Experience of guardians of adolescents in vaccination against papillomavirus: phenomenological study
Valéria Conceição de Oliveira1, Mariana Rodrigues da Silva1, Selma Maria da Fonseca Viegas1, Eliete Albano de Azevedo Guimarães1, Deborah Franscielle da Fonseca1, Patrícia Peres de Oliveira1
1 Federal University of São João del-Rei
ABSTRACT
Objective: to understand the experience of those responsible for adolescents in relation to vaccination against human papillomavirus. Method: qualitative study based on Alfred Schütz's Social Phenomenology. Data were collected from October to December 2014, through interviews with 14 adults responsible for adolescents who accepted or refused the vaccination. Results: the meanings expressed indicate the reasons for vaccinating adolescents: for prevention; to ensure a better future for the daughter; for the daughter to be healthier. The reasons for not allowing teenagers to vaccinate were: lack of information on the vaccine's effectiveness and the vaccine can encourage early sexual initiation. Conclusion: the experiences and feelings experienced by those responsible for the adolescents regarding the vaccine against human papillomavirus, associated with the cultural context, lead to the vaccination or the refusal to vaccinate the adolescents.
DESCRIPTORS: Papillomavirus vaccines; Adolescent Health; Collective Health; Nursing.
INTRODUCTION
Cervical cancer (CC) remains a major public health problem, it is the second most common type of malignancy worldwide, especially in less developed regions. If preventive actions are not implemented in these regions, a 63% increase in the number of deaths from this disease is expected in 2025(1,2).
In Brazil, the estimated incidence for 2016 was 16,340 new cases, with an estimated risk of 15.9 cases/ 100 thousand women(3). Data show that every year more than 270 thousand women die from CC, with over 85% of these deaths occurring in low and middle income countries, resulting from poor access to health services for early detection and treatment(1).
Cervical cancer is the final stage of unresolved human papillomavirus (HPV) infection, currently defined as a persistent presence of HPV DNA (deoxyribonucleic acid) in repeated cervical smear tests. Most HPV infections resolve spontaneously and are asymptomatic. However, when persistent infection with specific types of HPV occurs, with types 16 and 18 being more common, it can result in precancerous lesions as a consequence. HPV types 6 and 11 (low risk) are associated with condyloma acuminata, not cervical cancer(2).
Since 2006, the quadrivalent vaccine that protects against viral types 6, 11, 16 and 18, and the bivalent vaccine, which offers protection against types 6 and 11, have been licensed in more than 100 countries, and since 2012 they have been introduced into national immunization programs in at least 40 countries. Both vaccines are highly effective, both in preventing persistent infection with HPV 16 or 18, and in preventing cervical intraepithelial neoplasia (CIN) 2 and 3(2,4).
Vaccination should take place in pre-adolescence and adolescence, since in older ages this it is associated with a lower cost-effectiveness ratio, due to the greater propensity of these women to previous exposure to HPV(2). Sexually active women may even benefit, but only for protection against subtypes of viruses that have not yet beenacquired(4).
In Brazil, the quadrivalent vaccine against human papillomavirus was introduced in the National Immunization Program in 2014, in the public health service network, for female adolescents aged 9 to 13 years and from 2017 for males. The immunobiological is available in all Primary Health Care Units (PHC) of the Unified Health System(5).
Despite the importance of the HPV vaccination, there is a resistance in the media and social networks by some people against vaccination, with many controversies and discussions, such as adverse events, sexuality, among others. In order for an immunization program to be successful it is important that vaccines are safe and accepted by the population (6). Logistical factors, lack of inputs, professionals with low preparation to work with the population, among others, compromise the goals established for the prevention of vaccine-preventable diseases, and can have a negative impact on the credibility of this action.
In the United States of America, controversies over compulsory HPV vaccination began before the vaccine was licensed, when some religious conservatives expressed concern that the availability of a sexually transmitted infection vaccine could harm abstinence-based prevention messages. Family advocacy groups believed that mandatory vaccination constituted an attempt by the State to force a child to undergo an intervention that could be incompatible with the family's religious values and beliefs(7).
