Tele-care in post-discharge follow-up of elderly people with dementia and their caregivers: quasi-experimental study
Rosimere Ferreira Santana1, Thais da Silva Soares1, Carla Targino Bruno dos Santos2, Ana Beatriz Serra Hercules1, Mirian da Costa Lindolpho1, Yolanda Elisa Moreira Boechat1
1 Federal Fluminense University
2 University of Brasilia
ABSTRACT
Objective: To analyze the effect of tele-care in reducing the burden of caregivers and in maintaining the functional and behavioral capacity of the elderly after hospital discharge. Method: Quantitative, quasi-experimental research, with anterior-posterior design, involving Telecare as an intervention. Result: Post-test evaluations demonstrated that the intervention was effective in reducing the burden of caregivers Zarit (p-value <0.001); in the Neuropsychiatric Inventory (NPI) there was a change in the item Distress (p-value = 0.002) demonstrating the improvement in the coping of caregivers through behavioral changes; however, the Prisma 7 tests (p-value = 0.002) showed a difference, however, due to the change in the age factor of the elderly; and in KATZ 70% of the patients did not change, for 25% the score decreased and for 5% the score increased. In global analysis, the change in KATZ was not statistically significant (p-value = 0.102). Conclusion: However, the data from this study demonstrated that the Tele-care reduced the burden and distress of caregivers, and maintaining the capacity to perform the activities of daily living of the elderly.
Descriptors: Telemedicine; Elderly health; Alzheimer's disease; Geriatric nursing.
INTRODUCTION
The population aging process in Brazil has been highlighted as one of the greatest challenges today, as it is related to a growing social and economic demand. In the Brazilian scenario, about 85% of the elderly have at least one chronic disease and 10% of these have comorbidities; among chronic non-communicable diseases (NCDs) that affect people in the aging phase, dementias stand out for having characteristics that not only affect the sick individual, but extend to the entire family structure and society, causing them great psychosocial and economic impact (1).
Dementia is of greater importance as a health problem due to the increase in the contingent of the aging population worldwide, particularly in the age group of 80-year- olds (2). Epidemiological data indicate that more than 24 million people suffer from some dementia in the world and that this estimate may exceed 80 million in 2040 (3).
Dementia causes changes such as the deteriorating evolution of the patient which causes them to be increasingly dependent on care and without autonomy to perform simple daily activities, requiring the presence of a caregiver (3).
Living with elderly people with dementia requires a significant change in family dynamics, as the new needs of the sick family member need to be included in the daily lives of everyone involved in this process. Generally, a single person occupies the role of caregiver, whether by instinct or will, availability or capacity. He then becomes the primary caregiver and assumes care tasks, meeting the needs of the elderly and taking responsibility for them (4).
Nursing guidance on home care is fundamental to the quality of life of the elderly and their family, since there is a physical and emotional burden on those who offer care, and requires the implementation of specific nursing techniques such as positioning, bathing, feeding, skin care, etc. Family demands usually revolve around the management of the elderly with dementia and subsequent behavioral disorders. Thus, the physical, emotional and socioeconomic burden of caring for a family member is immense (5).
In this context, with regard to the caregiver's health, it can be highlighted, in addition to the burden, the accumulation of activities, the lack of housing structure, high costs for the family caregiver with the care of the elderly, the inadequacies in the health system and social isolation of both the elderly and the caregiver can all be mentioned. It is possible to understand that the aforementioned problems are just some of the factors that contribute to increased tension and stress, culminating in an increased feeling of burden (6).
Thus, it is essential that health professionals train the caregiver and support them to perform the care activities necessary for the elderly's daily life until they feel safe to do so (5). However, due to the difficulties encountered in transporting the elderly with dementia to the health unit, making appointments, as well as periodic home visits by the health team (7), the use of assisted technologies, such as tele-care or telemonitoring, can be a promising and viable alternative with regard to monitoring the elderly with dementia and their caregivers.
Telecare consists of an integrated system and defines health activities that can be carried out remotely. This monitoring can be performed through virtual consultations, video conferencing, telephone calls and cell phone text messages (8), resulting in reducing the need for community care, avoiding unnecessary hospital admission; delaying or preventing admission to residential or nursing care.
According to a systematic review study (6); there are only two articles that address tele-care with the nurse's performance (9 - 10). Through the use of tele-care, it is noted that the caregivers accepted it since the research results were positive (6). There was an increase in the number of patients monitored, better understanding of the practical and emotional impact of dementia on daily life, greater confidence in providing care with improved care skills, and reduced caregiver burden. Telecare has been an intervention of paramount importance, since it increases the speed of access between professional-patient, decreases waiting time and travel costs for face-to-face consultations.
There was also a positive feedback from caregivers when there was direct action by the nurse in distance monitoring (6; 9-10). With this, it can be seen that the distance monitoring by means of assisted technologies tends to be increasingly used and are aimed at better results in the daily life of the caregiver-elderly dyad.
Despite the lack of articles on the use of tele-care for elderly people with dementia and their caregivers with the role of nurses, the articles found describe the use of technologies as a viable alternative in providing quality care and easy access in monitoring elderly people with dementia and their caregivers (6; 9-10).
Therefore, the objective of the study was to analyze the effect of tele-care on the burden on the caregiver and on the functional and behavioral capacity of the elderly person after hospital discharge.
METHOD
This is a quantitative, quasi-experimental research, with an anterior-posterior design, involving the intervention of “tele-care” in elderly people with dementia and their caregivers after hospital discharge.
All participants in this study were initially submitted to a data production instrument composed of instruments suitable for this population, internationally recognized and validated in the Portuguese language: a) Caregivers: Caregiver Burden Inventory - ZARIT; b) Elderly: collection of detailed clinical history; physical exam; PRISMA-7; Neuropsychiatric Inventory; Evaluation of Basic Activities of Daily Living - KATZ.
