Biomarkers of stress in preterm newborns exposed to bath: a pilot study
Patrícia de Freitas1, Amélia Fumiko Kimura2
1 University of São Paulo
Abstract
Introduction: the corporal hygiene of the preterm newborn, although it is a recommended and routine practice, requires caution and safety for provoking disorganization in the autonomic system and homeostasis imbalance. Aim: to evaluate the variation of heart rate, oxygen saturation and salivary cortisol levels of preterm newborns submitted to conventional immersion baths and swaddled in sheets. Method: this is a randomized, pilot, cross-over clinical trial with 15 clinically stable preterm newborns. Results: the mean heart rate and oxygen saturation after the conventional immersion bath and swaddled in sheet did not present significant clinical and statistical differences. There was an increase in the salivary cortisol concentration when comparing the pre and post-bath values in the two bath techniques. Conclusion: there were no significant differences in stress biomarkers when comparing the two bathing techniques.
Descriptors: Biomarkers; Infant, Premature; Heart Rate; Oxygenation; Skin Care; Neonatal Nursing.
INTRODUCTION
With the advent of the Neonatal Intensive Care Units (NICUs), preterm newborn survival (PTNB) has improved dramatically, neonatal mortality rates have declined and morbidity due to developmental disorders represents a new public health challenge(1).
However, hospitalization in the NICU represents a number of stressors that may negatively impact the growth and development of preterm infants. As an inherent part of medical care, the newborn (NB) is exposed not only to invasive therapeutic procedures, but also undergoes frequent manipulations of daily procedures such as diapering, hygiene, change of position and weighing(2). Minimizing excess stimulus to reduce its impact is one of the basic principles of development assistance, which rationally involves planning the care of the PTNB and ensuring the safest practices based on scientific evidence.
With interventions involving manipulations, PTNBs respond with stress reactions, such as increased heart rate (HR), desaturation and changes in skin conductance and pain score(3-**5). **The body of the RN exposed to the manipulation responds with increased energy expenditure and there is an association of this with a decrease in oxygen saturation (SpO2)(6).
The body's response to autonomic nervous system-controlled stress and response to environmental stimuli are immature in PTNBs, and any interventions and the NICU environment itself are stressors. Thus, it is necessary to analyze the adequacy of the interventions in order to avoid overloading and impairing the organic homeostasis, with risk of damages to the clinical condition of the child and prolong the period of hospitalization(7).
Variations in heart rate (HR), drop in oxygen saturation (SpO2) and increased salivary cortisol (SC) concentration(8) indicate stress due to overload of stimuli. If the stressor stimulus is not interrupted, bradycardia and SpO2 fall may occur, further aggravating clinical conditions.
One of the routine nursing procedures in the context of NICUs that provides multiple sensorial stimuli is the corporal hygiene of the PTNB. The Ministry of Health published the Handbook Humanized Care for the Low Birth Weight Newborn: Kangaroo Method in 2011(9), which recommends that the hygiene be performed by immersion bath technique, based on evidence that this procedure has less impact on the thermoregulation of low birth weight PTNB. Another recommendation is that the immersion bath is performed with the PTNB swaddled in a drain or sheet.
The technique of wrapping PTNBs in a sheet, swaddling-cloth or blanket, known as swaddling or wrapping technique, is an intervention procedure that has been used as an effective non-pharmacological analgesic measure for acute painful procedures(10,11) to promote sleep quality in NBs, in this case, with controversial evidence for its benefit and risk(12,13) and as a measure to restrict NB movement during magnetic resonance imaging(14). There is a lack of evidence on the benefit and safety of the immersion bath with PTNB wrapped in sheet or swaddling-cloth. The only published clinical study evaluated the effect of the immersion bath swaddled in a cloth in PTNB on body temperature and crying time and the results showed that these babies presented lower thermal variation and less crying time compared to those who received conventional immersion bath(15).
Considering the absence of documented evidence on other outcomes as biomarkers of stress induced by the cited procedure, the objective of this study was to evaluate the variation of HR, SpO2 and SC levels in PTNB infants submitted to conventional immersion baths swaddled in sheets.