As the vaccination against HPV in the public service in Brazil is recent, there is a scarcity of Brazilian studies on the social perception of the HPV vaccine. The relevance of this study is based on the fact that it allows understanding of the experience of these mothers/guardians regarding the HPV vaccine of their adolescent children/grandchildren, based on their action in the lived world, in the social relationships established and that are connected to the decision whether or not to allow vaccination, expressing their feelings and their need for knowledge on the subject.
In view of the complexity of the issue surrounding HPV, the following concerns guided this study: how did the guardians experience HPV vaccination for adolescents? How do you perceive the approach of health services in relation to vaccination against HPV? What are your expectations when accepting or refusing to vaccinate the adolescent?
Thus, this research aimed to understand the experience of those responsible for adolescents in relation to vaccination against human papillomavirus.
METHOD
A qualitative study based on Alfred Schütz's Social Phenomenology. This theoretical-philosophical framework allows us to unveil the sense of being in the world, of being-with-the-other, contextualized in social relations, in the shaping of experience and action, understood as an intersubjective space, in the social process. Thus, it offers a systematic method for a better understanding of the social, spatial and temporal dimensions of the life world(8). In this present study, the experiences narrated by the guardians of adolescents culminated in the unveiling of their experiences in relation to the HPV vaccination of their daughters/granddaughters. These, despite being inscribed in the subjective universe of mothers/ fathers/grandparents of adolescents, also reflect a social sense configured from the intersubjective relationships they establish with others in the everyday world.
It is understood that in this framework, reality is built by people for themselves, from their intersubjective experiences. The social relationship is fundamental in the interpretation of the meanings of human action in the everyday world, a scenario where the individual lives and on which he has the scope to intervene, transforming himself continuously and modifying social structures (9), which can be unveiled in experience of adolescents' parents / grandparents in relation to HPV vaccination. The comprehension of the studied phenomenon, involved the evaluation of social behavior in relation to an action and the lived experience and unveiled their expectations in relation to the future, in addition to their daily life in the time when elements act, interact and understand themselves within the so-called social world make sense, and are means to justify their ends and how to proceed or live.
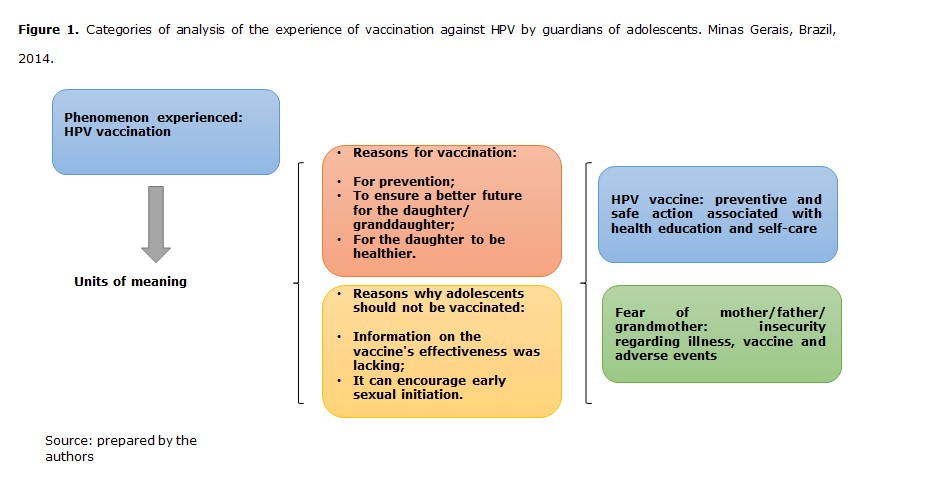
According to this phenomenological approach, social action is based on a project that man proposes to carry out and is motivated by existential goals that point to the future - "a reason for" - and for reasons based on lived experiences - "a reason because "(8). The analysis categories were identified, according to Figure 1.