Thus, all the necessary data were obtained for the selection of volunteers who meet the criteria: Inclusion criteria: a) Elderly: Hospitalized for clinical reasons; Secondary diagnosis: Dementia; Have a primary caregiver; Be accompanied by the Integrated Prevention Unit (UIP); Be over 65 years of age and, have a Mini Mental State Examination - MMSE less than or equal to 26; b) Caregiver: Caregiver is available for guidance; have cognitive ability to respond in time and place for this interface with the researcher and accept to participate in clinical research. Exclusion criteria: a) Elderly: Having clinical instabilities such as, for example, oxygen cylinder, decompensated Congestive Heart Failure, congestive obstructive pulmonary disease, cerebrovascular diseases, psychiatric diseases and being in exclusive palliative care; b) Caregivers: Have an auditory deficit that limits communication by phone and\or video call through the WHATSAPP® application; and caregiver with untreated psychiatric disorder. Discontinuity Criteria: Answering at least 75% of calls.
The research was carried out in a Philanthropic Hospital Network that has specialized care and self-management in Geriatrics and Gerontology in the city of Rio de Janeiro, therefore, it consists of a closed universe of clients.
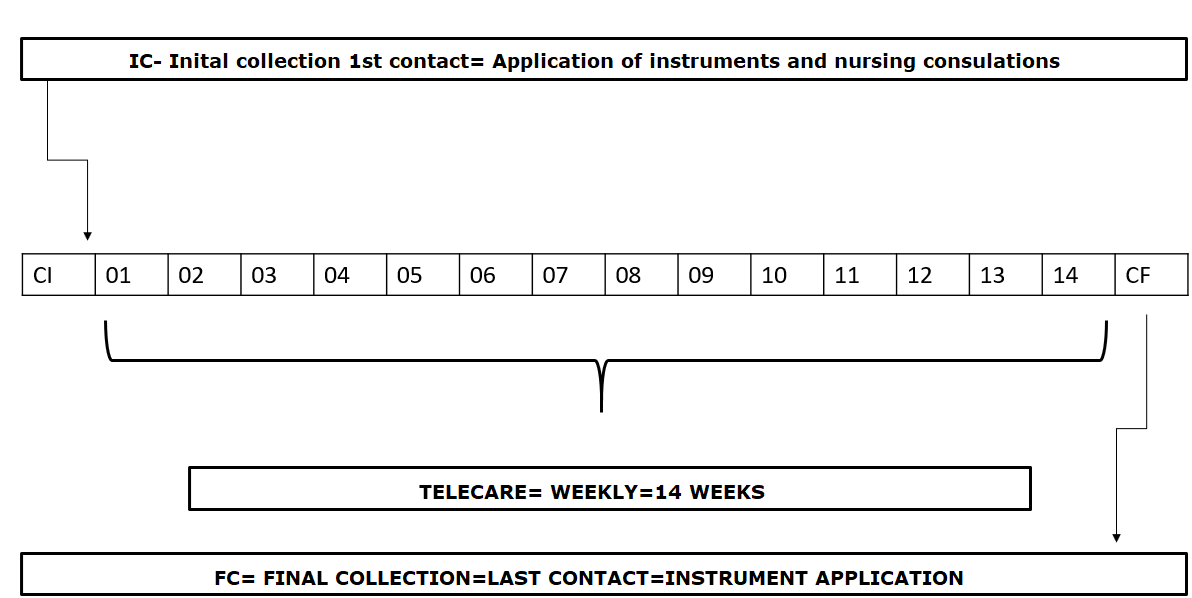
The research participants were divided into two groups as about 50% of the caregivers were elderly people who did not know how to use the video call application or did not have a smartphone and only had a landline, therefore they received calls exclusively in a conventional manner; and the group by Video Call through the WHATSAPP® application. After the division, the Telecare intervention was monitored and the before and after assessment of the elderly with dementia and their caregiver was performed. It should be noted that the same intervention and the same protocol were used for both groups, only the form of call was changed. The data collection period was from December 2018 to March 2019. The research was designed according to figure 01.
Figure 1 - Outline of the research. Niterói, Rio de Janeiro, 2019
Source: Author
The follow-up to identify maintenance and/or change in the functional capacity of the elderly with dementia and caregiver burden occurred before the intervention during hospitalization, and then at the elderly's home by a trained nurse specialist in gerontology, and not the same one who performed the intervention. With regard to follow-up by tele-care, this was performed through an instrument that contained questions about the caregiver, the elderly with dementia, the family, in addition to guidelines regarding home care obtained according to a systematic literature review (6). The Telecare instrument focused on: the care routine; relationship between the main caregiver and the elderly with dementia; alterations caused by the evolution of the disease. At the end of each call, a moment was allowed for comments and to clear up any last doubts.
Calls were made from 8 am to 6 pm, always on Wednesdays and Fridays or Tuesdays and Thursdays. At the end of the call, the researcher scheduled the next call on the participant's preferred day and time.
The expected outcome of the study consisted of reducing caregiver burden, decreasing neuropsychiatric symptoms by the elderly, and maintaining the functional capacity of the elderly with dementia assessed using the tests previously mentioned.
With regard to sociodemographic and clinical variables, the following stand out: - Age: self-declared from the date of birth (day/month/year), expressed in full years; -Sex: self-declared and categorized into: female and male; -Civil status: self-declared and categorized into: single; married; widower; separated/divorced; -Education level: self-declared and categorized as illiterate, incomplete elementary, complete elementary, incomplete high school, complete high school, incomplete higher and complete higher; - Income: self-declared and categorized as: worker with a formal contract; autonomous; student; home; retired; pensioner; unemployed and another; -Chronic diseases: self-declared: Diabetes Mellitus, Hypertension.
Regarding the variables related to monitoring by telephone, the duration of telephone calls is emphasized, considering the time in minutes of calls, and marking the time started and the time ended.
From the data collection, two databases were built and analyzed using the SPSS program (Statistical Package for the Social Science), version 22.0 and the Microsoft Excel 2013 application.
