1 - Search strategy. Belo Horizonte, MG, 2025
|
Database |
Search strategy |
|
Virtual Health Library |
"Comunidade Compassiva" OR "Comunidades Compassivas" OR "Compassionate Community" OR "Compassionate Communities" |
|
MEDLINE via PubMeD SCOPUS Web of Science |
"Compassionate Community" OR "Compassionate Communities"
|
|
Search strategy developed by the library service of the Federal University of Minas Gerais on 10/09/2024. |
|
As for the inclusion criteria, the Population (P) was defined as patients, families, and caregivers with palliative care needs. Patients are people who are experiencing serious, progressive, and life-threatening illnesses or conditions, and who may need relief from pain and other physical, psychological, social, and spiritual symptoms. Families and caregivers are part of the support network and therefore need guidance, psychological and social support, and preparation to deal with both the challenges of daily care and the bereavement process.
The Concept (C) corresponds to the configurations of compassionate communities, understood as initiatives that mobilize social networks, civil organizations, and local health services to offer support to people in palliative care. These communities can be realized through different strategies, such as educational activities in palliative care, cultural gatherings, volunteer actions, and clinical interventions.
Finally, the Context (C) refers to the global level. The actions developed by compassionate communities vary according to the historical, social, and economic characteristics of each country.
Therefore, for the selection of evidence sources, studies with quantitative and qualitative approaches were considered, with no restrictions on language or year of publication. Theses, dissertations, manuals, books, and government documents were also eligible. As exclusion criteria, studies that were not conducted in the context of compassionate communities or that only proposed the model without describing its application were disregarded. Additionally, duplicate studies and manuscripts that did not address the guiding question were excluded.
Regarding data extraction, the materials were submitted to an eligibility process using the Rayyan Qatar Computing Research Institute (Rayyan QCRI) software(10), which was used to organize the process of reading and selecting studies. For this, two independent, previously trained researchers evaluated the titles and abstracts of the articles. Subsequently, the included studies were read in full to verify and exclude those that did not meet the established criteria. In cases of doubt about the eligibility of the material, a third trained researcher was called upon for the final decision.
After this step, the data were extracted using a form created by the authors themselves in a Microsoft Excel 2017 spreadsheet. Regarding the analysis and synthesis of the evidence, the data were presented descriptively and critically analyzed considering the literature. Additionally, a bibliometric analysis was performed with the help of R software, which generated visual maps to identify trends and relationships between authors, citations, scientific production by country, among other indicators. This analytical approach favors the visualization of maps that facilitate a better interpretation of the data.
RESULTS
The search strategies resulted in a total of 667 articles. After the exclusion of 393 duplicate studies, 274 remained for analysis. In the first evaluation phase, based on the reading of titles and abstracts, 97 studies were excluded for not describing the application of a compassionate community, addressing the topic only theoretically. Of the 177 articles selected for full-text reading, 30 were included in the final review. Figure 1 presents the flow diagram for each step of the review process.
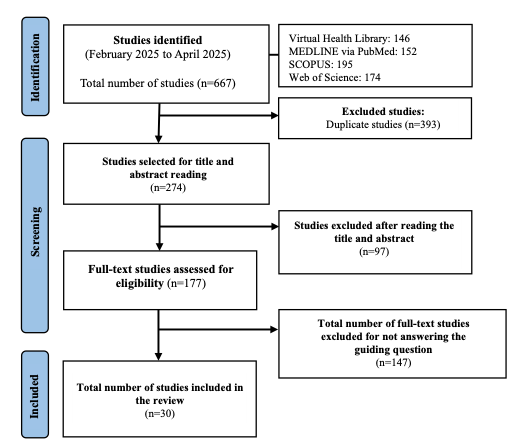
Figure 1 - Flowchart of the literature search and article selection, according to the PRISMA-ScR 2020 guidelines. Belo Horizonte, Minas Gerais, 2025
The analysis of the characteristics of the selected studies indicates a predominance of experience reports (n=8; 26.6%), followed by qualitative studies (n=7; 23.3%) and narrative reviews (n=4; 13.3%). Theoretical studies and mixed methods studies each accounted for (n=3; 10%). Less frequently, quantitative studies (n=2; 6.6%), a case study (n=1; 3.3%), action research (n=1; 3.3%), a scoping review (n=1; 3.3%), and a systematic review of mixed methods (n=1; 3.3%) were identified. The data describing the characteristics of the studies were compiled in Chart 2.
