Social pain, gender, and people with sickle cell disease: an exploratory study
Joseane Gomes Trindade da Silva1 , Evanilda Souza de Santana Carvalho2 , Aline Silva Gomes Xavier2, Michelle de Santana Xavier Ramos2, Heros Aureliano Antunes da Silva Maia1, Tania Maria de Araújo2
1 Universidade Estadual de Feira de Santana.
2 Universidade Federal Da Bahia.
ABSTRACT
Aim: Social pain, gender, and people with sickle cell disease: an exploratory study. Method: this is a qualitative and exploratory study and it was conducted in a Sickle Cell Disease Reference Center in a municipality in the interior of Bahia. The data obtained from theme-story drawings and interviews with 16 people were submitted to thematic content analysis. Results: two categories have emerged: “Social pain in women with sickle cell disease is expressed in the impossibility of being a housewife, mother and woman sexually” and “The social pain of men with sickle cell disease is expressed in the difficulty of being a worker, a provider and a sexually active man”. Discussion: the exclusion of work, changes in sexuality and parenting interfere in life projects and maintain the reproduction of gender stereotypes. Conclusion: sensitive listening in a multiprofessional care approach should be part of the therapeutic plan for people with sickle cell disease.
Descriptors: Gender Identity; Hemic and Lymphatic Diseases; Chronic Disease; Anemia, Sickle Cell.
INTRODUCTION
Social pain can be understood as painful sensations associated with the actual or potential damage of social ties, that is, those that derive from social rejection, social exclusion or loss(1). It happens when social relationships are threatened, damaged or lost, and is commonly described by metaphors or words used to refer to physical pain, such as “hurt feelings”, “broken bones” or “broken heart”, which help the interlocutor to understand the pain that is expressed(1,2). Unlike physical pain in which feelings are unlikely to be re-experienced after the painful episode is healed, the feelings arising from social pain can be revived even if the painful event happened long ago(2).
Social pain promotes the fear of isolation and abandonment, communication difficulties, besides economic losses, and loss of the social role played with family and friends(1,2). The need for acceptance is so fundamental that social exclusion has negative consequences for affection, health and well-being(2).
Among the chronic diseases characterized by social pain, one is sickle cell disease (SCD), the most prevalent chronic and hereditary disease in the world, due to a change in the hemoglobin molecule (Hb): the abnormal Hb S is produced in place of the normal Hb A. In Brazil, every year 3,500 children are born with SCD, predominantly in African descent individuals(5). It affects 0.1 to 0.3% of the black population, with a tendency to reach an increasingly significant share, due to the high degree of miscegenation in the country. In the State of Bahia the incidence of SCD is 1 for every 655 live births(3).
The occurrence of vaso-occlusions, especially in small vessels, represents the pathophysiological event that determines the majority of the signs and symptoms present in the clinical picture of patients with SCD, such as painful crises, lower limb ulcers, acute chest syndrome, splenic sequestration, stroke, retinopathy, chronic renal failure, and aseptic necrosis of the femoral(4).
Considering that the gender patterns are constituents of the social, it is possible to assume that the perspectives of feminine and masculine cross all the fields of human existence, imposing differences even in the field of sickness and care(5). In this sense, during the therapeutic listening in the consultation of people with SCD in a reference center, the following question emerged: how does social pain affect the gender roles of women and men with SCD? To answer this question, this study was developed with the objective of understanding the repercussions of social pain on the gender roles of women and men with SCD.
METHOD
A qualitative, exploratory study was developed. The participants were five women and 11 men, who met the following inclusion criteria: having a confirmed SCD diagnosis, being an adult aged equal or more than 18 years and less than or equal to 60 years, having experienced painful crises and being registered in the Reference Center of Attention to People with SCD, in a municipality in the interior of Bahia. Those who reported discomfort at the time of the interview were excluded in order to avoid bias in the research.
The number of participants was established by the theoretical saturation criterion, achieved after 16 interviews. Data collection was performed from March to May 2016. To ensure the anonymity of the participants, codes were used to represent them: the letter W to identify women, and M for men, followed by a number that determined the interview order.