Database 01 contains data covering socio-demographic variables, variables from the first assessment and variables observed in subsequent assessments. Database 02 contains data only from the connections based on the protocol to the experiment group in the period of analysis, together with the socio-demographic and subsequent variables of these patients.
The descriptive analysis of the data aimed to present the characteristics of the patients, their caregivers and the intervention; it was performed based on the construction of graphs, frequency distributions and calculation of descriptive statistics (proportions of interest and calculation of minimum, maximum, average, median, standard deviation, coefficient of variation - CV for quantitative variables). The variability in the distribution of a quantitative variable was considered low if CV <0.20, moderate if 0.20 ≤ CV <0.40, and high if CV ≥ 0.40.
The inferential analysis aimed to assess the statistical significance of the observed differences. In order to verify a significant association between two qualitative variables, the objective was to use the Chi-Square Test or the Fisher's Exact Test when the Chi-Square Test is inconclusive and it is possible. In the Inferential Analysis of a quantitative variable, the comparison of the distribution of the quantitative variable between two independent groups was performed using the Mann-Whitney non-parametric test, due to the small sizes of the subgroups.
All discussions were held at the maximum significance level of 5% (0.05), i.e., the following decision rule was adopted in the statistical significance tests: rejection of the null hypothesis whenever the p-value associated with the test was lower than 0.05.
RESULT
There was a total of 660 participants approached to participate in the study. From this general amount, 450 participants were subtracted who had a MMSE result greater than 26 and 190 participants who did not meet the inclusion criteria: 20 refused to participate in the research; 13 presented complications during hospitalization, prolonging hospitalization for more than 60 days; 100 were ILPI residents or Homecare; 45 had advanced cancer with metastasis or were in palliative care; 07 subjects were being readmitted and 05 died.
Thus, there was a sample of 20 participants to follow up tele-care, 10 in the tele-care group by telephone call and 10 in the video-call group via the WHATSAPP® application, allocated according to demand. It should be noted that there was no loss of follow-up.
To verify the existence of homogeneity in the sample, the characteristic profile of elderly people with dementia was drawn up (Table 1). It was found that the participants have the same training characteristics, i.e., the same basic initial conditions. Such finding is important so that the tele-care treatment applied is the main factor that differentiates the group before and after the intervention. And, thus the observed effects can be attributed to the maximum to the tele-care.
Table 1: Patient characteristics. Niterói, Rio de Janeiro, 2019.
|
Overall n=20 |
p-value |
|||
|
n |
% |
|||
|
Age (years) |
|
|
|
|
|
70 |¾ 75 |
2 |
10 |
0.765(a) |
|
|
75 |¾ 80 |
1 |
5 |
|
|
|
80 |¾ 85 |
10 |
50 |
|
|
|
85 |¾ 90 |
3 |
15 |
|
|
|
90 |¾ 95 |
3 |
15 |
|
|
|
95 |¾ 100 |
1 |
5 |
|
|
|
Sex |
|
|
|
|
|
Female |
08 |
40 |
0.679(a) |
|
|
Male |
12 |
60 |
|
|
|
Family income |
|
|
|
|
|
1 |¾4 |
05 |
25 |
0.796(a) |
|
|
4 |¾8 |
12 |
60 |
|
|
|
8 |¾10 |
03 |
15 |
|
|
|
Length of Hospitalization (days) |
|
|
|
|
|
5 |¾20 |
13 |
65 |
0.567(a) |
|
|
20 |¾ 35 |
3 |
15 |
|
|
|
35 |¾ 50 |
2 |
10 |
|
|
|
50 |¾ 65 |
2 |
10 |
|
|
|
Schooling |
|
|
|
|
|
Complete high school |
20 |
100 |
1.000(b) |
|
|
MEEM |
|
|
|
|
|
0 |¾ 10 |
14 |
70 |
|
|
|
10 |¾ 20 |
4 |
20 |
|
|
|
20 |¾ 30 |
2 |
10 |
|
|
|
Relationship with caregiver |
|
|
|
|
|
Caregiver |
|
|
|
|
|
Family member |
11 |
55 |
Non-conclusive chi-square test |
|
|
Professional |
6 |
30 |
||
|
Both |
3 |
15 |
||
|
Hospitalization diagnoses |
|
|
|
|
|
UTI |
7 |
35 |
0.194(b) |
|
|
Pneumonia |
5 |
25 |
0.179(b) |
|
|
Advanced palliative care |
3 |
15 |
0.345(b) |
|
|
Heart failure |
2 |
10 |
0.150(b) |
|
|
Falls |
1 |
5 |
1.000(b) |
|
|
Dehydration |
1 |
5 |
1.000(b) |
|
|
Reduction in level of conciousness |
1 |
5 |
0.400(b) |
|
a) Mann-Whitney test (b) Fisher's exact test Source: Author
Table 2 shows the frequency distribution of the caregivers' characteristics. When significance tests were performed comparing the distributions of the factors listed in Table 02 in the male and female groups, the resulting p-values, almost all greater than 5%, show that there are no significant associations between the distributions of the caregivers' characteristics and the sex of the patients. The exception is for the statement of everyday life that is significantly more cited when the patient is female (37%), p-value = 0.045 of Fisher's exact test.