The study was performed in a municipality in Minas Gerais, with 100% coverage by the Family Health Strategy (ESF), with six teams as research scenarios, with a diverse territory including urban and two rural teams, with differences in the social production of health.
Inclusion criterion were participants who considered themselves responsible for adolescents in the research scenario in this case, vaccination against HPV. Exclusion criteria were parents/grandparents with mental disorders or any other condition that could interfere with the interview. Thus, 14 guardians of adolescents participated, among them, nine mothers, three fathers and two grandmothers, aged between 33 and 60 years, and 11 accepted the vaccination for the teenager and three guardians refused the vaccination.
In order to identify the guardians who did not accept the vaccination, contact was made with the Municipal Health Secretariat of the municipality, which provided the names and addresses. Four adolescents who did not receive the vaccination were identified and after contacting and explaining the research objective, three guardians agreed to formally participate in the study. It is worth mentioning that mothers/guardians from all ESF units participated.
The statements were obtained between October and December 2014. The interviews were conducted at the participants' homes, in a private place, after explaining the research objectives. Permission was obtained to use the recorder in order to fully record the statements and their subsequent analysis.
The interviews lasted an average of 40 minutes, guided by the following questions: what was your experience of the HPV vaccination for your daughter/granddaughter? How would you like this HPV vaccination to have been addressed? What do you expect from the future, based on your decision to vaccinate or not to vaccinate the teenager? In order to guarantee the anonymity and confidentiality of the information, the participants were identified by the letter E (interviewee) followed by the sequential number of the interview.
The number of participants was not pre-established, but defined at the time the objective of the study was achieved.
Data analysis consisted of a systematic procedure for organizing and categorizing the material. Initially, they followed the steps of global reading of the testimony and the extraction of the units of meaning, according to the common sense understanding of the description of the phenomenon. The stages of transformed units of meaning, convergence and divergence of meaning were established, concretizing the essential reduction for the existence of the phenomenon, based on the experience of the research participants. Finally, interpretation and understanding were performed, which are configured in the discussion of results in the light of Alfred Schütz (8) and studies related to the theme.
The research was developed according to the guidelines and regulatory standards for research involving human beings, Resolution No. 466 of December 12, 2012. Thus, data collection started after the approval by the University's Research Ethics Committee Federal of São João del-Rei, Brazil under number 703.819 and CAAE: 31442714.0.0000.5545.
RESULTS
The meaning of the action of the guardians, in the context of their experience on vaccination against HPV, was organized and presented in the categories: “HPV vaccine: preventive and safe action associated with health education and self-care”, “fear of mother: insecurity regarding the disease, the vaccine, and adverse events ”.
HPV vaccine: preventive and safe action associated with health education and self-care
The mothers/guardians of the adolescents see the vaccine as an important preventive measure and their concern about a healthier future for their daughters had an influence on the mothers' adherence to the vaccine.
Prevention for the future. In the future she will not have certain "problems" that she has today. Her future is going to be a lot safer than mine. Certain “problems” that I had, she will not have, because she will be prevented. It is a prevention. She will be a much healthier mother than I am. (E9).
It is a prevention, a prevention for her future life, an opportunity that, for example, my aunt did not have, my aunt died of CC. So, for her this is an advantage because she is in the risk group, right [...]? (E11).
The mother expresses the act of vaccinating as an act of maternal care to offer the best for her daughter.
I see it as prevention. We who are parents, I am the mother of a teenager, whatever I can do to prevent any disease, any harm that may come to my daughter, I think I will play my role as a mother [...]. (E13).
The experience of cancer in the family and the indication to vaccinate by the pediatrician was among the reasons that influenced the decision to vaccinate.
Because of having cases of cancer in the family, CC, bowel cancer, my sister passed away, and the other was CCU, I think she was 27.(it was the reason for deciding to vaccinate) [...]. (E10).