Empirical data were obtained through the projective technique of the theme-story design and semi-structured interview. For the application of the projective technique, white A4 paper and colored pencils were made available and participants were asked to create a drawing from the following stimulus: “Draw something that represents a woman / man with pain and SCD”. After the drawing was completed, the participants were asked to elaborate a story, "look at your drawing and tell a story that has beginning, middle and end," and give it a title. The story was recorded and later transcribed by the first author.
Afterwards, the interviews were carried out through a semi-structured script that consisted of two parts: characterization of the participants and guiding questions about the experience of pain and the social roles of women and men with SCD.
All the interviews were carried out in a private room of consultation rooms, where only the participants and the interviewer were present; they lasted between 15 and 20 minutes; and were recorded and transcribed in their entirety by the interviewer herself.
The empirical material was submitted to thematic content analysis(6) and content analysis for story designs proposed by Coutinho(7) from data triangulation, obeying the following analysis scheme: (1) drawings observation and floating reading of interviews; (2) separation of the drawings by graphic similarity; (3) application of drawings analysis form for extracting explicit and implicit contents with construction of text synthesis (Figure 1); (4) Re-reading of statements, of the stories with their respective titles and of the synthesis texts with the codification of units of analysis (thematic unit); (5) categorization of themes and naming of categories; and (6) inference and data interpretation in the light of the literature on pain experience and on gender roles.
It should be noted that the categories were validated by the research team, authors of this article, consisting of two doctors (nurse and psychologist), two doctoral students in collective health (nurses), and two undergraduate students (nursing and medicine).
This study was approved by the Committee of Ethics in Research (CEP) of the State University of Feira de Santana (UEFS), under Opinion no. 1,254,708, and complied with the recommendations of Resolution 466/2012 of the National Health Council.
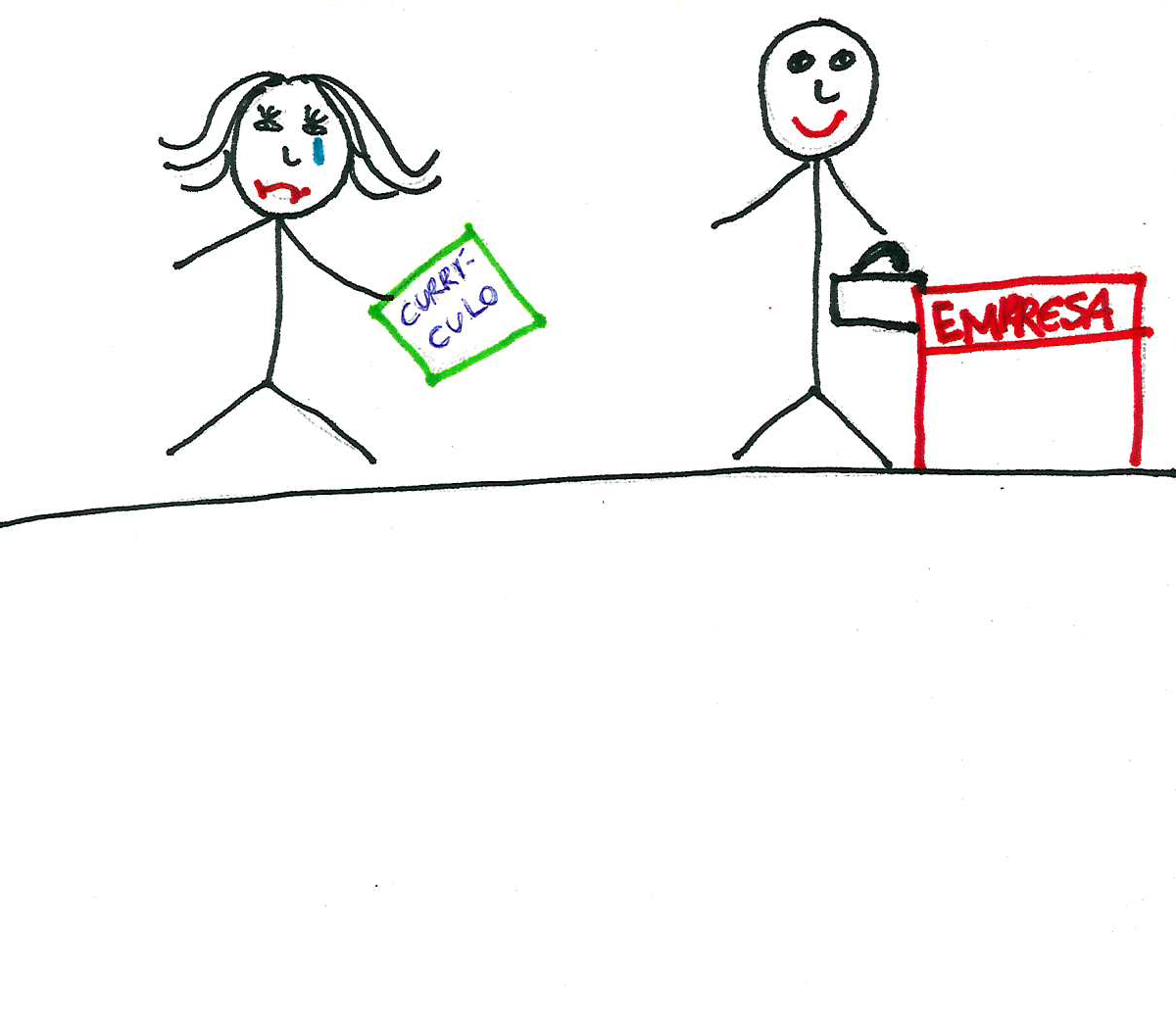
Figure 1. Model evaluation sheet of drawings. Bahia, 2016
|
DENOTATIVE CONTENT
(Explicit)
|
|
CONNOTATIVE CONTENT
(Implicit)
|
|
Woman
Tears
Woman's mouth tilted down
Curriculum in hand
Removal of bodies
Man with briefcase
Man's mouth tilted up
Table with business sign
|