Table 2: Characteristics of caregivers. Niterói, Rio de Janeiro, 2019
|
Factor |
Overall n=20 |
Female patient n=8 |
Male patient n=12 |
p-value of Fisher's exact test comparing the distributions of the variable in the male and female groups |
||||
|
n |
% |
n |
% |
n |
% |
|
||
|
Daily |
|
|
|
|
|
|
|
|
|
Quiet |
10 |
50 |
3 |
37 |
7 |
58 |
0.650 |
|
|
Tiring |
2 |
10 |
2 |
25 |
0 |
00 |
0.147 |
|
|
Busy |
3 |
15 |
3 |
37 |
0 |
00 |
0.045 |
|
|
Planned
Varies according to the state of the elderly |
8 |
40 |
2 |
25 |
6 |
50 |
0.373 |
|
|
|
6 |
30 |
2 |
25 |
4 |
33 |
1.000 |
|
|
How the caregiver feels |
|
|
|
|
|
|
|
|
|
Anxious |
7 |
35 |
3 |
37 |
4 |
33 |
1.000 |
|
|
Tired |
12 |
60 |
6 |
75 |
6 |
50 |
0.373 |
|
|
Calm |
1 |
05 |
0 |
00 |
1 |
08 |
1.000 |
|
|
Stressed |
2 |
10 |
1 |
12 |
1 |
08 |
1.000 0.619 |
|
|
Exhausted |
4 |
20 |
1 |
12 |
3 |
25 |
||
|
Sleep pattern |
|
|
|
|
|
|
|
|
|
Insomnia |
3 |
15 |
2 |
25 |
1 |
08 |
0.537 |
|
|
Sleeps less than 8 hours |
14 |
70 |
5 |
62 |
9 |
75 |
0.642 |
|
|
Sleeps more than 8 hours |
4 |
20 |
1 |
12 |
3 |
25 |
0.619 |
|
|
Leisure activities |
|
|
|
|
|
|
|
|
|
Go out with friends/ family |
6 |
30 |
1 |
12 |
5 |
42 |
0.325 |
|
|
Travel |
6 |
30 |
2 |
25 |
4 |
33 |
1.000 |
|
|
Attend church |
3 |
15 |
2 |
25 |
1 |
08 |
0.537 |
|
|
Others |
8 |
40 |
2 |
25 |
6 |
50 |
0.373 |
|
|
Diet |
|
|
|
|
|
|
|
|
|
Reduced |
1 |
05 |
1 |
12 |
0 |
00 |
0.400 |
|
|
Increased |
1 |
05 |
1 |
12 |
0 |
00 |
0.400 |
|
|
Medication use |
2 |
10 |
2 |
20 |
0 |
00 |
0.147 |
|
|
Perception of well-being |
12 |
60 |
6 |
75 |
6 |
50 |
0.373 |
|
|
Coping perception |
11 |
55 |
4 |
50 |
7 |
58 |
1.000 |
|
|
Perception of worsening health status of the caregiver |
16 |
80 |
7 |
87 |
9 |
75 |
0.619 |
|
|
Perception of worsening health status of the elderly |
4 |
20 |
1 |
12 |
3 |
25 |
0.619 |
|
|
Knowledge about the disease |
20 |
100 |
8 |
100 |
12 |
100 |
1.000 |
|
|
Difficulty in assisting the elderly |
20 |
100 |
8 |
100 |
12 |
100 |
1.000 |
|
|
Keeps conversation with the elderly |
17 |
85 |
7 |
87 |
10 |
83 |
1.000 |
|
|
Fear of performing care |
8 |
40 |
3 |
37 |
5 |
42 |
1.000 |
|
|
Apprehension about the health status of the elderly |
18 |
90 |
7 |
87 |
11 |
92 |
1.000 |
|
|
Fear of institutionalization |
2 |
10 |
1 |
12 |
1 |
08 |
1.000 |
|
|
Receives help from others |
10 |
50 |
2 |
25 |
8 |
67 |
0.170 |
|
|
Modified the environment for the elderly |
8 |
40 |
3 |
37 |
5 |
42 |
||
Source: Author
The elderly and their caregivers were followed up for up to 14 calls, made every 7 days. Therefore, the follow-up time was up to 98 days. The first 4 calls are the longest, varying from 40 to 70 minutes, with a median duration of 51 minutes, an average of 52.9 minutes and a standard deviation of 2.1 minutes, which represents low variability in the duration of these calls (CV = 0.15). From the fifth call, the duration of the call tends to decrease, to the point that in the fourteenth calls, the calls vary from 20 to 40 minutes, with a median duration of 25 minutes, an average of 27.5 minutes and a standard deviation of 5.5 minutes, which represents moderate variability in the duration of these connections (CV = 0.20). Chart 1 shows the interventions carried out in tele-care.
Chart 01 - Interventions performed during tele-care. Niterói, Rio de Janeiro, 2019.
