Validation of an instrument for the history of maternal and child nursing using Horta: a methodological study
Viviane Saraiva de Almeida1, Danielle Lemos Querido1, Ana Paula Vieira dos Santos Esteves1, Priscilla dos Santos Vigo1, Rita Bernardete Ribeiro Guérios Bornia1, Juliana Melo Jennings1
1Maternity-School of Federal University of Rio de Janeiro
ABSTRACT
Aim: to elaborate an instrument for the nursing history stage focused on maternal and child health service. Method: methodological study, with validation of content of an instrument for the nursing history for maternal and child service, based on the reference of Wanda Horta. Results: the form contains the following information: identification; vital signs, blood glucose and anthropometric data; clinical data and laboratory tests; interview and observation of the patient; physical examination and basic human needs; printouts. Other needs related to the area (reproduction/growth and development) not provided for by the underlying theory that gave grounds for the study were added. There was an overall content validity index of 0.81 for clarity, 0.85 for relevance, 0.92 for comprehensiveness, and 0.81 for organization. Conclusion: instrument built and validated based on Wanda Horta's theory, aimed at the maternal and child clientele, providing an important instrument to document the first stage of the nursing process.
Descriptors: Nursing Care; Nursing Theory; Maternal-Child Nursing; Pregnant Women; Postpartum Period.
INTRODUCTION
The Nursing Process (NP) is a method used to implant, in professional practice, a nursing theory. For this, it is necessary to use a scientific method for the applicability of scientific concepts(1). In Brazil, the most well-known and followed model for the implementation of the NP was the one proposed in 1979 by Wanda Horta, who describes the nursing history as the first stage of the NP(2).
Nursing theory should give support so that the instrument for recording data collection (nursing history) can systematize concepts, allowing the whole process to be viable for efficient and effective decision making(1,3).
The conceptual model chosen to base the instrument constructed in this study was Wanda Horta's basic human needs (BHN), since it is the most commonly used in the maternal and child area since the 1970s(4-5), providing a theoretical basis best suited to the specific needs of the clientele served.
This instrument based on this theory, built with scientific evidence and contributions of expertise, allows observing the specificities of hospitalization, with the possibility of nurses envisioning the perspective of an extended care that transcends the biological, technological and automatic dimension(6).
The justification of this study is based on the understanding that the NP is a requirement of the Conselho Federal de Enfermagem (COFEN - Federal Nursing Council) in the care practices, demanding that the nursing services invest in the construction and validation of instruments that meet their peculiarities, so it can guide and standardize the operationalization of this process(7).
Physical examination and anamnesis are fundamental to support the next phases of the NP(8), adding quality to care, visibility and recognition to Nursing, as well as supporting the reflection and evaluation of care practices(9).
In the context of improving the quality of care provided, maternal and child clients deserve special attention, since Brazil presents serious indicators of maternal mortality due to preventable causes. In an attempt to reverse this situation, the United Nations (UN) has established the Millennium Development Goals(10) for eighteen years, 10 which have not been fully achieved, including those related to the promotion of maternal and newborn health. Thus, in 2015, new priorities were established by the UN, known as Sustainable Development Goals (SDGs). One of the goals of the third SDG is to reduce the overall maternal mortality rate and eliminate the preventable deaths of newborns(11) through actions that improve the quality of prenatal, delivery and postpartum care(10).
Based on this assumption, in order to produce a humanized and quality nursing care in maternal and child health, it is necessary to organize the work in order to allow nurses to know the profile of the clientele served and the human and social needs affected, whether in the prenatal period, labor and delivery or puerperium(8). In this perspective, the nursing history step should include the collection of quality information that is relevant to the context, since an inadequate or inadequate evaluation may lead to an inappropriate diagnosis and/or prescription and to an improper judgment of the state of health of the clientele(12). On the other hand, a well-filled history and with pertinent information will support more effective nursing interventions and the improvement of the quality of care provided to the mother and child clientele.
Given the importance of this phase within the NP, a survey of the documents used by the nursing team was carried out in the setting of this study. It was identified that there were no instruments that would support the phase of data collection. In the scientific databases there were also no studies that contemplated the construction of nursing histories in the maternal and child area.
In response to this challenge, the present study had as objective: to elaborate an instrument for the nursing history stage focused on maternal and child service.