Chart 2 - Characteristics of the selected studies. Belo Horizonte, MG, 2025
|
ID* |
Title |
Year |
Country |
Journal |
Type of study |
|
1 |
Assessing and comparing compassionate communities benefits across cities in diverse cultural contexts: a step toward the identification of the most important ones(11) |
2025 |
Switzerland; Argentina; Colombia |
Palliative Care & Social Practice. |
Mixed methods study |
|
2 |
A compassionate university for serious illness, death, and bereavement: Qualitative study of student and staff experiences and support needs(12) |
2024 |
Belgium |
Death Studies |
Qualitative study |
|
3 |
A dimensão espiritual de pacientes em cuidados paliativos e seus cuidadores de uma comunidade compassiva de favela: estudo de método misto(13) |
2024 |
Brazil |
Portal Regional da BVS |
Mixed methods study |
|
4 |
Advanced practice nursing in palliative care within the compassionate favela community: an experience report(14) |
2024 |
Brazil |
Online Brazilian Journal of Nursing |
Experience report |
|
5 |
Age-Friendly Communities: Are they also "Friendly" for Death, Dying, Grief, and Bereavement?(15) |
2024 |
Canada |
Canadian Journal on Aging La Revue canadienne du vieillissement |
Theoretical study |
|
6 |
Barriers and drivers of public engagement in palliative care, Scoping review(16) |
2024 |
Spain |
BMC Palliative Care |
Scoping review |
|
7 |
Belonging, care, and support: findings from Ottawa's healthy end of life project(17) |
2024 |
Canada |
Journal of Religion Spirituality & Aging |
Case study |
|
8 |
Caring neighbourhoods in Belgium: lessons learned on the development, implementation and evaluation of 35 caring neighbourhood projects(18) |
2024 |
Belgium |
Palliative Care & Social Practice |
Qualitative study |
|
9 |
Comunidades Compassivas: uma resposta aos desafios em Cuidados Paliativos(19) |
2024 |
Portugal |
Motricidade |
Qualitative study |
|
10 |
Bereavement care reimagined(20) |
2023 |
United Kingdom, United States, Australia |
Annals of Palliative Medicine |
Narrative review |
|
11 |
Comunidades Compasivas: intervención comunitaria para la prevención del duelo complicado. Modelo implantado por Madrid Salud. Psicooncología(21) |
2023 |
Spain |
Psicooncología |
Mixed methods study |
|
12 |
Civic engagement in serious illness, death, and loss: A systematic mixed-methods review(22) |
2022 |
Belgium |
Palliative Medicine |
Systematic review of mixed methods |
|
13 |
Community Based Participatory Research For The Development of a Compassionate Community: The Case of Getxo Zurekin(23) |
2022 |
Spain |
International Journal of Integrated Care |
Action research |
|
14 |
A Compassionate Communities Approach(24) |
2021 |
Mexico |
Journal of Social Work in End-of-Life & Palliative Care |
Quantitative study |
|
15 |
Centering sexual and gender diversity within Compassionate Communities: insights from a community network of LGBTQ2S+ older adults(25) |
2021 |
Canada |
Palliative Care and Social Practice |
Qualitative study |
|
16 |
A Public Health Approach to Palliative Care in the Canadian Context(26) |
2020 |
Canada |
American Journal of Hospice & Palliative Medicine |
Qualitative study |
|
17 |
Bereavement support: From the poor cousin of palliative care to a core asset of compassionate communities(27) |
2020 |
Australia |
Progress in Palliative Care |
Quantitative study |
|
18 |
Choice depends on options: A public health framework incorporating the social determinants of dying to create options at end of life(28) |
2020 |
Australia |
Progress in Palliative Care |
Theoretical study |
|
19 |
Compassionate communities and collective memory: A conceptual framework to address the epidemic of loneliness(29) |
2019 |
United Kingdom |
British Journal of Community Nursing |
Theoretical study |
|
20 |
Comunidades compasivas en Colombia para el apoyo a personas con enfermedad avanzada y al final de la vida: uniendo esfuerzos(30) |
2019 |
Colombia |
Medicina Paliativa |
Experience report |
|
21 |
All with you: A new method for developing compassionate communities—experiences in Spain and Latin-America(31) |
2018 |
Spain |
Annals of Palliative Medicine |
Experience report |
|
22 |
A new method for developing compassionate communities and cities movement-"Todos Contigo" Programme (We are All With You): experience in Spain and Latin America countries(32) |
2018 |
Spain |
Annals of Palliative Medicine |
Experience report |
|
23 |
Building a narrative for compassionate communities: the case of Getxo Zurekin(33) |
2018 |
Spain |
International Journal of Integrated Care |
Qualitative study |
|
24 |
Celebrating indigenous communities compassionate traditions(34) |
2018 |
Canada |
Annals of Palliative Medicine |
Experience report |
|
25 |
Compassionate communities: Design and preliminary results of the experience of Vic (Barcelona, Spain) caring city(35) |
2018 |
Spain |
Annals of Palliative Medicine |
Experience report |
|
26 |
Compassionate communities in Canada: It is everyone’s responsibility(36) |
2018 |
Canada |
Annals of Palliative Medicine |
Narrative review |
|
27 |
Compassionate Communities - From frailty to community resilience – making a public health approach to end of life care a reality(37) |
2017 |
United Kingdom |
International Journal of Integrated Care |
Experience report |
|
28 |
Comunidades compasivas en cuidados paliativos: Revisión de experiencias internacionales y descripción de una iniciativa en Medellín, Colombia(38) |
2017 |
Colombia |
Psicooncología |
Narrative review |
|
29 |
Compassionate communities: Case studies from Britain and Europe(39) |
2016 |
United Kingdom |
Routledge Key Themes in Health and Society |
Experience report |
|
30 |
Compassionate communities: End-of-life care as everyone's responsibility(3) |
2013 |
United Kingdom |
QJM (Quarterly Journal of Medicine) |
Narrative review |
*ID: identification.