|
Performed interventions |
|
Intervention 1 - Encourage the caregiver to speak the whys of the answers Intervention 2 - Chat to demonstrate understanding of the caregiver's motives Intervention 3 - Guidance on ways to improve the care routine Intervention 4 - Determine safety risk for the elderly and caregiver Intervention 5 - Encourage the caregiver to vent their feelings properly and safely Intervention 6 - Assist in identifying preferred activities Intervention 7 - Assist in prioritizing activities to accommodate energy levels Intervention 8 - Guide the caregiver to maintain a normal sleep cycle Intervention 9 - Indicate relaxation techniques and caffeine reduction Intervention 10 - Guide on the importance of sleep Intervention 11 - Encourage leisure activities Intervention 12 - Guide on the importance of leisure activities Intervention 13 - Encourage the caregiver to optimize his time for care so that he can allocate time for himself Intervention 14 - Encourage caregivers to take care of their health Intervention 15 - Demonstrate the importance of being healthy Intervention 16 - Guidance on the need for a balanced diet Intervention 17 - Explain the proper use of medications prescribed by the doctor Intervention 18 - Encourage consultations for health monitoring Intervention 19 - Explain the severity of the use of non-pharmacological drugs Intervention 20 - Clarify the existence of aid groups Intervention 21 - Maintain the usual food, giving preference to light food Intervention 22 - Guide on the importance of a good diet, fluid intake and exercise during the day Intervention 23- Assist in the development of realistic expectations about care Intervention 24 - Assist in identifying activities of precipitating aspects that may or may not be changed Intervention 25 - Check the need for adaptation devices for personal hygiene, dressing, grooming, using the toilet and eating Intervention 26 - Encourage the elderly to perform normal activities of daily living according to their ability Intervention 27- Encourage the caregiver to encourage the elderly's independence and intervene only when necessary Intervention 28 - Identify the type and degree of cognitive impairment using a standardized instrument Intervention 29 - Teaching caregivers medical and nursing plans for care Intervention 30 - Determine the behavioral expectations of the elderly's cognitive status Intervention 31 - Assess the caregiver's level of knowledge Intervention 32 - Guidance on the pathology Intervention 33 - Clarify doubts according to demand Intervention 34 - Evaluate and ensure the best possible care Intervention 35 - Assess the emotional and family reaction of the elderly's condition Intervention 36 - Encourage interaction between family, caregiver and elderly Intervention 37 - Check if the elderly person shows signs of emotional abuse Intervention 38 - Identify caregivers who have impaired physical and / or mental health Intervention 39 - Encourage the search for an LTCF Intervention 40- Advise on the expected health problems of the elderly Intervention 41 - Assess the possibility of alternating care Intervention 42 - Encourage the caregiver's dialogue with family members regarding care Intervention 43 - Advise on adequate conditions for the elderly to live Intervention 44 - Guidance on the risks of falling |
Source: Author
Table 3 shows the frequency distribution of each intervention shown in Table 1 for each call day and overall. From the overall frequencies, it is observed that in the 14 calls and in more than 90% of the calls, the interventions most frequently performed were : Evaluate and ensure the best possible care; Encourage the caregiver's dialogue with family members regarding care; Assist in identifying activities of precipitating aspects that may or may not be changed; Talk in order to demonstrate understanding of the caregiver's motives; Guide on the importance of leisure activities; Encourage caregivers to take care of their health; Encourage the consultation of health monitoring periodicals; Advise on not performing self-medication; Encourage interaction between family, caregiver and elderly; Assist in identifying preferred activities; Determine security risk for the elderly and care; Guide on the importance of sleep and, Guide on the need for a balanced diet;
Table 3: Frequency of interventions treated at each call. Niterói, Rio de Janeiro, 2019
|
Intervention |
Call 1 % |
Call 2% |
Call
3% |
Call 4% |
Call 5% |
Call 6% |
Call 7% |
Call 8% |
Call 9% |
Call
10% |
Call 11% |
Call 12% |
Call 13% |
Call 14% |
Overall% |
|
Intervention 1 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
45 |
40 |
81.1 |
|
Intervention 2 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
45 |
40 |
91.8 |
|
Intervention 3 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 4 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
40 |
30 |
90.7 |
|
Intervention 5 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 6 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
45 |
30 |
91. |
|
Intervention 7 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
50 |
50 |
50 |
40 |
30 |
31.8 |
|
Intervention 8 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
25 |
20 |
30 |
25 |
|
Intervention 9 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
45 |
30 |
80.4 |
|
Intervention 10 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
40 |
30 |
90.7 |
|
Intervention 11 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
45 |
30 |
80.4 |
|
Intervention 12 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
30 |
91.4 |
|
Intervention 13 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
45 |
30 |
80.4 |
|
Intervention 14 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
30 |
91.4 |
|
Intervention 15 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 16 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
30 |
30 |
90 |
|
Intervention 17 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 18 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
30 |
91.4 |
|
Intervention 19 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
45 |
45 |
50 |
50 |
50 |
50 |
30 |
72.9 |
|
Intervention 20 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
30 |
91.4 |
|
Intervention 21 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 22 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
45 |
45 |
100 |
100 |
100 |
80 |
30 |
85.7 |
|
Intervention 23 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 24 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
65 |
30 |
92.5 |
|
Intervention 25 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 26 |
95 |
95 |
95 |
95 |
95 |
95 |
95 |
95 |
95 |
95 |
95 |
95 |
50 |
30 |
87.1 |
|
Intervention 27 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 28 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
- |
- |
100 |
100 |
100 |
100 |
30 |
80.7 |
|
Intervention 29 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 30 |
85 |
85 |
85 |
85 |
85 |
85 |
85 |
85 |
85 |
85 |
85 |
85 |
85 |
30 |
81.1 |
|
Intervention 31 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 32 |
95 |
95 |
95 |
95 |
75 |
75 |
75 |
40 |
40 |
95 |
95 |
95 |
50 |
30 |
75.0 |
|
Intervention 33 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 34 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
30 |
95 |
|
Intervention 35 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 36 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
30 |
91.4 |
|
Intervention 37 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 38 |
90 |
90 |
90 |
90 |
100 |
100 |
100 |
100 |
100 |
90 |
90 |
90 |
90 |
30 |
89.3 |
|
Intervention 39 |
100 |
100 |
100 |
100 |
65 |
65 |
65 |
65 |
65 |
50 |
50 |
50 |
50 |
30 |
68.2 |
|
Intervention 40 |
80 |
80 |
80 |
80 |
80 |
80 |
80 |
80 |
80 |
80 |
80 |
80 |
80 |
30 |
76.4 |
|
Intervention 41 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
50 |
50 |
50 |
50 |
30 |
80.7 |
|
Intervention 42 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
30 |
95 |
|
Intervention 43 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
70 |
70 |
50 |
50 |
50 |
50 |
30 |
76.4 |
|
Intervention 44 |
100 |
100 |
100 |
100 |
100 |
100 |
100 |
70 |
70 |
50 |
50 |
50 |
50 |
30 |
76.4 |
Source: Author
The ZARIT before and after the intervention showed that for 35% of the patients (cells in bold) there was no change in the ZARIT scale before and after the intervention. For 65% of patients, the ZARIT score decreased by 1 classification. In the overall analysis, the change in ZARIT was statistically significant, through the Wilcoxon test. It is concluded that after the intervention, caregivers showed a significant reduction in the ZARIT score.