METHODS
The research was developed as a cut of the institutional project called "Systematization of nursing care: the challenge of implementing the methodology in a maternal and child service "already appreciated by the Ethics and Research Council of the institution, where it followed the precepts of Resolution 466/2012 and was approved under the opinion No. 1,165,734 in July 2015. The study was developed from the following steps:
Preliminary stage: literature review
In order to identify studies related to the maternal-infant area and that used the BHN theory of Wanda Horta in the construction of the nursing history, a bibliographic research was performed in the Virtual Health Library through the terms "history of nursing" and "Horta ". This search resulted in 17 articles, of which none were related to the maternal and child area. A second round of searches was carried out using the terms "nursing history" and "nursing care systematization" with the same filter used in the first search: complete articles published in Portuguese, English or Spanish. In this new search, the system identified 21 articles, of which only one was related to the maternal-infant area, although the focus was exclusively the obstetric area. Notwithstanding these results, the applicability of this step was important, since the identification of this last article(13) supported, initially, the construction of the instrument of data collection of the present study.
First step: the construction of the data collection instrument
Based on Wanda Horta's theory, the instrument for collecting data to collect the patient's history was designed to address psychobiological, psycho-spiritual and psychosocial needs, based on the three levels of João Mohana(2):
- Psychobiological: oxygenation; hydration; nutrition; elimination; sleep and rest; exercises and physical activities; sexuality; shelter; body mechanics; cutaneous and mucosal integrity; physical integrity; regulation: thermal, hormonal, neurological, hydrosaline, electrolytic, immunological, cell growth, vascular; locomotion; perception: olfactory, visual, auditory, tactile, gustatory, painful; environment; and therapeutic.
- Psychosocial: love; freedom; Communication; creativity; learning; gregarious; recreation; leisure; space; orientation in time and space; acceptance; self-realization; self-esteem; participation; self-image; and attention.
- Psycho-spiritual: religious or theological; ethics or philosophy of life.
Second step: the validation of the data collection instrument
The validation of content and appearance of the instrument elaborated for maternal and child service was carried out, based on the theoretical framework of Wanda Horta.
Content validation determines whether the content of a measuring instrument effectively explores the requirements for measuring a particular phenomenon to be investigated. The Appearance Validation strategy that provides judgment on the suitability of items was also used(14). Judges should initially assess the instrument as a whole, determining its scope, and analyze the individual items for clarity and relevance. There is no consensus on the minimum or maximum number of judges, ranging from five to twenty subjects(15).
The letter of invitation, the data collection instrument and the manual with the criteria for evaluation were sent by e-mail along with a written informed consent form to 16 judges selected via Lattes platform, based on the following criteria: the body of judges should be composed of, at least, 50% of nurses graduated with stricto sensu, and the others should have a specialization degree in the maternal and child area; professional experience of, at least, five years of care practice in the area. Of the judges selected and invited, only 6 returned the instruments filled, all with expertise in the area of Nursing Assistance Systematization (NAS). Within this group, three were specialists, two masters and one doctor in the maternal-child area. Responses regarding the evaluation of the data collection instrument were considered as a positive consent to participate in the research. The content and appearance evaluation stage occurred in August and September 2015, from a Likert scale with a score of one to four (1 = disagree; 2 = partially disagree – this item needs major revision to be representative; 3 = partially agree – this item needs small revision to be representative; 4 = fully agree). Items scoring "1" or "2" were deleted.
The content validity index (CVI) followed from three approaches: S-CVI/Ave (CVI mean for each scale item), S-CVI/UA (proportion of items on a scale that achieves a relevance rating of 3 or 4 for all judges); and I-CVI (calculated as the number of judges who give a rating of 3 or 4 for the item, divided by the total number of experts). The content validation index of more than 0.80 was considered relevant(16).
For the apparent validation phase, the aspects clarity and understanding and pertinence of the instrument related to the maternal and child area in accordance with the BHN were considered. At the end of the instrument there was still a space for suggestions for adding, withdrawing or modifying items of the instrument.
The judges' answers were tabulated and analyzed in the Excel 2003 program. Items that did not reach the established index were modified and returned to the judges for a new round, and then those who did not meet the target set in the last round were removed from the form. Three rounds were necessary to obtain indices equal to or greater than 0.80 established for the study.