Regarding the publication period, the selected studies were published between 2013 and 2025. The year 2024 stood out with the highest number of publications (n=8; 26.7%), which indicates a recent increase in interest in the topic (Figure 2).
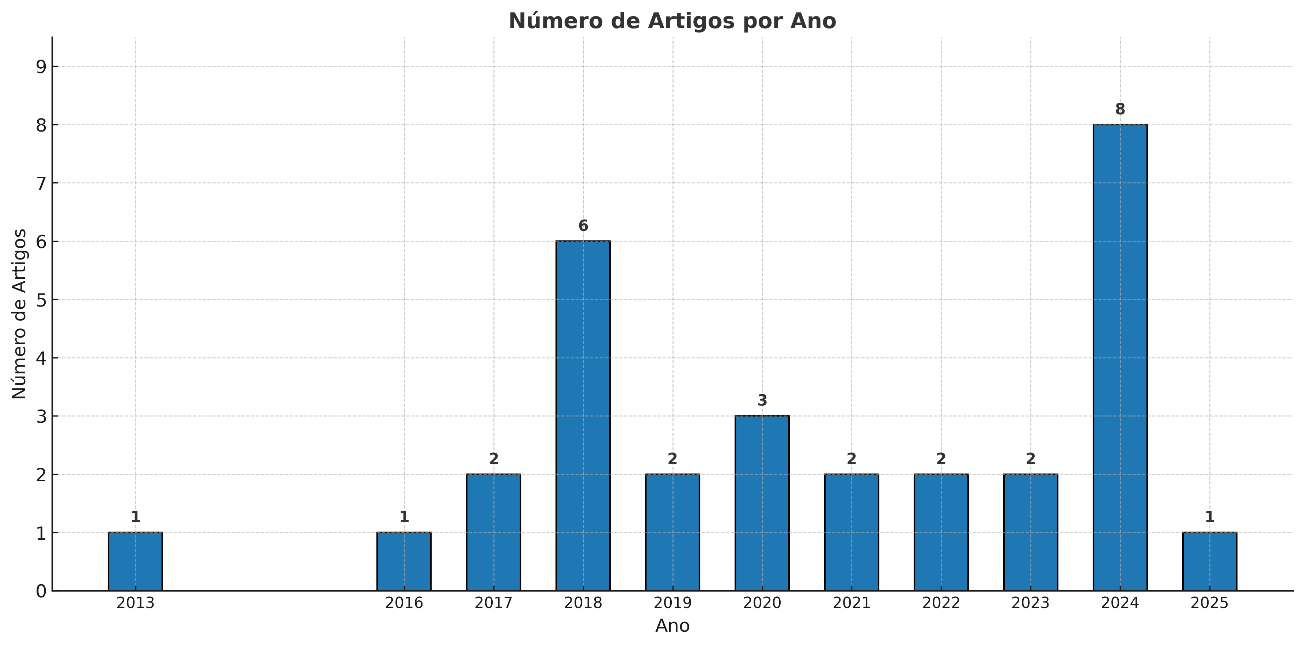
Figure 2 - Distribution of study publications by year. Belo Horizonte, MG, 2025
The average number of citations per article was 25.8, with the study by Allan Kellehear(3) standing out, having accumulated 334 citations as of April 2025 (Figure 3).
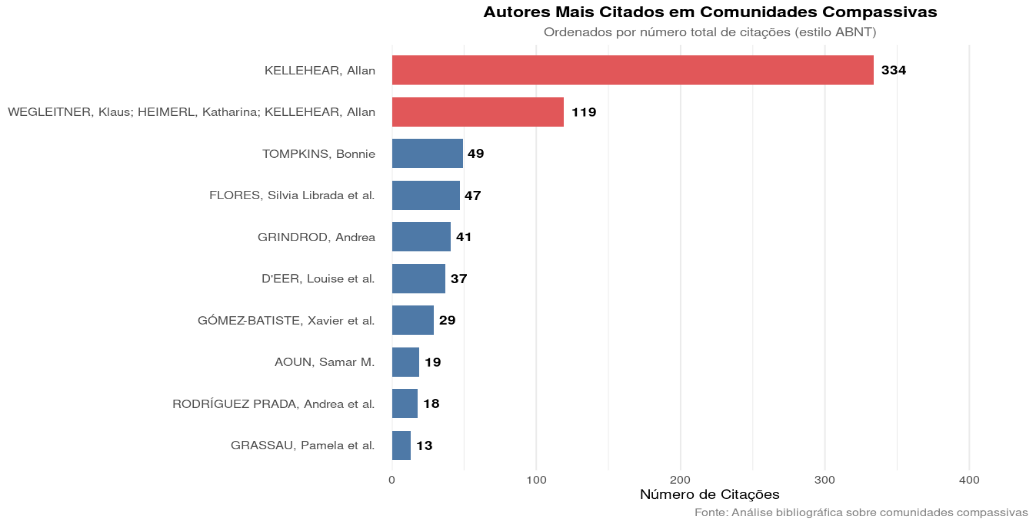
Figure 3 - Relationship of most cited authors. Belo Horizonte, MG, 2025.