[...] even my daughter is accompanied by a pediatrician and he had already suggested that she take it, but at the time it wasn´t free, it wasn´t free on the public health network, and I was already thinking about giving her these doses of the vaccine. Then it became free on the public health network, I was already thinking about buying it privately, and it became free, so that was what led me to consent [...]. (E13).
The adolescent's interest in being vaccinated also had an influence on parental acceptance:
[...] she took it of her own free will and was so excited about the vaccine, there was going to be a vaccine for her to take, she even had the initiative to want to take it, so I didn't even force it, I didn't force her to go “there ”and get the vaccine [...]. (E1).
The mother's confidence in the protection offered by the vaccine was identified, as it was prepared, analyzed and tested before being indicated for human use.
[...] they never release a vaccine that isn´t protective, because they do the research first, look at everything first, right [...]? (E2)
Officials reaffirmed the importance of the vaccine in disease control and cited the successful experience of the vaccine against childhood paralysis, as shown below:
[...] it will save, I think it saves a lot. A vaccine, the disease can even come like a lot of diseases, right? It protects her, it wouldn’t have the same effect as for her. Isn't that it? Just like you see, that paralysis vaccine, today you don’t see any more children with that disease [...]. (E2).
It was noted that medication alone is not enough. The context of the dialogue between parents and children, guidance, care, are relevant:
[...] but, it is not only through medicine and medication that we will be healthy. And our care is also personal [...]. (E5).
[...] if they were better oriented, especially society, if they were also orienting parents, because it is not easy, we know that it is not, a father sitting with his son and talking about it clearly, openly with him, but I think that it is still the best option to talk, to guide, to have a good orientation and to know what she will assume through her sexual life [...]. (E14).
Fear of mother/father/grandmother: insecurity regarding illness, vaccine and adverse events
The option of not vaccinating adolescents was argued by those responsible for the fear of vaccination and adverse events. Easy access to the internet and information awakens autonomy, but also the fear that influences the decision not to vaccinate.
[...] I also heard a lot about these reputable doctors, I saw on the internet that other countries that gave the vaccine, many girls had "problems". One even had paralysis in the entire body because of this vaccine. So, I don't understand why Brazil is bringing this vaccine if others had "problems" with it [...]. (E7).
[...] we also realized through our readings, our research that, in Japan, it was even abolished, the state was offering the vaccine and they took it out, due to the problems they had. There were more than two thousand cases of contraindications for the vaccine, it caused problems, even death, so from this aspect, we realized that the vaccine would not be such a good thing for a girl of twelve, thirteen, our daughter´s age, so we prefer not to let her take it [...]. (E14).
Another argument consisted of criticizing the age at which the vaccine was started, relating to encouraging early sexual life and, above all, attitudes of carelessness in relation to safe sex by adolescents, as they believe that the vaccine alone already guarantees protection:
[...] this for me is an incentive for girls to start sex earlier. Because at the age of nine, I think no teenager. Nowadays, it may even have one, but parents who are really responsible for their children will never let a nine-year-old child have sex. For me, nine years old is a child. So, I don't agree with vaccination [...]. (E7).
[...] I think that the teenager who is thirteen, eleven to thirteen years old if she did not have these guidelines, she will let herself be influenced, she will realize that she is already protected and that she will not have a problem anymore, and that she can enjoy sex as you please and often very wrongly [...]. (E14).
They express doubt regarding the vaccine's efficacy and effectiveness, however, they prefer to assume the risk than the feeling of guilt for not carrying out immunization care, as in the following statement:
[...] so you are having the opportunity to receive a vaccine, you may not even know if that vaccine will really have the necessary effect, but having the opportunity to receive it, you will run the risk, you don´t receive it and then you stay with a heavy conscience that he did not do what had to be done [...]? (E13)
In contrast, other mothers chose not to vaccinate their daughters for fear of the vaccine not being effective. They refer to information conveyed via the internet that influenced the decision not to vaccinate:
[...] I don't agree with vaccination. I do not agree, because I saw on the internet that some doctors even reported saying that no ... There is no guarantee of effectiveness. And others have said that if you have it, it will only be one for five years. So, I don't agree, because I will also vaccinate now and next year will be at the age of nine? He says it will go on for nine years. So, I think it is totally wrong [...]. (E7).