A pilot test was carried out and the form was put into use in the Obstetric Emergency sector, the study scenario, from November to December 2015, so that the nurses of that sector could test the instrument validated.
The inclusion of lay people related to the study would ensure the correction of phrases and terms that are not very clear(15).
RESULTS
First step: the construction of the data collection instrument
The data collection form (figure 1), nursing history, was constructed from the grouping of related information, in order to organize the collected information and the clinical reasoning of the nurse, without losing sight of the support of the theoretical reference of Wanda Horta. The instrument makes it possible to identify problems and evaluate the maternal and child clientele, trying to detail, to the maximum, all the information necessary to identify their needs. In addition, it also had as its aim the objectivity and focus on the possible problems of the maternal and child clientele, with the intention of not recording irrelevant information, which could divert the clinical reasoning of the nurse to disposable information or of little relevance, besides wasting both interviewee and interviewer time.
It was structured as a systematized guide so that data collection culminated with the establishment of nursing diagnoses and interventions, with the entire itinerary for the adequate implementation of NP and better organization of the data of the first stage.
The roadmap was elaborated with the following domains: identification; vital signs, blood glucose and anthropometric data; clinical data and laboratory tests; interview and observation of the patient (data of current hospitalization, current gestation and breastfeeding, if applicable); physical examination and basic human needs (psychobiological, psychosocial and psycho-spiritual needs); impressions or intercurrences. The following is a detail of the domains of this instrument:
-
Identification - the first part of the instrument is constituted by the identification of the patient that provides elements for the individualization of care and some sociodemographic data that situate the nurse in relation to the clientele served. This phase includes all the necessary data to begin the interview with the patient, besides allowing the host with risk classification, taking into account the clinical evaluation by priority (more severe cases).
-
Vital signs, blood glucose and anthropometric data - second part, in which the vital signs (axillary temperature, apical pulse, breathing, blood pressure, pain scale) are presented; peripheral blood glucose; weight and height of the patient.
-
Clinical data and laboratory tests – in the third part results of the laboratory tests are included: stool, urine, blood count, among others, besides other clinical data of interest of the nurse.
-
Interview and patient observation – the fourth part called the interview begins with data from the current hospitalization, defining the profile of the woman as a puerperal or pregnant woman, basic pathology and other relevant items. After completing data related to the current hospitalization, the interview takes place according to the patient's condition. If you are pregnant, you will fill in the following items: "Current gestation data"; "Previous breastfeeding data" (if you have previous experiences with breastfeeding). In the case of postpartum women, they will respond to the items: "previous breastfeeding data" and "current breastfeeding data", with the identification of possible risk factors and nursing problems that may support nursing interventions related to breastfeeding.
-
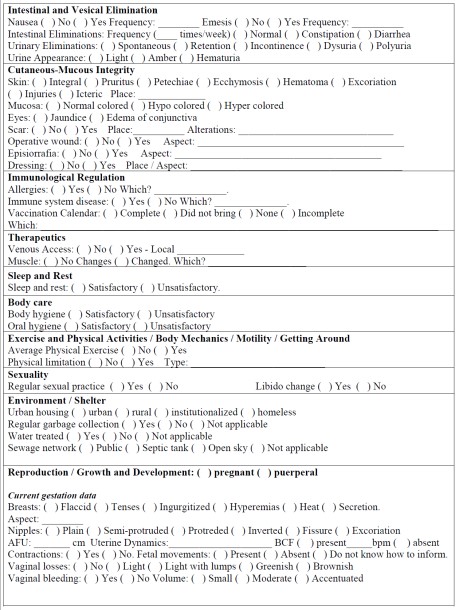
Physical examination and basic human needs – the fifth part groups up the items related to BHNs and those that have been grouped into psychobiological, psychosocial and psycho-spiritual needs in accordance with the emerging concepts of Wanda Horta's theory, adjusted to the problems commonly found in the maternal and child clientele, as can be seen below:
-
Psychobiological: neurological regulation; oxygenation; vascular regulation; thermal regulation; olfactory perception, auditory visual, tactile, gustatory, painful; nutrition; hydration; hydrosaline and electrolytic regulation; intestinal and bladder elimination; cutaneous-mucosal integrity, immunological regulation; therapy; sleep and rest; body care; exercise and physical activities; body mechanics; motility; locomotion; sexuality; environment and shelter; reproduction/growth and development.