The analysis of the co-authorship network reveals little connection between authors, demonstrating that the topic is still studied in isolation by different research groups (Figure 4).

Figure 4 - Integration network among the authors. Belo Horizonte, MG, 2025
Regarding the geographical distribution of publications (Figure 5), Spain stood out with the highest number of studies (n=7), followed by Canada (n=5) and the United Kingdom (n=4). Six other countries were represented, including Brazil (n=2). Additionally, two studies were multicenter, involving Switzerland, Argentina, and Colombia in one, and the United Kingdom, United States, and Australia in the other.
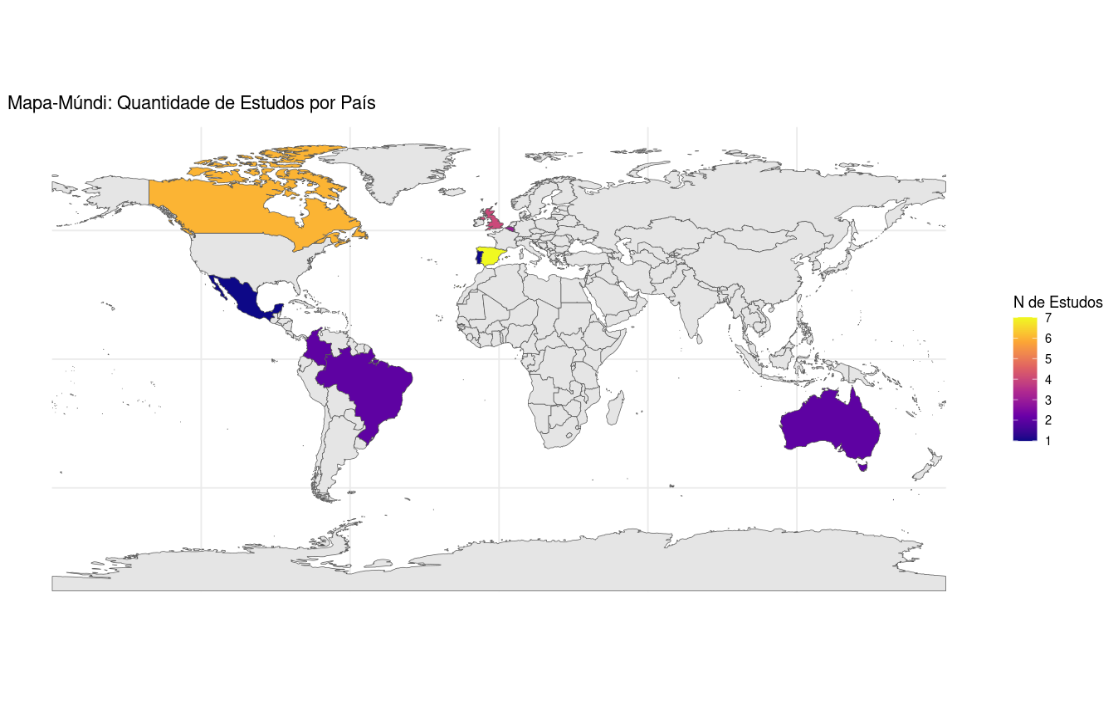
Figure 5 - World map with the number of studies per country. Belo Horizonte, MG, 2025
The analyzed evidence indicates that the actions developed by compassionate communities vary according to the social, cultural, and economic characteristics and the specific palliative care needs in each context. Interventions occur in different settings—community, home, outpatient, and hospital—and are distributed among cultural and educational practices (34.2%), clinical (26.3%), normative (13.1%), intersectoral articulation (13.1%), and community mobilization (13.1%), as systematized in Chart 3.