Regarding acceptability, an interviewee reports the need for satisfactory results of the safety and efficacy of the vaccine in preventing the disease through people who have already been immunized and have been protected from the disease:
[...] show an example ... of a person who took it and guarantees that this vaccine worked. In order to show us the certainty that this vaccine will really be valid for a long, long time [...]. (E5).
A father also believes that there is an unclear interest behind the vaccination and this causes him to be unsure about the decision to vaccinate.
[...] we are not sure, what is the interest behind this, these vaccines? There are a lot of questions that sometimes we are like this, it does not give us a sense of security [...]. (E14).
DISCUSSION
Considering the relevance of vaccinating and the context of effective communication and health education for effective interventions in the prevention of risks and injuries, the results of this study contextualize these typifications in the constructs lived and experienced in daily life.
Two types of reasons for social behavior are considered, according to phenomenological sociology: those that involve action and purpose, which are the “reasons for”, and those that assume the scenario of the actors, the environment, the psychic disposition are the "reasons why"(8).
The “reasons for”, given by the participants of this study, in order to vaccinate teenagers against HPV were: for prevention; to ensure a better future for the daughter; for the daughter to be healthier; to play their role as a mother. The "reasons" that underpin the decision to vaccinate adolescents were: cancer in the family; the pediatrician's indication to vaccinate; the vaccine is free in the public health network; the teenager's interest in vaccinating; confidence in the protection and manufacture of the vaccine; the vaccine saves from the disease; the vaccine ended the childhood paralysis disease; the risks of vaccinating so as not to take the blame for not vaccinating. And the "reasons" for not allowing teenagers to vaccinate were: lack of information regarding the vaccine's effectiveness; the vaccine can encourage early sexual initiation; what is behind this vaccination? It is very obscure. These reasons for not vaccinating adolescents are understandable to the researchers by weighting the subject(9).
Thus, the primary constructs express the sense of the natural attitude in the world of these research participants, who have knowledge of common sense, of the information sought, transmitted and interpreted in the light of their experiences and contextualized in a social environment, as one expresses desires and perceptions that others reaffirm or inquire about.
The factors involved in the acceptability of the vaccine by parents are related to critical capacity regarding the knowledge about the vaccine, the age of vaccination, the way they approach sex education, fear of adverse events and the lack of trust regarding a new vaccine(10).
Research conducted with mothers who refused vaccination, showed that they had worse knowledge about CC, especially the relationship with HPV and sexual activity. There was a general consensus that the vaccine had "come out of nowhere" and therefore long-term side effects could not be predicted(11). In addition to the suspicion that a very expensive vaccine was being offered free of charge and therefore be of low quality or being tested on girls as part of a clinical vaccine trial(12).
Concerns about the age group, negative effects of vaccination such as promiscuity and concern about the safety of the vaccine, such as side effects, were also influential factors in refusing vaccination(11,13).
In a study conducted in the United States of America, the authors' perception was that, for most mothers who refused the vaccine, the reason resulted in a low-risk combination due to the lifestyle imposed by Judaism related to beliefs about sex before of marriage and the concern about being a new vaccine and its effects may appear in the long term (14). This illustrates that parents mistakenly believe that the HPV vaccine is only necessary if there is sexual activity (13). Some parents considered that the HPV vaccine would be a way of giving a “carte blanche” to sexual relations and weakening self-care practices(10).
Thus, we can see that the way in which a controversial issue is approached, such as vaccination against a sexually transmitted disease, may or may not interfere in the decision-making process of vaccination. Many of the mothers, both of whom accepted or refused, thought that the vaccine was being offered at a very young age, expressing the opinion that their daughters were not sexually active and some mothers were concerned with discussing sexual issues with their daughters at that age (10,13). The guardians do not feel prepared to address sexuality with adolescents and, believe that the best would be for professionals to do it during the vaccination (12).