-
Psychosocial: neurological regulation; oxygenation; vascular regulation; thermal regulation; olfactory perception, auditory visual, tactile, gustatory, painful; nutrition; hydration; hydrosaline and electrolytic regulation; intestinal and bladder elimination; cutaneous-mucosal integrity, immunological regulation; therapy; sleep and rest; body care; exercise and physical activities; body mechanics; motility; locomotion; sexuality; environment and shelter; reproduction/growth and development.
-
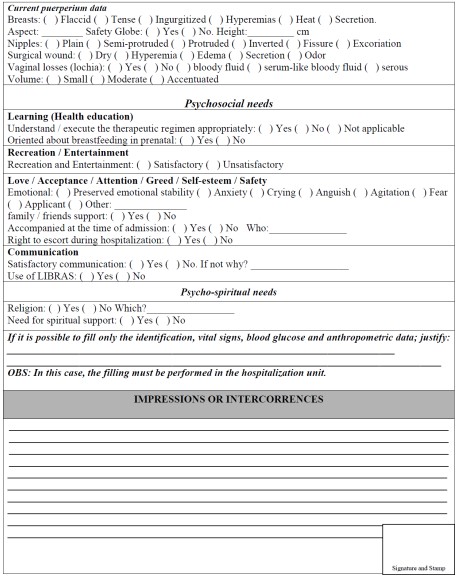
Psychosocial: learning; recreation and leisure; love; acceptance; attention; gregariousness; self-esteem; safety; Communication.
-
Psycho-spiritual: religion.
Second step: the validation of the data collection instrument
Table 1 shows the results of the judges' evaluation for each domain identified after the rounds. I-CVI was verified for clarity, pertinence, comprehensiveness and organization ranging from 0.83 to 1. It was also identified the global CVI (S-CVI/Ave, S-CVI/UA) that was 0.81 for clarity, 0.85 for relevance, 0.92 for comprehensiveness and 0.81 for organization. All items with I-CVI lower than 0.80 were withdrawn from the instrument.
Table 1 – Distribution of Content Validity Indices. Rio de Janeiro, RJ, 2016
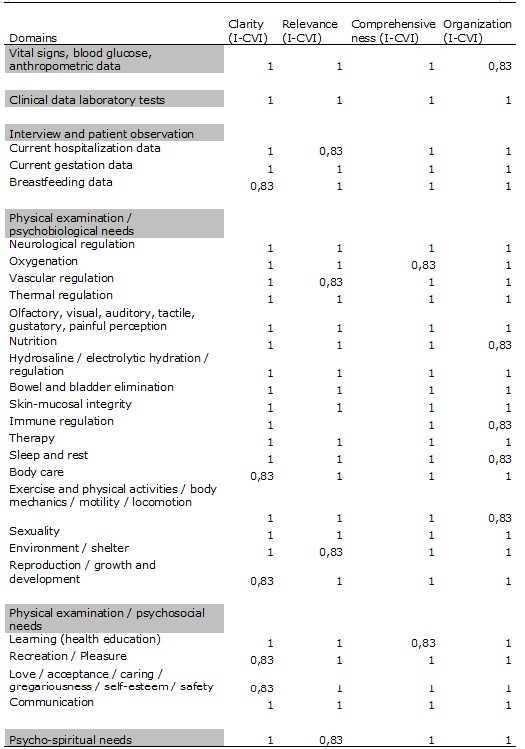
Source: Authors
Some items were excluded from the form by the researchers: the item "eyes" was removed from the need for visual perception, section Physical Exam/basic human needs, since visual acuity is already contemplated in this section; the "visual pain scale" was excluded from the form, leaving only the result of the pain assessment in the Vital Signs section, blood glucose and anthropometric data in order to improve the form space. As a suggestion, the pain scale was fixed at the nursing consultation table.
After 3 rounds of evaluation of the judges, the included items were: "prenatal site" in the Identification section; "pain" was included in the Vital Signs section; "LMP" (last menstruation period) and "USG" (ultrasonography) were included to determine which method was used to calculate the current gestational age; "desired gestation" was included in current gestation data in the Interview and Observation section of the patient; "Peripheral perfusion" in the need for vascular regulation; "Did not bring" and "does not have" were included for immunization schedule in need of immunological regulation, Physical examination/basic human needs section.