Chart 3 - Description of actions carried out in the context of compassionate communities. Belo Horizonte, MG, 2025
|
Thematic categories |
Actions carried out in the context of compassionate communities
|
Study identification |
|
Cultural and educational |
Popular education on palliative care for the community |
E3; E4; E10; E11; E12; E13; E14; E16; E20; E21; E22; E24; E27; E28 |
|
Educational activities on death and bereavement in schools |
E5; E9; E13; E26; E28; E29 |
|
|
Educational activities on death and bereavement in universities |
E9; E14; E20 |
|
|
Training on death and bereavement for teachers |
E21 |
|
|
Health education for family members of patients with palliative care needs |
E7; E8 |
|
|
Health education on palliative care in the context of diversity |
E15 |
|
|
Professional training actions on palliative care |
E11; E18; E20; E21 |
|
|
Art exhibitions for the celebration of life and understanding of death |
E1; E5; E13; E21; E25 |
|
|
Awareness campaigns on death and bereavement in schools |
E21 |
|
|
Community parties for welcoming new neighbors |
E8 |
|
|
Valuing traditional funeral ritual practices in indigenous communities |
E24 |
|
|
Death Cafés |
E13; E20; E27 |
|
|
Intergenerational actions involving local memory and tradition |
E19 |
|
|
Clinical |
Bereavement intervention groups led by psychologists and social workers |
E14 |
|
Home care by multiprofessional teams for the control of multidimensional symptoms |
E3; E4; E25; E27 |
|
|
Nursing home visits for symptom management and control |
E4 |
|
|
Nursing consultations via telemonitoring for symptom management and control |
E4 |
|
|
Care model based on traditional and scientific knowledge |
E24 |
|
|
Support by psychologists and social workers in the final phase of life and bereavement |
E11 |
|
|
Multiprofessional palliative home care integrated with support from informal caregivers |
E3; E4; E28 |
|
|
Early palliative care approach aimed at symptom prevention |
E26 |
|
|
Hospital palliative care approach for people living with HIV/AIDS |
E28 |
|
|
Outpatient palliative care and rehabilitation approach for people living with HIV/AIDS |
E28 |
|
|
Intersectoral articulation |
Support in the transition from hospital to home care by informal caregivers |
E6 |
|
Care management by nurses for articulation with the local health care network |
E4 |
|
|
Consultations using telemonitoring by external program supporters |
E3 |
|
|
Donations of health care supplies and social support by external program supporters |
E3; E19 |
|
|
Integration of community resources with the local health care network |
E1; E3; E4; E9; E12; E13; E15; E17; E18; E20; E23; E29; E30 |
|
|
Normative |
Creation of compassionate universities with the development of institutional policies aimed at supporting illness, death, and bereavement for students and workers |
E2 |
|
Consultancies for the creation of local public policies aimed at death and bereavement |
E5; E16 |
|
|
Creation of observatories for monitoring and evaluation with criteria for the certification of cities and institutions as "Compassionate Communities" |
E21; E22 |
|
|
Creation of public and institutional policies with funding to foster the development of compassionate communities |
E28 |
|
|
Creation of compassionate companies with the development of institutional policies for workers who care for family members in the final phase of life |
E20; E26 |
|
|
Community mobilization |
Home visits by informal caregivers to reduce the isolation of people in the final phase of life |
E5; E6; E16 |
|
Formation of networks of informal caregivers for palliative care |
E3; E4; E1; E16; E21; E22 |
|
|
Creation of informal care networks that assist in the access of people in palliative care and the socially vulnerable to local health services |
E7; E12; E18; E25; E27 |
|
|
Creation of bereavement support groups led by bereaved individuals for interaction between neighbors |
E13 |
|
|
Integration of volunteers in support and care activities for people with dementia |
E28 |
DISCUSSION
Across the studies, it is observed that the theoretical foundation of the actions undertaken is anchored in Allan Kellehear(3), who stands out as the main conceptual reference adopted by researchers. The author proposes an expansion of the understanding of palliative care, conceiving it as a health promotion strategy, which enables its incorporation into community contexts and not just in institutions.
Considering this, it is noted that a large portion of the mapped interventions (34.2%) focuses on activities aimed at fostering community education in palliative care and on cultural activities about death, dying, and bereavement. Among the identified strategies are educational actions developed in educational institutions, such as schools and universities, and specific training for teachers, aiming to qualify the pedagogical approach to these topics in the school environment(5,15,19,23-24,30-31,36,38).
Furthermore, there are palliative care education initiatives aimed at the context of sexual and gender diversity(25), as well as training actions for professionals from different areas, focusing on qualification for palliative care(21,28,30-32). In the cultural sphere, noteworthy activities include intergenerational activities between children and the elderly, aimed at addressing social isolation and centered on valuing local memory and traditions(29); festivities with the purpose of welcoming new neighborhood residents as a way to strengthen neighborhood bonds(18); and also practices that recover and respect traditional funeral rituals, as in indigenous communities(34).
These strategies seek to promote greater public awareness regarding the finitude of life and the shared responsibility in caring for people with weakened support networks. Additionally, they aim to stimulate reflection on inevitable aspects of the human experience, such as aging and death, fostering more receptive and supportive attitudes towards these processes(11,20-21).
Beyond cultural and educational activities, palliative care practices by multiprofessional health teams were also recorded in home(13-15,35,37-38), outpatient, and hospital settings(38). The distinguishing feature of some of these proposals is the formation of a community support network, in which citizens (neighbors) from the territory itself assist the teams in monitoring patients(13-14,38).
In this scenario, nurses stand out for their clinical reasoning and ability to manage care. They use standardized instruments for the assessment and management of physical, psychological, and spiritual symptoms, both in face-to-face and telemonitoring consultations. Furthermore, they adapt procedures to the social realities of patients, expanding access to and continuity of palliative care, especially in vulnerable contexts. In this process, they also guide and train informal caregivers to perform basic care, contributing to the safety and quality of care provided at home(13-14).
In addition to this, care in the bereavement process also emerged as a recurring practice within compassionate communities. Studies(21,24,27) reveal that although the approach to bereavement is aligned with the philosophy of palliative care, many services still lack well-defined structures for its implementation. Moreover, when people are not followed by palliative care teams, they rarely have access to the necessary support for managing grief.