As for the NPI-intensity before and after intervention, it was evident that for 100% of the patients (cells in bold) there was no change in the intensity of the NPI before and after the intervention, and shows the joint frequency distribution of the NPI- Distress before and after the intervention. intervention. For 50% of the patients (cells in bold) there was no change in the NPI-Distress scale before and after intervention, for the remaining 50% there was a reduction of 1 classification in the NPI Distress classification. In the overall analysis, the change in NPI- Distress was statistically significant through the Wilcoxon test. It is concluded that after the intervention, the patients presented a significant reduction in the NPI-Distress classification.
Table 04 shows the joint frequency distribution of the applied tests for the PRISMA - 7, KATZ, NPI AND ZARIT. The Prisma7 pre and post intervention. For 50% of the patients (in bold), there was no change in the Prisma7 scale before and after the intervention. For the remaining 50% of patients, there was an increase of 1 point in the Prisma score7. In the overall analysis, the change in Prisma7 was statistically significant from the Wilcoxon test. It is concluded that after the intervention, patients showed a significant increase in the Prisma score7.
The KATZ pre and post intervention presents 70% of the patients (cells in bold) there was no change in the KATZ scale pre and post intervention. The Katz score decreased for 25% of patients and increased for 5%. In global analysis, the change in KATZ was not statistically significant in the Wilcoxon test.
Table 4: Evolution of the Prisma7, Zarit, NPI-D and Katz scales before and after the intervention. Niterói, Rio de Janeiro, 2019
|
KATZ pre- intervention |
Katz post-intervention |
TOTAL
n % |
P – value ( Wilcoxon test) |
|||||
|
0 n % |
1 n % |
2 n % |
3 n % |
4 n % |
5 n % |
|
p-value=0.102 |
|
|
0 n % |
02 10 |
00 00 |
00 00 |
00 00 |
00 00 |
00 00 |
02 10 |
|
|
1 n % |
00 00 |
04 20 |
01 05 |
00 00 |
00 00 |
00 00 |
05 25 |
|
|
2 n % |
00 00 |
00 00% |
04 20 |
00 00 |
00 00 |
00 00 |
04 20 |
|
|
3 n % |
00 00 |
00 00% |
1 05 |
02 10 |
00 00 |
00 00 |
03 15 |
|
|
4 n % |
00 00 |
00 00% |
0 00 |
4 20 |
01 05 |
00 00 |
05 25 |
|
|
5 n % |
00 00 |
00 00 |
00 00 |
00 00 |
00 00 |
01 05 |
01 05 |
|
|
Total n % |
02 02 |
04 00 |
06 00 |
06 00 |
01 00 |
01 00 |
20 02 |
|
|
NPI Distress pre intervention |
NPI Post-intervention distress |
Total n % |
P – value ( Wilcoxon test) |
|||||
|
0 Absent n % |
1 Minimum % |
2 Mild n % |
3 Moderate n % |
4 Moderate to intense n % |
p-value=0.002 |
|||
|
0 Absent n % |
10 50 |
00 00 |
00 00 |
00 00 |
10 50 |
02 10 |
||
|
1 Minimum n % |
04 20 |
00 00 |
00 00 |
00 00 |
04 20 |
05 25 |
||
|
2 Mild n % |
00 00 |
03 15 |
00 00 |
00 00 |
00 00 |
04 20 |
||
|
3 Moderate % |
00 00 |
00 00 |
02 10 |
00 00 |
00 00 |
03 15 |
||
|
4 Moderate to Intense n % |
00 00 |
00 00 |
00 00 |
01 05 |
00 00 |
05 25 |
||
|
Total n % |
14 70 |
03 15 |
02 10 |
01 05 |
14 70 |
01 05 |
||
|
Prisma 7 pre intervention |
Prisma 7 post-intervention |
Total n % |
P – value ( Wilcoxon test) |
|||||
|
4 n % |
5 n % |
6 n % |
||||||
|
4 n % |
01 05 |
00 00 |
00 00 |
01 50 |
p-value=0,002 |
|||
|
5 n % |
08 40 |
06 30 |
00 00 |
14 70 |
||||
|
6 n % |
00 00 |
02 10 |
03 15 |
05 25 |
||||
|
Total n % |
09 45 |
08 40 |
03 15 |
20 100 |
||||
|
Zarit pre intervention |
Zarit post-intervention |
Total n % |
P – value ( Wilcoxon test) |
|||||
|
0 Without Burden n %
|
1 Moderate burden n % |
2 Moderate to Severe burden n % |
||||||
|
0 Absent n % |
02 10 |
00 00 |
00 00 |
02 10 |
p-value < 0,001 |
|||
|
1 Moderate burden n % |
04 20 |
02 10 |
00 00 |
06 30 |
||||
|
2 Moderate to severe burden n % |
00 00 |
05 25 |
03 15 |
08 40 |
||||
|
3 Severe budren n % |
00 00 |
00 00 |
04 20 |
04 20 |
||||
Fonte: Autor
DISCUSSION
In the present study, the profile of participants is similar to that reported in the literature, in which the majority of caregivers are women (11); these women who care for men are more likely to accept changes and innovations in care interventions (12).
In this context, it is emphasized that care for the elderly with dementia, in plurality, is carried out by family members - informal caregivers - who are available to provide the care that the elderly needs. The role of caregivers was mainly exercised by women, wives, daughters, married, elderly or middle age and the prevalence of family and primary caregivers, demonstrating a greater bond with the elderly (11) because, culturally, they coordinate, care and they organize the family, and thus it is also up to them to care for the elderly family member, if necessary (13).
As they are mostly women who play the role of caregiver, burden is reported due to performing other domestic activities. This subjective burden of women caregivers was greater when patients had another comorbidity. In addition, the greater the number of problematic behaviors of the patient (evidenced by the NPI), the greater the family member's burden.
In addition, the presence of comorbidity was a factor associated with subjective burden, possibly because it represents a greater severity of the patient's clinical condition, since the severity of the patient's clinical condition is also associated with a greater degree of subjective burden (13).