METHOD
This is a cross-sectional clinical trial, with a sample of 15 PTNBs admitted to the neonatal unit of a school hospital in the city of São Paulo. The PTNB were randomized to the bath sequence in two groups: Group A submitted first to the conventional bath (CB) and then to the swaddled bath (SB); and Group B submitted to SB followed by CB. Because it was a cross-over trial, each subject had self-control and received both the control and experimental interventions. Cross-tests require a smaller sample, in addition to avoiding problems of comparison between the control and experimental groups(16). The subjects were included in the study according to the randomization list of the order of bath types. The interval between the two types of bath ranged from 24 to 72 hours. The baths occurred in the morning period (7:30 a.m. to 8:45 a.m.).
Data were collected from March to April 2014. The eligibility criteria were: corrected gestational age ≥ 33 and < 36 weeks and 5 days; postnatal age > 24 hours; clinically stable; spontaneous breathing; absence of congenital anomaly; heart disease; sedation and previous surgeries; and minimum interval of one hour after feeding.
The PTNBs were naked and immersed in the tub with water covering the entire body surface, except for the neck and head. In the swaddled bath (SB) the PTNBs were naked, wrapped in a cradle sheet, and then immersed in the bath water. The technique of immersion bath swaddled in sheet was adopted, as recommended in the Kangaroo Method of the Ministry of Health(9). The water temperature was maintained between 38ºC and 40ºC, the minimum ambient temperature during the baths was 27ºC and the average bath duration was 10 minutes.
The list of randomization with the sequence of bathing techniques to which each PTNB would be submitted was kept in a sealed envelope, accessed only by two nursing technicians, employees of the neonatal unit, previously trained in both types of bath.
The outcome variables analyzed were: HR (heart rate per minute - bpm), SpO2 (%) and SC level (nmol/L). HR and SpO2 were obtained by means of a pulse oximetry sensor and the multiparametric monitor display was filmed. Both were gauged immediately prior to undressing the PTNBs for bath, after resting for 10 minutes and between the 9th and 10th minute and the 19th and 20th minute after bath, with the RN dressed and resting in the crib. Filming was analyzed and the data were obtained by calculating the mean of the variation at the three one-minute intervals for measurement. Two saliva samples were collected with ophthalmic swab. The first one was obtained before the bath and the second one at the 20th minute after the bath. The laboratory analysis of SC was performed by the Elisa test.
Data were analyzed using the Fisher's test, paired Student's t-test, repeated measures ANOVA and mixed effect model. For the data loss of a subject who participated only in the first phase of the study (conventional bath) and did not participate in the second phase due to hospital transfer, the Intention-to-treat analysis was used, considering the worst outcome of the SB group variables.
The research project was approved by the Institutional Research Ethics Committees; proposer (No. 351,497) and co-participant (No. 601,951-0); and was registered in the Brazilian Registry of Clinical Trials (UTN: U1111-1151-5469). A written consent was obtained from those responsible, without any refusal.
The project was funded by the Foundation for Research Support of the State of São Paulo (case 2013/23884-1).
RESULTS
The study included 15 PTNBs that met the eligibility criteria and whose parents authorized participation. The two stages of the 14 PTNBs were completed, as there was a hospital transfer loss that completed only the first step, that is, it was only exposed to CB.
Figure 1 -- Flowchart of newborns who participated in the study. São Paulo, 2014
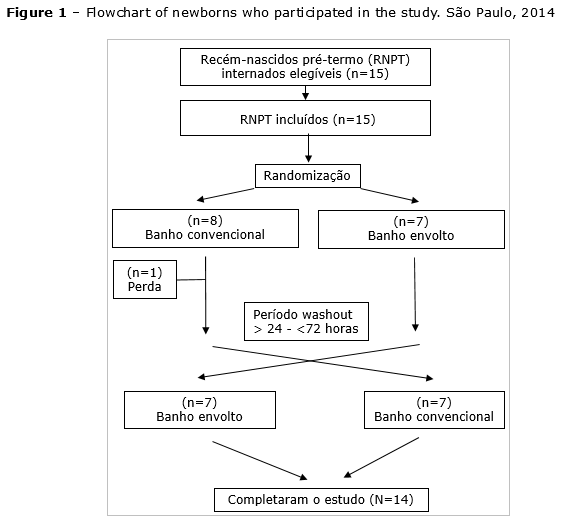
The majority of preterm infants were born vaginally (n=11, 73.3%) and were female (n=8, 53.3%). The calculated mean weight was 2.169 (±484.00) grams. The main hospitalization diagnoses were: low birth weight, respiratory discomfort and infection. The minimum and maximum APGAR scores at the 1st and 5th minutes of life were, respectively, 4 and 10 and 8 and 10. The mean gestational age was 34.21 (±1.730) weeks.