In this sense, the authors adopted the principles of compassionate communities to develop programs aimed at bereavement support in the communities, promoting free and public meetings with spaces for listening, sharing, and psychoeducation. Likewise, they established psychological and social work support at home for patients and families experiencing life-threatening conditions or illnesses, aiming to prevent complicated grief in places with weaknesses in the health care network(21,24,27).
In the context of intersectoral articulation activities, it is observed that in many studies, the integration of community resources with the local health care network is one of the premises for implementing compassionate communities(11,13-14,19,22-23,25,28,30,33,39). This aspect reinforces that this type of approach does not replace the duty of public bodies in ensuring coverage and access to palliative care services but is created to strengthen this network(40).
Examples of these initiatives include support in the transition of care from the hospital to the home, carried out by previously guided informal caregivers(16), and care management conducted by nurses, who articulate with the different points of the health care network(14). Furthermore, the use of telemonitoring for consultations with the support of external program supporters is observed, expanding access to care by professionals from various specialties(13).
Another relevant aspect is community mobilization, which is expressed in initiatives such as donations of supplies and social support, highlighting the engagement of different sectors for the sustainability of compassionate initiatives(13,29). These actions include home visits by informal caregivers to reduce the isolation of people in the final phase of life(15-16,26), the formation of support networks for palliative care, the articulation of community groups that assist socially vulnerable people in accessing health services(11,13-14,26,31-32), the creation of bereavement support spaces led by bereaved individuals(17,22,28,35,37), and the integration of volunteers in support activities for individuals with dementia(38).
Not limited to issues related to culture, education, and health, the philosophy of compassionate communities has been gaining ground in the normative context, in university institutions(12) and companies(30,36). In these contexts, the virtue of compassion, defined(29) as the human capacity to recognize the suffering of another and act to alleviate it, has been incorporated into the creation of institutional policies that support students and employees during processes of illness and bereavement of family members or close ones.
A qualitative study(12) conducted at a compassionate university in Belgium explored the experiences and support needs of students and staff facing serious illness, death, and bereavement. Although there are institutional policies that provide for academic flexibility, medical leave, and psychological support, the results indicate that barriers persist, such as the lack of sensitivity of some professors and managers, especially in non-family losses. Difficulties in locating clear information about available services and limitations in the use of technologies, such as the automated chatbot, whose impersonality discourages the search for support, were also pointed out.
In the corporate sphere, compassion has been incorporated as an organizational value, reflected in initiatives that promote mutual support among colleagues and in the institutional recognition that processes such as illness, death, and bereavement are part of the workers' experience and must be respected(30). In this regard, the federal government of Canada has stood out since 2004 by encouraging institutions to support employees responsible for people in palliative care(36).
Through the compassionate care benefit, funded by federal employment insurance, workers can request paid leave of up to 26 weeks to accompany loved ones in the final phase of life. However, due to the provincial management of labor codes, job security during this period is not yet guaranteed in all regions of the country(36).
Some organizations, such as the New Health Foundation (NHF), have been developing certifications and accreditations for compassionate companies in the corporate sphere, with the definition of criteria to guide the implementation of institutional policies aligned with the philosophy of palliative care. The NHF has created programs such as NewPalex®, All with You®, and iNewCare®, aimed at strengthening organizational practices that integrate health, social support, and end-of-life care, also considering the care of workers. It is a management system that involves the organization, its employees, patients, and the community(31).
CONCLUSION
The philosophy of compassionate communities promotes the integration of palliative care with social and cultural support in the communities, recognizing the importance of dealing with the finitude of life in a supportive and compassionate manner. The approach focuses on building support networks, raising awareness about death, bereavement, and end-of-life care, and including all social actors involved: patients, families, citizens, and professionals. Although progress is evident, there are still challenges to be overcome, mainly in integrating this philosophy into the culture and institutional agendas.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