A sad and tearful woman loses the opportunity to stay in the company where she delivered the resume.
Smiling man with folder in hand, near to the company sign
|
|
MENTAL MAP / MAKE THE SYNTHESIS:
Woman with sickle cell disease loses the job opportunity because she has the disease, that causes her to suffer; while the man represented is happy to have been given the opportunity to work. Thus, we can infer that having a formal job, that is, a job, promotes fulfillment and happiness, and disease is an obstacle to reach this ideal.
|
RESULTS
There were 16 people participating in this study, of whom five were women and 11 were men, all with HbSS hemoglobinopathy, aged between 18 and 52 years. Nine declared to be black. Only one participant had higher education. The occupations reported were merchant, homemaker, student and hairdresser. Eight were unemployed at the time of collection and only one received assistance from the National Institute of Social Security (INSS, acronym in Portuguese).
Among the participants, 15 reported having low income (≤1 minimum wage) and exclusive access to health services through the Unified Health System (SUS); only one participant at the higher level received four minimum salaries and, in addition to SUS services, provided private assistance services. The repercussions of social pain on the gender roles of women and men with SCD were organized into two categories that will be presented below.
Social pain in women with sickle cell disease is expressed in the impossibility of being a housewife, mother and sexed woman
Gender relations imprint different marks and roles to be socially fulfilled by women and men. For women with SCD, the significance of having the disease added to the experience of frequent seizures directly compromises domestic activities, leading to poor performance and frustration.
Often simply getting out of bed and doing daily activities, such as sweeping a house, washing the dishes, washing clothes, and making some meal, gets in the way [...] (W4).
It prevents taking care of children, taking care of the husband... (W5).
In general, women have concerns about difficulties in exercising their maternal roles and home and partner care. In addition to the low performance in domestic activities, due to the low level of education, the women interviewed have difficulty entering the world of work, and when this occurs, it is usually linked to domestic and informal work, such as child care or cleaning. Thus, losing the capacity to work affects the subsistence, autonomy and self-esteem of women.
I lost work [...], they fired me saying that they didn't want anyone sick working for them. I got into a deep depression. [...] I worked as a house cleaner, raised four younger siblings, and was unemployed (W5).