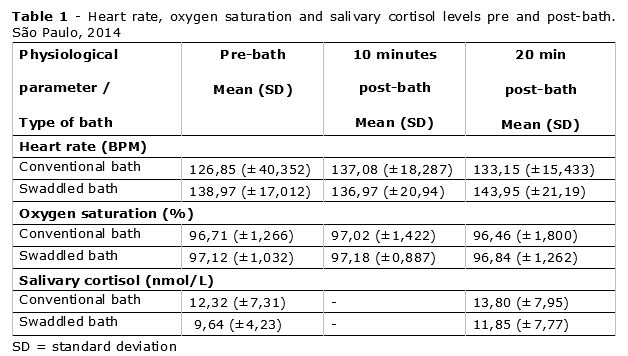
The mean HR of the SB group was significantly higher before bathing (p=0.013). There was no significant increase in HR over time (p=0.406) for both bath types and there was no statistical difference in HR variation between bath types (p=0,070).
In relation to the SpO2 values, there was no significant statistical difference in the mean values of this value before bath between bath types (p=0.428), without significant differences in the three measurement times (p=0,237) and SpO2 mean values were iqual for both types of bath (p=0,848).
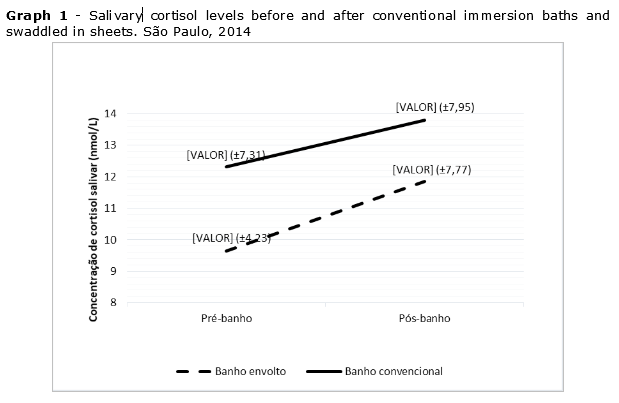
Regarding SC results, BCNB infants had significantly higher pre and post-bath mean values than those of SB (p=0.016). The SC of the SB group had an increase of 2,21 nmol/L (22.92%), while in the CB it was 1,48 nmol/L (12.01%). This increase was the same for both groups (p=0,729).
The analyzed results showed no differences in physiological and hormonal biomarkers indicative of stress in the immersion bath, regardless of the technique employed.
DISCUSSION
The present study aimed at evaluating the variations in HR, SpO2 and SC concentration, stress response indicators to the immersion bath by the conventional method and with the PTNB swaddled in sheets, a procedure recommended by the Ministry of Health for PTNBs and with low weight.
The results showed that there were no statistical and clinical differences in the physiological and hormonal responses analyzed. The only data that presented difference between the types of bath was in relation to the pre-bath HR, which in the SB group was statistically larger; however, such a difference is irrelevant from the clinical point of view. This difference may have occurred because NBs were more manipulated by being swaddled in the sheet before being immersed in the bath water.
The manipulations of the PTNBs trigger patterns of stress responses that are indicative of their ability to cope with environmental stimuli, which can be evaluated through autonomic and behavioral response parameters, and evidences point to a significant increase during the care given(17), including the immersion bath, considered one of the procedures that most require manipulation of the caregiver.