The reformulated items, on the other hand, that were related to the human needs of reproduction and growth/development section of Physical Exam/basic human needs were reorganized to facilitate understanding and objectivity. The information was subdivided into "current gestation data" and "current puerperium data".
It was suggested that the section Vital Signs, glycemia and anthropometric data be allocated at the beginning of the form because they are important data and may somehow define the need for immediate nursing care or provide data for a drug therapy. The importance of contemplating breastfeeding data on the form was emphasized, due to the specificity of the clientele attended at the institution. After all these steps, the following form was obtained (figure 1):
Figure 1 – Nursing history for maternal and child clientele. RJ, Rio de janeiro, 2016
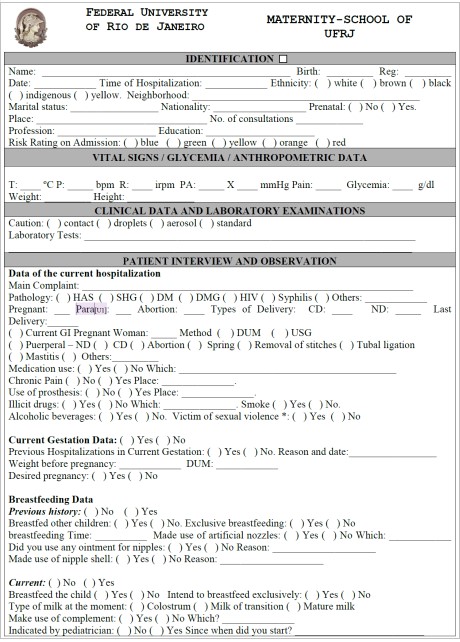

Source: Authors, 2016.
DISCUSSION
The collection and organization of the data in the nursing history will enable an important structure for the nurse to correctly determine diagnoses, prescription and nursing evolutions(1).
All subsequent NP steps are linked to the data collected. In this sense, it is of paramount importance that these data be complete and organized, enabling the nurse to evaluate the patient's responses to adverse conditions(17).
Patient health data should be grouped together with related information, focusing on human response and functioning patterns. This grouping is one of the bases of critical thinking that favors nurses to have an objective view of health problems, making their judgment and inferences correct. The instrument should be designed to contain relevant and holistic information, taking into account the biological, social, psychological and spiritual spheres, according to the nursing theory used(1).
The indispensable minimum items to contemplate an adequate nursing history are: identification data; perception and expectations of the patient (previous experiences, problems, what is known about the disease, among others); basic needs (nutrition, hydration, elimination, sleep and rest, body care, recreation, spiritual); physical exam; problems or patterns of communication(2).
Patient identification data should be as complete as possible, including: full name, ward, bed, record, sex, age, marital status, nationality, occupation, educational level and admission date(2).
It is necessary to promote the understanding, as accurately as possible, of the history of the patient's current illness. When recalling the events related to health conditions, the patient should be the protagonist and the more he reports on his own health more reliable it will be(18).
The phases prior to the physical examination are also called by some anamnesis authors. The nursing history includes the phases of anamnesis and the physical examination. Anamnesis is defined as the first phase of the process, and it may contain subjective, objective, historical and current data. These can be obtained through: interview, observation, results of diagnostic tests and review of medical records and collaboration of other professionals. It should provide a complete picture of the history of the person's current and past pathological disease(18).
However, as in all NP, this systematization is only didactic, as the phases overlap and, in this sense, the evaluation of basic human needs occurs simultaneously to physical examination. The physical examination is a valuable tool for care, since it allows nurses to validate the findings of the anamnesis, identify problems, define nursing diagnosis, plan and program nursing actions and follow the evolution of the patient(18).
As a relevant step, we look for abnormalities, objective and verifiable signs that may contain information on significant health problems for the identification of nursing diagnoses, essential support for care planning(18).
In this study, it was observed that, in order for the form to be objective and its construction relevant, with data covering the maternal-infant area, the incorporation of other psychobiological needs not contemplated by Wanda Horta was necessary. They were: needs of reproduction and growth/development already studied and validated by other authors, who also took as base the BHN of Wanda Horta, as the nomenclature CIPESC® of Curitiba(19).