The sexuality of women with SCD was marked by the decrease in interest/libido, which is influenced by two occurrences. The first is related to the fact that they experienced episodes of pain during the sexual act, which causes the fear of exposing themselves to new stimuli, thus contributing to the decrease of desire, refusal to meet and deprivation of sexual activity. In the second situation, which is more evident in women with leg ulcers, it has been noticed that, because they are ashamed and embarrassed when exposing their bodies with a wound, women with SCD feel less attractive and this alteration of the self-image contributes to indisposition for the sexual act.
[...] I myself don't feel like having sexual activity; I don't like him to stay on top of me... It bothers me... (W2).
Figure 2. Drawing story of a woman with sickle cell disease. Bahia, 2016
AN INJURED WOMAN
This drawing is from a woman who is going through a lot of pain; she is looking at that wound that bothers her a lot. She's a little crooked, her neck turned aside because the pain bothers her a lot and she's trying to help herself to see if the pain goes away. So this is what this drawing is; she tries to repair, but she can't; she walks awkwardly. (W5).
Pain also reduces the motivation for participation in daily activities, as well as changing the body posture that, over time, adds to individuals motor limitations and discomforts with their own image. In addition to the altered sexual experience, having SCD also showed interference in the maternity plans, which was influenced by the fear of experiencing abortion and the adversities of the illness of a child with this disease.
The issue of pregnancy is also... a complicated matter for me (tears)... because I've already lost two brothers... I dream of having children, but I don’t want this life of struggle anymore. I'm afraid to get pregnant, and then something happens and I can’t have the baby... (W1).
The social pain of men with sickle cell disease is expressed in the difficulty of being a worker, a provider and a sexually active man
In the perspective of the man with SCD, the social dimension of pain was directly related to the consequences of leaving the work and the expectation of changing the role of provider to the role of financially dependent on someone.
In my self-esteem, I interfere in this part because I worked and now I don't work anymore (M3).
The painful experience, during or after the sexual act, was commonly reported by men, and it sometimes contributed to the end of relationships. There is a prejudice about the sexuality promoted by the pain, whose interference occurs even before the sexual act, discouraging individuals to seek to meet their sexual need. However, when initiatives occur, the relationship is marked by pain that can occur in any part of the body.
Pain affects my sex life a lot, because if I'm at rest and have sexual intercourse, I feel my feet hurt, my knees hurt, my back hurts, my neck hurts, my elbows hurt... everything! Everything hurts, especially after ejaculation (M5).
Priapism is one of the complications of SCD presented by men, characterized by the painful and involuntary erection of the penis and usually causes sexual impotence, deeply shaking their referential masculinity. When speaking about priapism the participants were ashamed and embarrassed.
It prevents up dating. In the case of priapism, which we feel a lot, the sexual potency really decreases. I don't have it, but when I had it, I felt strong pain in the morning... (M2).
I had priapism all the time. Nowadays I don't have it any more. I used to have it two or three times a week; it was more often at night (M4).
The painful experience becomes disabling and interferes in the realization of personal development plans and projects, such as building a professional and family career. In this sense, men are hopeless, frustrated and very sensitive, with negative expectations about the outcome of the disease.
I had a dream of being a family man, having my children, my wife, my house, my job... If it rained or it was sunny, I would be there to secure my house... But that was a dream that I can't make come true today. (M5)
For men, happiness is closely linked to the realization of paternity plans, but SCD appears as an obstacle to the success of their life projects.