When identifying the reasons why adolescents were not vaccinated against HPV, parents' lack of trust regarding the vaccine was one of the main reasons(10). Immunopreventable diseases are becoming less common and, as a result, parents' concerns are directed towards safety and the need for vaccines (11,14). However, the risks regarding vaccination have been known since the beginning of their use, however, in developing countries, such as Brazil, the focus is still concentrated on maintaining high vaccine coverage and the issue of vaccine safety has not received the same attention given developed countries (4). Pre-vaccination counseling must go beyond the benefits of the vaccine and the risks related to the disease, it must consider the doubts, fears and risks of serious adverse events (14).
Parents' decisions are also made in a broader context of beliefs about their children's health, personal experiences, perceived norms, and trust in health systems and professionals. The parents' position is the starting point for health professionals to choose the most appropriate communication strategy. Naturally, these will vary according to needs, individual circumstances and beliefs(10).
Research highlights that there is more acceptability to the vaccine when there is more information, advice from health professionals or family members (13), therefore, communication and health education is important, so that parents feel safer with the new vaccine and are willing to question and remove doubts that may arise with new preventive measures.
It should be noted that, despite covering the experience of those responsible for HPV vaccination, in daily life considering sociality, this is not an absolute reality for everyone who is living with HPV vaccination of adolescents, indicating the need for other approaches in different realities, which can be highlighted as a limitation of the study. Nevertheless, the results obtained provide important elements for planning actions that aim to meet the specific needs of those responsible.
The information, which is still incipient about the HPV vaccine, the importance of vaccination, what is HPV and the mode of transmission, are notions that should be regularly shared with the population by health professionals and specifically, those in nursing who are protagonists in the vaccine room.
The “fear of the mother” is clear in her position as a caring and protective woman, when she expresses doubts about the safety and effectiveness of the vaccine. This investigation warns of aspects that transcend the organization of services and preventive actions for preventable diseases, as one of the priorities within the scope of SUS.
It is expected that the health system, made up of institutions, professionals and civil society, is prepared to respond to the deficiencies and conflicts that impact on the daily activities of health care, especially in the preventive approach to risks and harm and health promotion which is everyone's right.
CONCLUSION
The results of the present study made it possible to understand the experience of mothers/fathers/ grandparents in the context of the HPV vaccine of their adolescent children/ grandchildren. It was possible to apprehend the way in which these guardians deal with vaccination, in their daily lives, facing insecurity in the face of the disease, the vaccine and adverse events. This approach broadens the discussion about the lack of information and knowledge of lay people about HPV vaccination.
At the same time, it was possible to characterize typical attitudes and behaviors of the guardians. Their experiences compose a social sense, as those responsible belong to a social group, with their individualities, senses, feelings and notions.
The HPV vaccine, the protection against HPV infections, was guaranteed for adolescents in the recommended range, as a response from the State as a right to health due to CC. This relevant measure is understood by those responsible for adolescents, on the one hand, as a necessary preventive action for the control of the disease, and on the other, as something unnecessary that interferes with beliefs, cultures, lifestyle when considering some participants in the research that did not accept vaccination.
REFERENCES
1. Global Burden of Disease Cancer Collaboration. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol [Internet]. 2017 Apr [cited 2017 Mar 23];3(4):524-48. Available from: file:///C:/Users/User/Downloads/2016-CA-_A_Cancer_Journal_for_Clinicians.pdf
2. Sainato R, Flores M, Malloy A, Geaney C, Rajnik M, Ottolini M, et al. Health maintenance deficits in a fully insured population of adolescents with chronic medical conditions. Clin Pediatr [Internet]. 2017 [cited 2017 Mar 23]; 56 (6): 512-18. Available from: http://journals.sagepub.com/doi/pdf/10.1177/0009922816678183
3. Brasil. Ministério da Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativas 2016: incidência de câncer no Brasil [Internet]. Rio de Janeiro: INCA; 2016. [cited 2017 Mar 03]. Available from: http://www.inca.gov.br/estimativa/2016/estimativa-2016-v11.pdf.