It was also evident that the incorporation of all the human needs listed by Wanda Horta would not be objective and focal to the construction of history in the area of study. In this way, the needs that best fit the mother-child clientele were selected. This method was also used by other authors in the construction of nomenclatures in the area of human needs, in the case of CIPESC® of Curitiba(19). This classification comprises 25 needs, ten of which are foreseen by Horta(2), thirteen indicated by other authors(20), and two new needs that did not appear in previous nomenclatures, namely: reproduction and growth/development related to the psychobiological needs of the individual.
It should be mentioned that the CIPESC®(19) nomenclature did not list the needs, predicted by Horta(2), for body regulation, except for vascular and immunological regulation, which are basal for collective health practice focusing on the consultations directed to pregnant women and children. The basic human needs of physical integrity, safety and environment, shelter, mechanics, body, locomotion, leisure, love and acceptance, communication, creativity, self-realization and space are not included in the nomenclature CIPESC®.
The validation phase of the instrument by judges and the suggestions made by them was important in that it was verified that the instrument included the most relevant data related to Wanda Horta's Theory, focusing on the maternal and child area. It was also at this stage that specific needs related to the area of study (reproduction/growth and development), not provided for in the basic theory, were added, and that alternatives were created to support the information needed to attend to the aforementioned psychobiological needs.
It should be emphasized that, even though it has been validated by experts in the field, the instrument presents itself as a technology that does not rule out the capacity for critical analysis and judgment of nurses when performing NP. The instrument aims to facilitate the data collection phase and the consequent identification of nursing problems and diagnoses, fulfilling its role in the first stage of the nursing process.
CONCLUSION
The nursing history is applied in the initial phase of the NP, because it is precisely in this first approach with the patient that nurses must become familiar with patients' history and seek to establish mutual trust that facilitates the establishment of the link. Once established this link, associated to an anamnesis and a well structured physical examination, it is possible to identify the biopsychosocial and spiritual changes of the patient. Given this recognition, the NP can follow, by defining nursing diagnoses, goals and/or nursing prescriptions, through registries, with the aim of placing the nurse as an active agent for the development of their care. The search for literature review to support scientific knowledge was extremely important to solidify the choice of Wanda Horta's Theory, understanding that its central concepts could be applied in our practice.
The validation of the instrument by judges helped to adapt it to the theory adopted and provided a method to the stage of the nursing history envisaged in the NP, which can be adapted according to the characteristics of other services and serve as a support for the direction of related studies to the NP in the maternal and child area. The implanted instrument may still undergo changes at the suggestion of the professionals who use it; however, the evaluation has been positive since the instrument facilitates the annotation of care data, corroborating to an increase in the quality of nursing records, and provides attributes for the recognition and appreciation of nurses in their care practice.
REFERENCES
- Tannure MC, Pinheiro AM. SAE: Sistematização da assistência de enfermagem: guia prático. Rio de Janeiro: Guanabara Koogan; 2011.
- Horta WA. Processo de Enfermagem. São Paulo: EPU; 1979.
- Domingos CS, Moura PC, Braga LM, Rodrigues NV, Correia MDL, Carvalho AMP. Construction and Validation of the Historical Contents of Nursing Guided by Orem Reference. Rev Min Enferm. [internet]. 2015 [cited 2016 jan 5];19(2):165-175. Avaliable from: http://www.reme.org.br/artigo/detalhes/1013
- Lucena ICD, Barreira IA. Revista enfermagem em novas dimensões: wanda horta e sua contribuição para a construção de um novo saber da enfermagem (1975-1979). Texto contexto - enferm. [Internet]. 2011 Sep [cited 2018 Feb 21]; 20( 3 ): 534-540. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-07072011000300015&lng=en. http://dx.doi.org/10.1590/S0104-07072011000300015.
- Medeiros AL, Santos SR, Cabral RWL, Silva JPG, Nascimento NM. Assessing nursing diagnoses and interventions in labour and high-risk pregnancies. Rev. Gaúcha Enferm. [Internet]. 2016 [cited 2018 Feb 22]; 37(3): e55316. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1983-14472016000300409&lng=en. Epub Sep 29, 2016. http://dx.doi.org/10.1590/1983-1447.2016.03.55316.