Figure 3. Drawing on the story of a man with sickle cell disease. Bahia, 2016
THE DISEASE INTERFERE IN HAPPINESS SOMETIMES 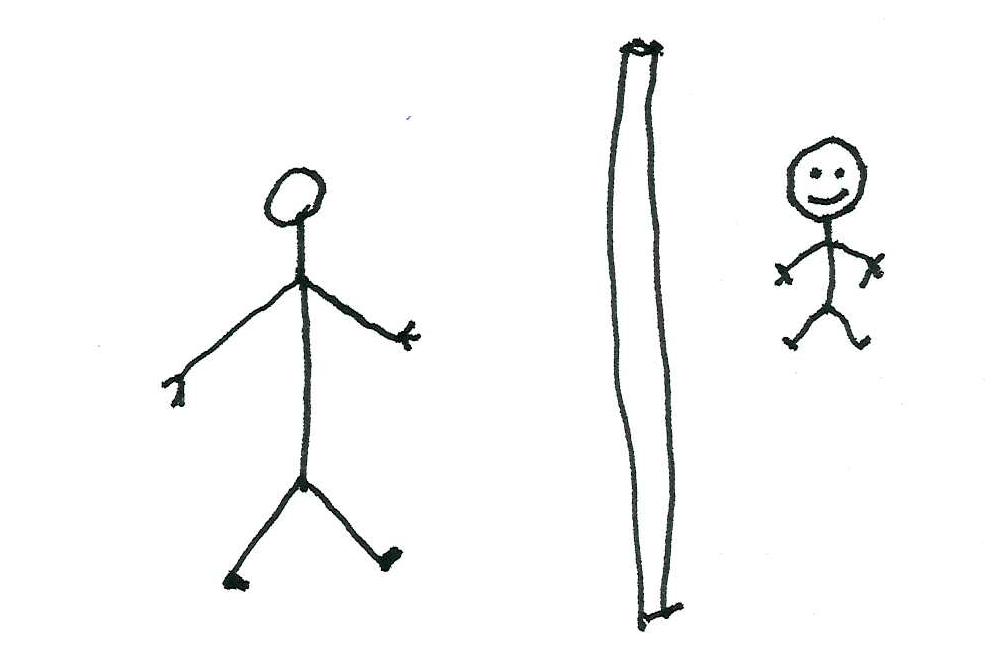
My drawing means the following: let's say that here I am the father; the boy is the son I want to have; and the wall means the disease that prevents me from fulfilling my dream of being a father, because if it were not for the illness I would have already had a child, but I try to avoid it because I don't want anyone suffering what I suffer. (M3).
While recognizing the ability to bear children, men, recalling the experiences of relationship rupture and erectile dysfunction, fear rejection by partners and abdicate the projects of being a father. For those who already experience paternity, the disease intervenes in the performance of expected tasks of the father, such as playing with the children, running with them and taking them to school, which leads to dissatisfaction.
For me it is terrible because the children have to be taken to school, but somebody else takes them and I stay on bed taking medicine and moaning, waiting for the pain to pass. (M11).
The man with DF experiences economic losses and the rupture of the social role played with the family and the community, as well as changes in sexuality and paternity.
DISCUSSION
Pain occupies a central place in the experience of people with SCD. Since childhood, they present pictures of dactylitis, painful crises, enlargement of the spleen, leg ulcers and hormonal changes with a consequent delay in sexual maturation, forging an identity marked by suffering, discrimination and inequality that characterize social pain.
Together, these bodily alterations affect self-image, self-esteem and self-confidence(8), provoking different reactions in patients, friends and relatives, which provoke the self-isolation and difficulties to initiate the first partnerships of friendship and courtship.
Among women with SCD, social pain is shaped by the complexity of fears, limitations and frustrations of socially constructed expectations. In this sense, their social pain involves the fear of spontaneous abortion, fear of raising a child with the disease, or of not fulfilling what is expected of a mother. These findings are in agreement with the study involving 25 women with SCD at reproductive age, which showed that the fact of wishing to become pregnant, satisfying the social expectation of motherhood, promotes conflicts, feelings of inadequacy and guilt. Most of them feel they are making a "mistake" when they get pregnant, given the possibility of the child being born with the disease. The experience of having an abortion or losses of other relatives due to complications of the disease also contribute to increase the fear of women with SCD who wish to become mothers(8).
Frustrations, irritability, feelings of self-disgust, mood swings and depression are evidenced from social losses due to chronic illness, both in women and men with SCD. Frustrations, irritability, feelings of self-disgust, mood swings and depression are evidenced from social losses due to chronic illness, both in women and men with SCD(9).
According to a review study on the implications of chronic pain in family relationships, close people, such as spouses, may either overestimate or underestimate complaints of family pain. Both judgments, however, are detrimental to the relationship, since, by overestimating the complaints, there is a tendency to adopt behaviors of overprotection that hinders the protagonism of the people and hurts their autonomy. On the other hand, underestimating implies more criticism and less support, which can intensify the feeling of abandonment and loneliness and, consequently, lead to social pain(9, 10).