Pre- and post- quasi-experimental study evaluated the effect of hydrokinesiotherapy on the outcomes HR, SpO2, SC, respiratory rate, and pain score in the Neonatal Infant Pain Scale (NIPS) in 15 PTNBs hospitalized at the NICU weighing more than 1000 grams. The vital parameters were evaluated five minutes before the immersion bath in bucket and immediately after. There was a significant reduction in the mean values pre-compared with post-hydrotherapy of the HR (163.4 BPM versus 150.4, p=0.003), SpO2 increase (97% versus 99%, p=0.002), SC reduction (p=0.004), decreased respiratory rate (55.2 versus 49.3, p=0.004), and reduced NIPS pain score from 0.53 to 0 (p=0,087). Hydrokinesiotherapy included placing the infused NB in a flexed position in a bucket with 37°C water and passive mobilizations of the upper and lower limbs, overall stretching, trunk rotation and proprioceptive and vestibular tactile stimulation, ending with the baby in fetal position. The therapy lasted 10 minutes(18). These results showed similarity with the findings of the present study, with the exception of SC that was contrary to those found in this study.
The reduction of SC levels is associated with the positioning of the NB(19) as described in the literature. NB's positioning during the exposure to Hydrokinesiotherapy and the way of manipulating the NB may explain the difference found in the mean values of SC, suggesting that the procedures adopted in the body hygiene should consider the quality and quantity of stimuli caused in the PTNB, as well as the positioning in the bathtub.
With regard to SC, the results indicate that exposure to SB had a higher increase in the mean of the hormonal levels after bathing when compared to CB, although this statistical difference was not significant, considering the small sample of this pilot study. The difference in the values of the pre-bath mean of the CB compared to the pre-bath means of the SB was a finding that drew attention, since the SC collection procedure was performed in a standardized way with all the apparently calm, resting, dressed, and covered in the cradle, following the standard procedure described in the method. The PTNB were not manipulated or stimulated during the 10-minute interval before removing the clothes and initiating the baths.
It is worth emphasizing that in the cross-over trials, all the subjects of the study are exposed to both types of intervention. In the case of this study, CB and SB, and the result to be considered are the difference between the means of pre- and post-bath SC concentration that showed no difference between the groups. In any case, the results confirm that the immersion bath procedure is a stressor factor for PTNBs, because the SC levels remained higher in relation to pre-bath values, even after 20 minutes of the end of the procedure, although the pre and post differences were not statistically significant for the two types of bath.
The literature points out that it is difficult to collect the saliva sample for SC examination because of the volume required for analysis(20); this was not verified in the present study because of the innovative technique used in the collection (use of ophthalmic swab and time of stay of the swab in the mouth of the NB -- 10 minutes) to obtain the minimum volume required (1mL) for laboratory analysis. The literature reports failure to collect saliva samples ranging from 1% to 46%(2,20) due to insufficient volume of saliva in PTNBs. These data alerted the study team about the cost of losses in the planning phase of the study and led to the search for material (swab) that allowed high absorption and safety for the collection of biological material, as well as to search the literature for the ideal time of maintenance of the swab in the mouth of the newborn to obtain the necessary volume of saliva. These strategies were successful in obtaining and analyzing salivary cortisol without any loss.
CONCLUSION
There were no significant statistical and clinical differences in the pre and post-bath values among the PTNB groups studied in relation to HR, SpO2 and SC, although the latter was increased for both groups regardless of the technique used, thus concluding that there is no difference between the bathing techniques employed. Because it is a pilot study, it is necessary to increase the size of the sample in order to reach definitive conclusions.
REFERENCES
-
Santos J, Pearce SE, Stroustrup A. Impact of hospital-based environmental exposures on neurodevelopmental outcomes of preterm infants. Curr Opin Pediatr. 2015;27(2):254-60.
-
Mörelius E, He H-G, Shorey S. Salivary cortisol reactivity in preterm infants in neonatal intensive care: an integrative review. Bielajew C, Mileva G, eds. Int J Environ Res Public Health. 2016;13(3):337.
-
Lyngstad LT, Tandberg BS, Storm H, Ekeberg BL, Moen A. Does skin-to-skin contact reduce stress during diaper change in preterm infants? Early Hum Dev. 2014 Apr;90(4):169-72.
-
American Heart Association. Highlights of the 2015 American Heart Association. Guidelines Update for CPR and ECC. Am Heart Assoc, 2015.