4. Kumar S, Biswas M, Jose T. HPV vaccine: current status and future directions. Med J Armed Forces India [Internet]. 2015 [cited 2017 Mar 03]; 71(2):171-77. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0377123715000258 doi:https://doi.org/10.1016/j.mjafi.2015.02.006
5. Barreto JAPS, Marinho MNASB, Vidal ECF, Pinto AGA, Aquino PS, Vidal ECF. Feelings of women with human papilloma virus regarding their infection: an exploratory study. Online Braz J Nurs [Internet]. 2016 [cited 2017 May 16];15 (3):382-92.Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/5305.
6. Keim-Malpass J, Mitchell EM, DeGuzman PB, Stoler MH, Kennedy C. Legislative activity related to the human papillomavirus (HPV) vaccine in the United States (2006–2015): a need for evidence-based policy. Risk Manag Healthcare Policy [Internet]. 2017 [cited 2017 May 16];10:29-32. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5356918/ doi: 10.2147/RMHP.S128247
7. Voss DS, Wofford LG. Human Papillomavirus vaccine uptake in adolescent boys: an evidence review. Worldviews Evid Based Nurs [Internet]. 2016 [cited 2017 May 16];13(5):390-95. Available from: https://sigmapubs.onlinelibrary.wiley.com/doi/abs/10.1111/wvn.12172 doi:https://doi.org/10.1111/wvn.12172
8. Schutz A. Sobre fenomenologia e relações sociais. Trad. Wagner HTR. Petrópolis: Vozes; 2012.
9. Oliveira MD, Merighi MAB, Kortchmar E, Braga VA, Silva MH, Jesus MCP. Experience of women in the postoperative period of bariatric surgery: a phenomenological study. Online Braz J Nurs [internet] 2016 [cited 2017 May 12]; 15(1):1-10. Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/5167
10. Giambi C, D’Ancona F, Del Manso M, De Mei B, Giovannelli I, Cattaneo C, et al. Exploring reasons for non-vaccination against human papillomavirus in Italy. BMC Infect Diseases [Internet]. 2014 [cited 2017 June 09];11(14):545.Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-014-0545-9
11. Ojinnaka CO, McClellan DA, Weston C, Pekarek K, Helduser JW, Bolin JN. Determinants of HPV vaccine awareness and healthcare providers' discussion of HPV vaccine among females. Prev Med Rep [Internet]. 2017 [cited 2017 June 26];5:257-62. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5262500/
12. Fu LY, Zimet GD, Latkin CA, Joseph JG. Associations of trust and healthcare provider advice with HPV vaccine acceptance among African American parents. Vaccine [Internet]. 2017 [cited 2017 June 10];35(5):802-07. Available from: https://www.ncbi.nlm.nih.gov/pubmed/28063706
13. Lai D, Bodson J, Davis FA, Lee D, Tavake-Pasi F, Napia E, et al. Diverse families’ experiences with HPV vaccine information sources: a community-based participatory approach. J Community Health [Internet]. 2017 [cited 2017 June 29];42(2):400-12. Available from: https://link.springer.com/article/10.1007/s10900-016-0269-4
14. Moss JL, Reiter PL, Truong YK, Rimer BK, Brewer NT. School entry requirements and coverage of nontargeted adolescent vaccines. Pediatrics [Internet]. 2016 [cited 2017 June 10];138(6):Pii: e20161414. Available from: https://pediatrics.aappublications.org/content/138/6/e20161414
ACKNOWLEDGMENT
The project funded by the National Council for Scientific and Technological Development - CNPq, Public Notice No. 001/2014 / PROPE.
Received: 05/18/2017
Revised:01/15/2020
Approved:01/15/2020