In a qualitative study conducted in patients with neuropathic pain, difficulties in planning social activities due to the unpredictable nature of pain were identified as the main cause of limitations to fulfill social commitments(11).
Men resent the loss of the ability to work and suffer from the impossibility of maintaining the material conditions of existence given the limitations imposed by physical pain. They often feel a "burden" in assuming the position of financial dependency of family members. A study in which narratives of men with SCD were heard revealed that the disease prevents the continuity of work activities, culminating in unemployment and an obstacle to remain as provider of the family and responsible for the maintenance of its members(12).
The fear of reliving the feelings of social pain, avoiding new contacts or moving away from family and friends, is similar to the experience of women with leprosy, in which self-isolation adopted as a way of self-protection against discrimination impoverishes the support network or prevents the necessary support for people in situations of vulnerability(13).
A study that listened to people with low back pain and disc hernias identified that these people construct narratives that help them understand attitudes toward the limitations imposed by pain, such as “to continue life without pain” and “life with pain continues”. The first narrative influences the dogged pursuit of elimination of pain while maintaining a strict regimen of pain control. In the second, on the other hand, people tend to establish strategies and find ways to a functional life even with the continuity of pain(14).
Both the women and the men in this study revealed the interference of pain in their daily activities, as well as participants in another study that included people with neuropathic pain after spinal cord injury. The latter alleged that they perceive themselves in a constant battle for the control of their own life, the pain being the adversary. This perception of loss of control is directly related to the low acceptance of pain, while the sense of greater acceptance of pain leads the person to choose to stop fighting it(15).
The social pain in women is based on the failure to perform domestic tasks, whereas in men it is based on the non-fulfillment of the role of worker/provider. This perspective links women to the home space, historically reserved for the female sex, and the public space destined for men in the sexual division of labor(5)
Although women have occupied public spaces in the last decades, it can be seen in this research that women with chronic diseases are increasingly confined to the domestic space and the role of caregiver in an informal way. This does not guarantee them financial autonomy or labor rights capable of maintaining their material subsistence when pain prevents them from working. While recognizing their limitations in meeting social expectations, the power of reproducing gender stereotypes becomes explicit when women feel unable to continue caring for family members and resentful recalling that they fulfilled that role before disability(5).
The status conferred on men by their work plays an important role in the sense of identity, self-esteem, and psychological well-being(15). Thus, men with chronic disease with various manifestations in the body, as in the case of the SCD, who are unable to enter or remain in the labor market, are totally dependent on their relatives and, as a consequence, the frustration, impotence and uselessness to the world and life emerge(15).
Another aspect of the social pain of people with SCD evidenced was the change on the exercise of sexuality. Women, on the one hand, complained of loss of interest due to altered self-image, because they perceived themselves less attractive. Men, on the other hand, complained that pain prevents them from performing the sexual act due to priapism and erectile dysfunction(16). Negative sexual experiences affect socially constructed referrals of masculinity and alter paternity projects(16).
The self-devaluation of women in this study is similar to the result found in a study on women with chronic wounds who, because they live with odors, secretions and scars, lose self-confidence and self-esteem(17). It should be noted that in the SCD, leg ulcers appear at a very young age in the periods of greatest effervescence of social contacts(17).
In the case of men, the harm that can be caused on sexuality can happen even before the sexual act, since physical pain discourages them from seeking to meet their sexual need. In addition, at times when there are initiatives, sexual interaction is marked by pain that can occur in any part of the body. Moreover, the social pain left by the consequences of priapism hurts the masculinity of men with SCD who suffer from early shame when they are mistaken for sexual perverts, and once their sexual performance is modified by erectile dysfunction, they suffer from the constant fear of “failing” at the time of sex(18).
As found in the reports of men with SCD from this study, the results of another study indicate that chronically ill men avoid getting close to representations of fragility and passivity, considered attributes or qualities typically feminine. And, in addition to feeling pressured to play a sexual role in interacting with partners, they test their masculinity through active action in the relationship, denying the problem, and often subjecting themselves to undesirable or painful situations to meet social expectations(19).