It was observed that women spent more time to care for the patient than men (14). The fact that the patient does not perform an activity outside the home can increase the amount of time spent by caregivers in caring for the patient in everyday life, increasing the burden on women caregivers.
The time spent on caring for the elderly was over 12 months, with the predominant rate of this survey of caregivers offering care over 10 years (15). It is believed that the variable time to care is important if a relationship is established between the person being cared for and the person who cares.
The average age of elderly people with dementia was 84.5 years. The minority of the elderly in this study was partially dependent for Activities of Daily Living. The elderly with total dependency were older than those with partial dependence. The elderly women were more dependent when compared to the elderly men. Singles and widowers were more dependent than married, divorced and separated.
The advanced age added to the level of dependence of this elderly person with dementia becomes one of the main factors to characterize this elderly person as being a frail elderly person and thus increase the length of hospitalization. The frail elderly had a higher average number of days in hospital compared to non-frail ones, with time equal to or greater than ten days, which corroborates the finding in this survey of a mean hospitalization of 25 days (16).
Another factor that also contributes to characterizing the elderly with dementia as fragile is the level of readmissions, also evidenced in this research with almost 30% of readmissions. The readmission rates of frail elderly people are high when compared to non-frail elderly people; that is why the association of fragility variables are important and should be investigated, with Prisma7 as a good screening tool for this (16).
PRISMA-7 is the instrument used in the Program on Research for Integrating Services for the Maintenance of Autonomy (PRISMA Project), in Canada, to identify elderly people with functional dependence. It consists of the application of a quick questionnaire consisting of seven questions. The elderly are considered fragile when they have three or more positive responses, with sensitivity and specificity of 78.3% and 74.7%, respectively (17). The data indicate a majority of frail elderly in this sample, therefore, it was not expected to change this test, only its characterization and monitoring.
Similar to the Katz Index Prism, which assesses the elderly person's ability to perform activities of daily living, despite the statistical results without significance, one can infer clinical significance to the results since 70% of patients (cells in bold) did not show changes in the Katz Index, that is, they maintained their functional capacity. This result for elderly patients after hospital discharge with dementia and multimorbidity is clinically relevant.
Based on the analysis of the results obtained with the Zarit Burden Inventory, there was a statistically significant decrease in the burden scores. Thus, an intervention study was also performed, where he also noticed a significant decrease in perceptions of burden (18). Two differences between the study in question and that of Ferreira and Barham is the intervention time, which in this study was 14 weeks, and that of Ferreira and Barham, was 08 weeks. The intervention program that Ferreira and Barham used was face-to-face and, in this research, it is performed by remote technology with the use of telephone and video calling through the WHATSAPP®s application.
By comparing the responses of caregivers in the pre-test and in the post-test, there was a reduction in the difficulties they reported in relation to dealing with the elderly with dementia. The answers show that the caregivers modified some of their behaviors when dealing with difficult situations of the demented elderly, especially in the daily care, medication and challenging behavior. Therefore, using the NPI was a useful tool for the assessment of behavioral changes in several situations, related to very frequent neuropsychiatric changes in dementia at all stages of severity, such as behavioral changes, neurodegenerative issues and questions about the distress of the caregiver of each of the evaluated behaviors (19).
The study in question allowed the identification of behavioral changes, and making possible an accurate performance for each elderly and caregiver through the interventions. In order to recognize how and how much each of the changes can affect both, intervening individually in each case, causing a significant reduction in the emotional distress of the caregiver at the end of the research. In other words, there was an emotional improvement in the caregiver or a greater understanding of the changes caused by dementia (20) it is stated that by training health professionals to manage the neuropsychiatric symptoms presented by the elderly with the use of specific interventions, they reduce the distress of the caregiver favoring the improvement of the quality of life of both.
CONCLUSION
However, the data from this study demonstrated that Tele-care reduced the burden and distress of caregivers, and the maintenance of activities of daily living for the elderly. It confirms that nurses should associate their clinical knowledge with gerontological principles, providing person-centered care considering the functional capacity of elderly individuals as a care goal as well as planning discharge with education and preparation of family/caregivers for home care. In the data of this study, it is emphasized that post-hospital discharge care can continue in transitional care centers, in the outpatient clinic, at the client's home in association with the use of remote technologies. Thus, tele-care may be an increasing form of communication in the post-discharge nursing care to guarantee and improve access to health care.
REFERENCES
1. Silva AR, Sgnaolin V, Nogueira EL, Loureiro F, Engroff P, Gomes I. Doenças crônicas não transmissíveis e fatores sociodemográficos associados a sintomas de depressão em idosos. J Bras Psiquiatr [Internet]. 2017 [cited 2019 set 25]; 66(1): 45-51. Available from: https://www.scielo.br/scielo.php?pid=S0047-20852017000100045&script=sci_arttext
2; Lino VtS, Rodrigues NCP, Camacho LAB, O’Dwyer G, Lima IS, Andrade MKN, et al. Prevalence of overburden in caregivers of dependent elderly and associated factors in a poor area of Rio de Janeiro, Brazil. Cad Saude Publica [Internet]. 2016 [cited 2019 set 25]; 32(6). Available from: https://www.scielo.br/scielo.php?pid=S0102-311X2016000605001&script=sci_arttext
3. Abreu WC. Cuidados paliativos para utentes com demência avançada: Reflexões sobre a sua implementação. Rev Portu Enferm Saúde Mental [Internet]. 2016 [cited 2019 set 30]; (6): 6-10. Available from:http://www.scielo.mec.pt/scielo.php?script=sci_arttext&pid=S1647-21602016000300001
4. Nunes, D. P., Brito, T. R. P. D., Duarte, Y. A. D. O., & Lebrão, M. L. (2019). Cuidadores de idosos e tensão excessiva associada ao cuidado: evidências do Estudo SABE. Rev Bras Epidemiol [Internet] 2019 [cited 2019 set 30]; 21 (Suppl02): 1-14. Available from: https://www.scielosp.org/article/rbepid/2018.v21suppl2/e180020/
5. Labegalin CMG, Nogueira IS, Moretti AZP, Carreira L, Baldissera VDA. Demandas educativas de cuidadores familiares de idosos dependentes. Rev Enferm Cent O Min [Internet]. 2016 [cited 2019 set 30];1(6): 1994-2008. Available from:http://www.seer.ufsj.edu.br/index.php/recom/article/view/1129/1008
6. Santana RF, Dantas RV, Soares TS, Delphino TM, Hercules ABS, Leite Junior HMT. Telecare to elderly people with alzheimer and their caregivers: sistematic review. Cienc Cuid Saude [Internet]. 2018 [cited 2019 out 20];17(4): 1-6.Available from: http://www.periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/41653/751375138716
7. Michel T, Lenardt MH, Willig MH, Alvarez AM. Do real ao ideal-o (des) cuidar da saúde dos idosos longevos. Rev Bras Enferm [Internet]. 2015 [cited 2019 out 20]; 68(3): 343-9. Available from:https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672015000300398
8. Nascimento BO, Souza NVDO, Santos DM, Silva PADS. Telemonitoramento em enfermagem para clientes em situação de estomaterapia: experiência inovadora para o processo ensino-aprendizagem. Inter: pensando exten [Internet]. 2018 [cited 2019 out 20]; 1(26): 73-78.