- Santos DMA, Sousa FGM, Paiva MVS, Santos AT. Development and implementation of a nursing patient history in Pediatric Intensive Care. Acta paul. enferm. [Internet]. 2016 Apr [cited 2018 Feb 21]; 29(2): 136-145. Available from: http://www.scielo.br/readcube/epdf.php?doi=10.1590/1982-0194201600020&pid=S0103-21002016000200136&pdf_path=ape/v29n2/en_1982-0194-ape-29-02-0136.pdf&lang=en
- Silva EGC, Oliveira VC, Neves GBC, Guimarães TMR. Nurses' knowledge about Nursing Care Systematization: from theory to practice. Rev. esc. enferm. USP [Internet]. 2011 Dec [cited 2018 Feb 23]; 45(6): 1380-1386. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342011000600015&lng=en. http://dx.doi.org/10.1590/S0080-62342011000600015
- Garcia TR. Classificação Internacional para Prática da Enfermagem - CIPE®: aplicação à realidade brasileira. Porto Alegre: Artmed; 2015.
- Trindade LR, Silveira A, Ferreira AM, Ferreira GL. Compreensão do processo de enfermagem por enfermeiros de um hospital geral do sul do Brasil. Rev Enferm UFSM. 2015; 5(2): 267-77
- World Health Organization (WHO). Millennium Development Goals. New YorK: WHO; 2000. Available from: http://www.un.org/millenniumgoals/maternal.shtml
- World Health Organization (WHO). Sustainable Development Goals. New YorK: WHO; 2015. Available from: http://www.un.org/sustainabledevelopment/sustainable-development-goals/
- Tavares TS, Castro AS, Figueiredo ARFF, Reis DC. Avaliação da implantação da sistematização da assistência de enfermagem em uma unidade pediátrica. Rev Min Enferm [Internet] 2013 Abr-Jun [cited 2018 Feb 22]; 17(2):287-295. Available from: http://www.reme.org.br/artigo/detalhes/650
- Santos RB, Ramos KS. Sistematização da assistência de enfermagem em Centro Obstétrico. Rev. bras. enferm. [Internet]. 2012 Feb [cited 2018 Feb 23]; 65( 1 ): 13-18. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672012000100002&lng=en. http://dx.doi.org/10.1590/S0034-71672012000100002
- Bellucci Júnior JA, Matsuda LM. Construção e validação de instrumento para avaliação do Acolhimento com Classificação de Risco. Rev. bras. enferm. [Internet]. 2012 Oct [cited 2018 Feb 22]; 65(5): 751-757. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672012000500006&lng=en. http://dx.doi.org/10.1590/S0034-71672012000500006.
- Alexandre NMC, Coluci MZO. Content validity in the development and adaptation processes of measurement instruments. Ciênc. Saúde Colet. [internet]. 2011 [cited 2016 jan 5]; 16(7):3061-3068. Avaliable from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232011000800006&lng=pt. http://dx.doi.org/10.1590/S1413-81232011000800006
- Polit DF, Beck CT. The content validity index: are you sure you know what's being reported? Critique and recommendations. Res Nurs Health [Internet]. 2006 Oct [cited 2018 Feb 23]; 29(5):489-97. Available from: http://onlinelibrary.wiley.com/doi/10.1002/nur.20147/pdf
- Silva R, Pereira A, Ribeiro A, Marinho C, Carvalho I, Ribeiro R. Preparation of a critical patient data collection instrument: nursing record. Rev. Enferm UERJ [internet]. 2012 [cited 2016 Mar 16]; 20(2):267-73. Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/1552/2870
- Santos N, Veiga P, Andrade R. Importance of history and physical examination for the care of nurses. Rev. bras. enferm. [internet]. 2011 [cited 2016 Sep 21]; 64(2):355-358. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672011000200021&lng=en. http://dx.doi.org/10.1590/S0034-7167201100020002
- Albuquerque LM, Cubas MR. Cipescar é preciso!... In: Albuquerque LM, Cubas MR, organizadores. Cipescando em Curitiba: construção e implementação da Nomenclatura de Diagnósticos e Intervenções de Enfermagem na Rede Básica de Saúde. Curitiba: ABEn; 2005.
- Benedet SA, Bub MBC. Manual de Diagnóstico de Enfermagem: Uma Abordagem Baseada na Teoria das Necessidades Humanas Básicas e na Classificação Diagnóstica da NANDA. Florianópolis: Bernúcia; 1998.
All authors participated in the phases of this publication in one or more of the following steps, in according to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the version submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 10/06/2016 Revised: 02/15/2018 Approved: 02/19/2018