REFERENCES
1. Neighborhood Centres Queensland. Compassionate communities: an implementation guide for community approaches to end of life care [Internet]. Queensland (AU): NOUS; 2018 [cited 2025 Jan 10]. Available from: https://ncq.org.au/resources/compassionate-communities-an-implementation-guide-for-community-approaches-to-end-of-life-care/
2. Mesquita MG da R, Silva AE, Coelho LP, Martins MR, Souza MT de, Trotte LAC. Slum compassionate community: expanding access to palliative care in Brazil. Rev Esc Enferm USP. 2023;57:e20220432. https://doi.org/10.1590/1980-220X-REEUSP-2022-0432en
3. Kellehear A. Compassionate communities: end-of-life care as everyone’s responsibility. QJM. 2013;106(12):1071-1075. https://doi.org/10.1093/qjmed/hct200
4. Abel J. Compassionate communities and end-of-life care. Clin Med (Lond). 2018;18(1):6-8. https://doi.org/10.7861/clinmedicine.18-1-6
5. Dumont K, Marcoux I, Warren É, Alem F, Alvar B, Ballu G, et al. How compassionate communities are implemented and evaluated in practice: a scoping review. BMC Palliat Care. 2022;21(1):131. https://doi.org/10.1186/s12904-022-01021-3
6. Roleston C, Shaw R, West K. Compassionate communities interventions: a scoping review. Ann Palliat Med. 2023;12(5):936-951. https://doi.org/10.21037/apm-22-867
7. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467-473. https://doi.org/10.7326/M18-0850
8. Peters MD, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Scoping reviews. In: Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editores. JBI Manual for Evidence Synthesis. Adelaide: JBI; 2024. https://doi.org/10.46658/JBIMES-24-09
9. Araújo WCO. Recuperação da informação em saúde: construção, modelos e estratégias. Conci. 2020;3(2):100-134. https://doi.org/10.33467/conci.v3i2.13447
10. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. https://doi.org/10.1186/s13643-016-0384-4
11. González-Jaramillo V, Krikorian A, Tripodoro V, Jorge M, Orellana S, López F, et al. Assessing and comparing compassionate communities benefits across cities in diverse cultural contexts: a step toward the identification of the most important ones. Palliat Care Soc Pract. 2025;19:26323524251314899. https://doi.org/10.1177/26323524251314899
12. Bakelants H, Droogenbroeck FV, Chambaere K, Vanderstichelen S, De Donder L, Deliens L, et al. A compassionate university for serious illness, death, and bereavement: Qualitative study of student and staff experiences and support needs. Death Stud. 2024;48(5):442-453. https://doi.org/10.1080/07481187.2023.2233495
13. Souza MT. A dimensão espiritual de pacientes em cuidados paliativos e seus cuidadores de uma comunidade compassiva de favela: estudo de método misto [master’s thesis]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2024.
14. Silva AE, Almeida AR, Martins MR, Oliveira TM de, Mesquita MG da R, Trotte LAC. Advanced practice nursing in palliative care within the compassionate favela community: an experience report. Online Braz J Nurs. 2024;22(Suppl2):e20246690. https://doi.org/10.17665/1676-4285.20246690
15. Brassolotto J, Banerjee A. Age-Friendly Communities: Are they also “Friendly” for Death, Dying, Grief, and Bereavement? Can J Aging. 2024;43(2):311-318. https://doi.org/10.1017/s0714980823000624
16. Barnestein-Fonseca P, Nebro-Gil A, Aguiar-Leiva VP, Víbora-Martín E, Ruiz-Torreras I, Martín-Rosello ML, et al. Barriers and drivers of public engagement in palliative care, Scoping review. BMC Palliat Care. 2024;23(1):117. https://doi.org/10.1186/s12904-024-01424-4
17. Van Vliet L, Grassau P, Mercer L, Miloff H, Nelson-James A, Mayo C, et al. Belonging, care, and support: findings from Ottawa’s healthy end of life project. J Relig Spiritual Aging. 2024;36(4):424-438. https://doi.org/10.1080/15528030.2024.2375355
18. De Donder L, Stegen H, Hoens S. Caring neighbourhoods in Belgium: lessons learned on the development, implementation and evaluation of 35 caring neighbourhood projects. Palliat Care Soc Pract. 2024;18:26323524241246533. https://doi.org/10.1177/26323524241246533
19. Leão D, Carqueja E. Comunidades Compassivas: uma resposta aos desafios em Cuidados Paliativos. Motricidade. 2024;20(1):36-44. https://doi.org/10.6063/motricidade.33970
20. Abel J, Kellehear A, Aoun SM. Bereavement care reimagined. Ann Palliat Med. 2023;12(4):816-825. https://doi.org/10.21037/apm-23-24
21. Carrascosa Pujalte E, Valero Herranz E, Adán Pérez E, Garrido Sanz V, Trujillo Mejía X, Plaza Bedmar G, et al. Comunidades Compasivas: intervención comunitaria para la prevención del duelo complicado. Modelo implantado por Madrid Salud. Psicooncología. 2023;20(1):87-102. https://doi.org/10.5209/psic.87572
22. D’Eer L, Quintiens B, Van den Block L, Dury S, Deliens L, Chambaere K, et al. Civic engagement in serious illness, death, and loss: A systematic mixed-methods review. Palliat Med. 2022;36(4):625-651. https://doi.org/10.1177/02692163221077850