9. Gitlin LN, Winter L, Dennis MP, Hodgson N, Hauck WW. Targeting and managing behavioral symptoms in individuals with dementia: a randomized trial of a nonpharmacological intervention. J Americ Geriatr Society [Internet]. 2010 [cited 2019 out 20]; 58(8): 1465-1474. Available from:https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1532-5415.2010.02971.x
10. Matthews JT, Lingler JH, Campbel GB, Hunsaker AE, Hu L, Pires BR, et al. Usability of a wearable camera system for dementia family caregivers. J Healthcare engineering [Internet]. 2015 [cited 2019 out 20]; 6(2): 213-238. Available from:https://www.hindawi.com/journals/jhe/2015/120149/
11. Figueiredo K, Coelho FGM, Corazza DI, Pádua AM, Ferreira BN, Papini CB. Efeito de intervenção de exercícios físicos multifuncionais na percepção da qualidade de vida de cuidadores de pacientes com Doença de Alzheimer. Rev bras Qual Vida [Internet]. 2018 [cited 2019 out 20];10(2):1-15. Available from:https://periodicos.utfpr.edu.br/rbqv/article/viewFile/7651/5181
12. Quaresma MLB, Ribeirinho C. Envelhecimento–Desafios do Séc. XXI. Rev Kairós: Gerontol [Internet]. 2016 [cited 2019 out 15];19(3):29-49. Available from:https://revistas.pucsp.br/index.php/kairos/article/view/30900
13. Pizolotto ALZ, Leite MTL, Hildebrandt LM, Costa MC, Resta DG. Organização da família no cuidado ao idoso com doença de Alzheimer. Espaç Saúde [Internet]. 2015 [cited 2019 nov 2];16(4):41-53. Available from:https://pesquisa.bvsalud.org/portal/resource/pt/biblio-834519
14. Sharma N, Chakrabarti S, Grover S. Gender differences in caregiving among family-caregivers of people with mental illnesses. World J Psychi [Internet]. 2016 [cited 2019 nov 2]; 6(1),7. Available from: https://www.researchgate.net/publication/298428873_Gender_differences_in_caregiving_among_family_-_caregivers_of_people_with_mental_illnesses
15. Jacob CS, Beuter M, Girardon-Perlini, Schwartz E, Leite MT, Roso CC. A dinâmica familiar frente ao idoso em tratamento pré-dialítico. Esc Anna Nery [Internet]. 2017 [cited 2019 nov 2]; 21(1). Available from:https://www.scielo.br/scielo.php?pid=S1414-81452017000100222&script=sci_abstract&tlng=pt
16. Freire JCG, Nóbrega IRAP, Dutra MC, Silva LM, Duarte HA. Fatores associados à fragilidade em idosos hospitalizados: uma revisão integrativa. Saúde Deb [Internet]. 2017 [cited 2019 nov 2];41(115): 1199-1211. Available from: https://www.scielo.br/scielo.php?pid=S0103-11042017000401199&script=sci_abstract&tlng=pt
17. Santos PHS, Fernandes MH, Casotti CA, Coqueiro RS, Carneiro JAO. Perfıl de fragilidade e fatores associados em idosos cadastrados em uma Unidade de Saúde da Família. Cien Saúde Coletiva [Internet]. 2015 [cited 2019 nov 2];20(6), 1917-1924.Available from: https://www.scielo.br/scielo.php?pid=S1413-81232015000601917&script=sci_abstract&tlng=pt
18. Ferreira CR, Barham EJ. Uma intervenção para reduzir a sobrecarga em cuidadores que assistem idosos com doença de Alzheimer. Rev Kairós: Gerontol [Internet]. 2016 [cited 2019 nov 2];19(4): 111-130. Available from:https://revistas.pucsp.br/kairos/article/view/31645
19. Terra NL, Crippa A, Nascimento NMR. Auxiliando o cuidador de idosos. [S.l.]: EDIPUCRS;2018.
20. Silva, B. M. C., Caldas, C. P., David, H. M. S. L., & Thiollent, M. J. M. (2018). Dificuldades encontradas no cuidado ao idoso com demência: enfrentamento baseado na pesquisa participativa. Rev Bras Geriatr Gerontol [Internet]. 2018 [cited 2019 nov 2];21(1): 35-43. Available from:https://www.scielo.br/scielo.php?script=sci_abstract&pid=S1809-98232018000100035&lng=pt&nrm=iso
Received: 02/17/2020
Revised:05/12/2020
Approved: 05/12/2020