As for changes in paternity, the social pain was revealed in the non-realization of the plans to be a father, either by infertility or erectile dysfunction, by the lack of financial autonomy to fulfill the parental function (provide care with food, clothing, education, health, and others) or by not being able to follow the activities of the children as they idealized(19,20).
The way women and men experience social pain in SCD is closely related to how they see themselves within the frame of reference defined by and in the culture, projecting ideals to drive their plans of being in the world.
CONCLUSION
This study aimed to understand the repercussions of social pain on the gender roles of women and men with SCD. The participants in this study were characterized by low level of schooling, low socioeconomic status and, consequently, greater financial dependence on family members.
The social dimension of pain is experienced by women and men, with similarities in suffering because of the lack of job opportunities that guarantee them a place socially recognized and valued. As for sexuality, it can be inferred that men, even under stress caused by pain before and after the sexual act, maintain the initiative for sex, failing to do so only in view of the limitations on erection caused by the subsequent events of priapism. Women, on the other hand, seemingly lose their sexual interest because they fear new seizures or because they feel less attractive when they have leg ulcers.
In both sexes there is frustration over unplanned projects of building a family and exercising motherhood/parenthood either because they fear that their children will be born with the disease or because the complications prevent them from maintaining reproductive functions successfully or because the economic needs restrict access to the material conditions of existence that assure them to assume the expenses foreseen in parenthood.
Regarding the methodological limitations, because it is a qualitative research, its results cannot be generalized. Moreover, the fact that the sample was composed mainly of socially and economically disadvantaged people from a city in the interior does not allow us to infer that the social dimension of pain is a reflection of the same causes that afflict people of different social classes residing in capitals, since social pain is influenced by context, the availability of services and support networks.
This study highlights that people suffering from SCD can benefit from sensitive listening in a multiprofessional care approach, which considers gender determinations as a marker of social expectations that influence their life projects, helping them to cope with the changes that cause them pain that cannot be minimized with medicines.
REFERENCES
1. Dalgleish T, Walsh ND, Mobbs D, Schweizer S, Van Harmelen AL, Dunn B, et al. Social pain and social gain in the adolescent brain: A common neural circuitry underlying both positive and negative social evaluation. Scientific reports.(Online) [Internet] 2017 Mar [cited 2018 Jun 20] 7, 42010. Available from: https://authors.library.caltech.edu/74244/1/srep42010.pdf
doi:10.1038/srep42010.
2. Meyer ML, Williams KD, Eisenberger NI. Why Social Pain Can Live on: Different Neural Mechanisms Are Associated with Reliving Socialand Physical Pain. PLoS One. (Online) [Internet] 2015. Jun [cited 2018 Jul 05]10;10(6): e0128294.Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0128294 doi: 10.1371/journal.pone.0128294.
3. Arduini GAO, Rodrigues LP, Marqui ABT. Mortality by sickle cell disease in Brazil. Rev Bras Hematol Hemoter. 2017;39(1):52–6.
4. Alencar SS, Junior CJC, Guimarães BF, Cunha DP, Rocha LV, Teixeira FEN, et al. Complicações clínicas mais prevalentes em pacientes portadores de Doença Falciforme de uma cidade de médio porte de Minas Gerais. Brasil. Rev. med. Minas Gerais (Online) [internet] 2015. Nov [cited 2016 abr 06 ]; 25(2):162-6. Available from: file:///C:/Users/Juliana%20Moraes/Downloads/v25n2a04.pdf
5. Anjos, KPL.; Lima, MLC. Gênero, sexualidade e subjetividade: algumas questões incômodas para a psicologia. Psic em Pesq. (Online) [Internet] 2016 [cited 2016 Mar 25] 10 (2):49-56.Available from: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1982-12472016000200007
6. Mendes MR, Miskulin RGS. A análise de conteúdo como uma metodologia. Cadernos de Pesquisa. 2017 Jul [cited 2018 Jun 22] 7(65):1044-1066.