23. Hasson N, Urtaran-Laresgoiti M, Nuño-Solinís R, Moreno I, Espiau G, Grajales M, et al. Community based participatory research for the development of a compassionate community: the case of Getxo Zurekin. Int J Integr Care. 2022;22(1):2. https://doi.org/10.5334/ijic.5707
24. Zuniga-Villanueva G, Ramirez-GarciaLuna JL, Villafranca-Andino RI. A Compassionate Communities Approach in a Grief and Bereavement Support Program: Bridging the Gap in Palliative Care. J Soc Work End Life Palliat Care. 2021;17(1):9-18. https://doi.org/10.1080/15524256.2021.1894309
25. Grassau P, Stinchcombe A, Thomas R, Wright DK. Centering sexual and gender diversity within Compassionate Communities: insights from a community network of LGBTQ2S+ older adults. Palliat Care Soc Pract. 2021;15:26323524211042630. https://doi.org/10.1177/26323524211042630
26. Sirianni G. A public health approach to palliative care in the Canadian context. Am J Hosp Palliat Care. 2020; 37(7):492-496. https://doi.org/10.1177/1049909119892591
27. Aoun SM. Bereavement support: from the poor cousin of palliative care to a core asset of compassionate communities. Prog Palliat Care. 2020;28(2):107-114. https://doi.org/10.1080/09699260.2019.1706277
28. Grindrod A. Choice depends on options: A public health framework incorporating the social determinants of dying to create options at end of life. Prog Palliat Care. 2020;28(2):94-100. https://doi.org/10.1080/09699260.2019.1705539
29. Sime C, Collins S. Compassionate communities and collective memory: a conceptual framework to address the epidemic of loneliness. Br J Community Nurs. 2019;24(12):580-584. https://doi.org/10.12968/bjcn.2019.24.12.580
30. Samudio ML, Krikorian A, Vélez MC, Flores SL, Agudelo V, Franco M, et al. Comunidades compasivas en Colombia para el apoyo a personas con enfermedad avanzada y al final de la vida: uniendo esfuerzos. Med. paliat. (Internet). 2019;26(4):309-317. https://doi.org/10.20986/medpal.2019.1099/2019
31. Flores SL, Molina EH, Osuna JB, Vargas RM, Vicuña MN. All with You: a new method for developing compassionate communities—experiences in Spain and Latin-America. Ann Palliat Med. 2018;7(S2):S15-S31. https://doi.org/10.21037/apm.2018.03.02
32. Flores SL. A new method for developing compassionate communities and cities movement—“Todos Contigo” Programme (We are All With You): experience in Spain and Latin America countries. Ann Palliat Med. 2018;7(Suppl 1):AB004. https://doi.org/10.21037/apm.2018.s004
33. Hasson N, Grajales M, Grajales I, Espiau G, Nuño R, Urtaran M. Building a narrative for compassionate communities: the case of Getxo Zurekin. Int J Integr Care. 2018;18(S2):A321. https://doi.org/10.5334/ijic.s2321
34. Prince H. Celebrating indigenous communities compassionate traditions. Ann Palliat Med. 2018;7(Suppl 1):AB005. https://doi.org/10.21037/apm.2018.s005
35. Gómez-Batiste X, Mateu S, Serra-Jofre S, Molas M, Mir-Roca S, Amblàs J, et al. Compassionate communities: design and preliminary results of the experience of Vic (Barcelona, Spain) caring city. Ann Palliat Med. 2018;7(Suppl 2):S32-S41. https://doi.org/10.21037/apm.2018.03.10
36. Tompkins B. Compassionate Communities in Canada: it is everyone’s responsibility. Ann Palliat Med. 2018;7(S2):S118-S129. https://doi.org/10.21037/apm.2018.03.16
37. Morris L, McDaid M. Compassionate Communities - From frailty to community resilience – making a public health approach to end of life care a reality. Int J Integr Care. 2017;17(5):134. https://doi.org/10.5334/ijic.3442
38. Prada AR, Gómez JC, Daveloza AK, Benjumea AZ. Comunidades compasivas en cuidados paliativos: revisión de experiencias internacionales y descripción de una iniciativa en Medellín, Colombia. Psicooncología. 2017;14(2-3):325-342. https://doi.org/10.5209/PSIC.57089
39. Wegleitner K, Heimerl K, Kellehear A, editors. Compassionate communities: case studies from Britain and Europe (Routledge key themes in health and society). New York: Routledge; 2017.
40. Martins MR, Velloso ISC, Almeida BC de, Silva AE. Making People Live or Letting Them Die? Biopolitics and Palliative Care for Older Persons Living in Slums in Brazil. J Aging Soc Policy. 2025;37(5):953-971. https://doi.org/10.1080/08959420.2025.2462325
Submission: 30-Jul-2025
Approved: 15-Sep-2025
Editors:
Rosimere Ferreira Santana (ORCID: 0000-0002-4593-3715)
Geilsa Soraia Cavalcanti Valente (ORCID: 0000-0003-4488-4912)
Érica Brandão de Moraes (ORCID: 0000-0003-3052-158X)
Corresponding author: Matheus Rodrigues Martins (matheusrodrigues355@gmail.com)
Publisher:
Escola de Enfermagem Aurora de Afonso Costa – UFF
Rua Dr. Celestino, 74 – Centro, CEP: 24020-091 – Niterói, RJ, Brazil
Journal email: objn.cme@id.uff.br
|
AUTHORSHIP CONTRIBUTIONS |
|
Study conception: Martins MR, Silva AE, Lima ALA, Jesus MLCSR, Raizaro EP, Silva KL. Data acquisition: Martins MR, Lima ALA, Jesus MLCSR, Raizaro EP. Data analysis: Martins MR, Silva AE, Lima ALA, Jesus MLCSR, Raizaro EP, Silva KL. Data interpretation: Martins MR, Lima ALA, Jesus MLCSR, Raizaro EP. All authors are responsible for drafting the manuscript, critically revising its intellectual content for the final published version, and ensuring the study’s accuracy and integrity with regard to ethical, legal, and scientific aspects. |