-
Thiriez G, Mougey C, Vermeylen D, Wermenbol V, Lanquart J, Lin SJ, et al. Altered autonomic control in preterm newborns with impaired neurological outcomes. Clin Auton Res. 2015;25(4):233-42.
-
Peng NH, Bachman J, Chen CH, Huang LC, Lin HC, Li TC. Energy expenditure in preterm infants during periods of environmental stress in the neonatal intensive care unit. Jpn J Nurs Sci. 2014;11(4):241-7.
-
Smith SL, Haley S, Slater H, Moyer-Mileur LJ. Heart rate variability during caregiving and sleep after massage therapy in preterm infants. Early Hum Dev. 2013;89(8):525-529.
-
Cabral D. M., Antonini S. R. R., Custódio R. J., Martinelli C. E., Jr., Da Silva C. A. B. Measurement of salivary cortisol as a marker of stress in newborns in a neonatal intensive care unit. Horm Res Paediatr. 2013;79(6):373--378.
-
Brasil. Ministério da Saúde. Atenção humanizada ao recém-nascido de baixo peso: Método Canguru. 2ªed. Brasília: Editora do Ministério da Saúde, 2011.
-
Dezhdar S, Jahanpour F, Firouz Bakht S, Ostovar A. The effects of Kangaroo Mother Care and swaddling on venipuncture pain in premature neonates: a randomized clinical trial. Iran Red Crescent Med J. 2016;18(4):e29649.
-
Ho LP, Ho SS, Leung DY, So WK, Chan CW. A feasibility and efficacy randomised controlled trial of swaddling for controlling procedural pain in preterm infants. J Clin Nurs. 2016 Feb;25(3-4):472-82.
-
Abdeyazdan Z, Mohammadian-Ghahfarokhi M, Ghazavi Z, Mohammadizadeh M. Effects of nesting and swaddling on the sleep duration of premature infants hospitalized in neonatal intensive care units. Iran J Nurs Midwifery Res. 2016;21(5):552-556.
-
Pease AS, Fleming PJ, Hauck FR, Moon RY, Horne RS, L'Hoir MP, et al. Swaddling and the risk of Sudden Infant Death Syndrome: a meta-analysis. Pediatrics. 2016 Jun;137(6): e20153275.
-
Antonov NK, Ruzal-Shapiro CB, Morel KD, Millar WS, Kashyap S, Lauren CT, et al. Feed and wrap MRI technique in infants. Clin Pediatr (Phila). 2017;56(12):1095-1103.
-
Edraki M, Paran M, Montaseri S, Razavi Nejad M, Montaseri Z. Comparing the effects of swaddled and conventional bathing methods on body temperature and crying duration in premature infants: a randomized clinical trial. J Caring Sci. 2014;3(2):83-91.
-
Wellek S, Blettner M. On the proper use of the crossover design in clinical trials: Part 18 of a series on evaluation of scientific publications. Dtsch Arztebl Int. 2012;109(15):276-281.
-
Zeiner V, Storm H, Doheny KK. Preterm infants' behaviors and skin conductance responses to nurse handling in the NIC. J Matern Fetal Neonatal Med. 2016; 29(15):2530-2535.
-
Tobinaga WCO, Marinho CL, Abelenda VLB, Sá PM, Lopes AJ. Short-term effects of hydrokinesiotherapy in hospitalized preterm newborns. Rehabil Res Pract. 2016;2016:1-8.
-
Cândia MF, Osaku EF, Leite MA, et al. Influence of prone positioning on premature newborn infant stress assessed by means of salivary cortisol measurement: pilot study. Rev Bras Ter Intensiva. 2014;26(2):169-175.
-
Maas C, Ringwald C, Weber K, Engel C, Poets CF, Binder G, et al. Relationship of salivary and plasma cortisol levels in preterm infants: results of a prospective observational study and systematic review of the literature. Neonatology. 2014; 105(4):312-318.
Authors' contribution to research:
Patrícia de Freitas -- Performed the data collection, database, analysis, discussion, and bibliographic search;
Amélia Fumiko Kimura -- Participated in the data analysis and discussion.
All authors participated in the phases of this publication in one or more of the following steps, in according to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the version submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 08/01/2018
Revised: 09/17/2018
Approved: 01/10/2018