7. Rivemales MCC, Rodrigues GRS, Paiva MS. Técnicas projetivas gráficas: aplicabilidade na pesquisa em representações sociais – revisão sistemática. Online Braz j Nurs (Online) [Internet] 010[cited 2016 Mar 25]9(2). Available from: http://www.objnursing.uff.br/index.php/nursing/rt/printerFriendly/j.16764285.2010.3153/704
8. Xavier ASG, LopeS DM, Ferreira SL. Uso de métodos contraceptivos por mulheres com anemia falciforme. Cienc Cuid Saude 2014 Jan [cited 2016 Apr 10] 13(1):27-34.
9. Riffin C, Fried, T, Pillemer K. Impact of Pain on Family Members and Caregivers of Geriatric Patients. Clin in geriatric med, 2016 (Online) [cited 2016 Mar] 32(4): 663-675. Available from: doi: 10.1016/j.cger.2016.06.010
10. Campbell P, Jordan KP, Smith BH, Scotland G, Dunn KM. Chronic pain in families: a cross-sectional study of shared social, behavioural, and environmental influences. Pain, 2017 [cited 2016 Mar] 159(1): 41-47.
11. Dueñas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016 (Online) [cited 2016 Jun 28] 9:457-67. Available from: doi:10.2147/JPR.S105892
12. Marques PA, Xavier ASG, Carvalho ESS, Lacerda KL, Ferreira SL. Experiências afetivas e sexuais de homens com doença falciforme e úlceras de perna. Rev ABPN. 2015 [cited 2016 Jun 28] 7(16):128-53.
13. Gonçalves M, Prado M, Rodrigues A, Silva SS, Santos KS, Araujo PN, et al. Trabalho e hanseníase: as mulheres em suas dores, lutas e labutas. Rev. Bras. Enferm. 2018 (Online) [Internet] [citado 2019 Mar 04] 71(Suppl 1): 660-667. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672018000700660&lng=pt. http://dx.doi.org/10.1590/0034-7167-2017-0598.
14. Angel S, Jensen LD, Maribo T, Gonge BK, Buus NS. Narratives of life with long-term low back pain: A follow up interview study. J Pain. [Internet] 2017. [cited 2017 Oct 18] 2 (1):382-389. Available from:doi: 10.1016/j.sjpain.2017.09.018.
15. Sousa LP, Guedes DR. A desigual divisão sexual do trabalho: um olhar sobre a última década. Estudos Avançados, 2016, 30(87): 123-139.
16. Borsa JC, Nunes MLT. Aspectos psicossociais da parentalidade: O papel de homens e mulheres na família nuclear . Psicol. Argum. 2017 Jan 29 (64):31-39
17. Lacerda FKL, Carvalho ESS, Araújo EM, Miranda NBA, Dias ALA, Almeida TA. Mulheres com anemia falciforme (con)vivendo com as úlceras de perna e a dor. Rev Enferm UFPE 2014 (Online) [Internet] [cited 2017 Apr 17] 8(7):2054-60. Available from:http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/view/4983/pdf_ 5513
18. Maia HAAS, Alvaia MA, Carneiro JM, Xavier ASG2, Bessa Júnior J, Carvalho ESS. Acesso de homens com doença falciforme e priapismo nos serviços de emergência. BrJP. 2019 jan (Online) [Internet] [cited 2017 May 17] 2(1):20-6. Available From: http://www.scielo.br/pdf/brjp/v2n1/pt_2595-0118-brjp-02-01-0020.pdf
19.Hearn JH, Cotter I, Fine P, A Finlay K. Living with chronic neuropathic pain after spinal cord injury: an interpretative phenomenological analysis of community experience. Disabil Rehabil. 2015 [Internet]37(23):2203-11. Available from: doi:10.3109/09638288.2014.1002579.
20. Silva RMCRA, Oliveira DC, Pereira ER, Silva MA, Trasmontano PS, Alcantara VCG. Humanization of health consonant to the social representations of professionals and users: a literary study. Online Braz J Nurs. 2014 [internet] [cited 2017 Oct 22] 13(4):677-85.Available From: http://www.objnursing.uff.br/index.php/nursing/article/view/4773/pdf_314
All authors participated in the phases of this publication in one or more of the following steps, in according to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the version submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received:2018/07/25
Reviewed: 2019/03/22
Approved: 2019/09/20