Empirical indicators of human needs affected in mobile prehospital care: a methodological research
Aline Cecilia Pizzolato1, Leila Maria Mansano Sarquis1, Maria Júlia Paes da Silva2, Maria de Fátima Mantovani1
1Federal University of Paraná
2University of São Paulo
ABSTRACT
Aim: identify and collectively select empirical indicators of Basic Human Needs (BHN) in the context of Mobile Prehospital Care (MPC). Method: This is a descriptive research of the methodological type, using a quantitative approach, carried out at the Mobile Emergency Care Service (SAMU), in Curitiba-PR-Brazil, between 2014 and 2015. It was developed in two stages: the first, through consultation in the scientific literature related to MPC and through consultation in the international protocols Advanced Cardiac Life Support (ACLS) and Prehospital Trauma Life Support (PHTLS); the second, through a questionnaire applied to the 34 nurses participating in the research. Results: 138 empirical indicators were obtained. Of these, 96 were considered relevant and, among these, the regrouping and reorganization were carried out, totaling 69 indicators. Conclusion: The identification of the empirical indicators allowed the selection of the most relevant signs and symptoms in the context of MPC.
Descriptors: Signs and Symptoms; Nursing Care; Nursing; Prehospital Care.
INTRODUCTION
In Brazil, the implantation of the Mobile Prehospital Care service (MPC) occurred in the early 1990s, and was called the Mobile Emergency Care Service (Serviço de Atendimento Móvel de Urgência – SAMU). According to the Ministry of Health(1), this service is characterized by the care that seeks to reach the victim early, after a health problem has occurred.
The nurse is part of the SAMU teams at Advanced Life Support Units (ALSU) and has the following competencies and duties: to provide more complex nursing care to serious and life-threatening patients; provide nursing care to the pregnant woman, the parturient and the newborn; participate in training and improvement programs for health personnel in emergencies; make quality control of the service in the aspects inherent to their profession; and know equipment(1).
It should be noted that the MPC presents some particularities and that the nurse's performance in this service requires scientific knowledge and the ability to make immediate decisions(1). In order to anchor the knowledge of professional teams in emergency care, there are internationally applicable universal protocols, such as Pre-Hospital Trauma Life Support (PHTLS)(2) and Advanced Cardiac Life Support (ACLS)(3), which standardize care for patients by means of a sequence of priorities. And to guide the professional practice of nurses, there are Conceptual Models of Nursing, which support the scientific action of nurses(4) in the quest for professional autonomy, with the specificity of Nursing knowledge, through their own knowledge(5).
The researcher(6) advocates the BHN Conceptual Model and considers BHNs to be interrelated and part of an indivisible whole of the human being, so that, when one manifests, they all suffer some degree of change. From this perspective, the priorities for nursing care in MPC have to be adjusted systematically. In this sense, it is essential to establish criteria to select the most relevant needs.
As a way of determining a nursing planning to attend the affected BHNs in the patients, it is necessary to have knowledge about the empirical indicators. Through the identification of these indicators, nurses recognize the health needs to plan the nursing care(7).
Empirical indicators are identified by the selection of terms that represent the focus of nursing care. That is, they are signs and symptoms that patients present in the context of MPC. In this sense, this research was based on the BHN(6) reformulated by the researchers(8) and the international protocols. It is understood that there is a similarity of the proposals of the two models: the PHTLS protocol(2); and the Conceptual Model of BHN(6), since in both there is the determination of a similar logic and priority sequence, considered important for the primary patient assessment in MPC.
Therefore, the identification of the most relevant signs and symptoms that affect the BHN in this service supports the conduction of the clinical reasoning of the nurse to perform the priority individualized and systematized care based on the nursing process. It also allows the nursing record, which should contain a summary of the data collected, diagnoses, interventions and nursing outcomes(9). However, in the application of the Nursing Process (NP) it is observed that the nurse finds difficulty in establishing the nursing diagnosis, since many are unaware of BHN and its symptoms(6).
Thus, it is perceived that the MPC nurse needs to know systematized evaluation methods to support the recognition of the signs, symptoms and BHN affected and to develop the appropriate nursing care planning and registration. The aim is to promote a balance of BHNs with scientific knowledge based on the analysis of the empirical indicators.
Thus, it is imperative for nursing care that nurses develop a critical thinking to make safe and priority decisions, based on scientific evidence.
In view of the above, this research aimed to identify and collectively select the empirical indicators of the BHN in the context of Mobile Prehospital Care.
METHOD
It is a descriptive research of the methodological type, with a quantitative approach, which allows the investigation of methods of obtaining and organizing data, from the elaboration, validation and evaluation of instruments and research techniques(10). It was developed in the Advanced Support Units (USA) of SAMU, of the Department of Urgency and Emergency (DUE), linked to the Municipal Health Secretariat (Secretaria Municipal de Saúde – SMS) of the Municipality of Curitiba (Prefeitura Municipal de Curitiba – PMC), state of Paraná, from August 2014 to January 2015.
This article was elaborated from the first stages of the research, developed in the master's dissertation, presented to the Graduate Program in Nursing - Professional Master's Degree. To reach the proposed objectives, it was developed in two stages.
In the first step, the identification of the empirical indicators of the BHNs was carried out through consultation in the scientific literature on the MPC, as well as the consultation of the international protocols ACLS(3) and PHTLS(2). Among the BHNs classified, those identified by the researcher as the most relevant were chosen. It is emphasized that the survey of the empirical indicators from the scientific literature is considered important to base the construction of instruments and is understood as the first stage for its elaboration(11). Some studies reinforce this understanding(7,12,13).
In the second stage, the collective selection of BHN empirical indicators was carried out. In order to do so, a letter of clarification and a semi-structured questionnaire were prepared to organize the concepts of the BHN affected in the MPC, as well as the empirical indicators identified for each need. This instrument provided a dichotomous response, so that the empirical indicators of the BHN presented, selected from the consultation in the scientific literature, could be identified as "relevant" or "not relevant" by SAMU nurses from Curitiba-PR.
After the collective selection, the researcher performed an analysis of the indicators that were repeated and/or similar, to verify the most appropriate indicator and in which BHN it would fit better. In addition, it has regrouped and reorganized the empirical indicators for better applicability.
A total of 37 nurses, both men and women, working in the SAMU ALSU, with at least six months' experience, participated in the study. The exclusion criterion was determined for cases where nurses were on vacation and/or on work leave due to health reasons during the period of data collection.
For the first stage of the research, the analysis was descriptive, based on the scientific literature. In the second stage of the research, the data obtained by the application of the semi-structured questionnaires were compiled in order of receipt in Microsoft Office-Excel spreadsheets, 2013, through which the frequency of the empirical indicators was verified in order to identify the indicators that presented frequency above 80% relevance. Therefore, the data were analyzed through descriptive statistics with absolute frequency and percentage, which is a technique used to order numerical data. The results were presented in tables and charts.
The research covered the ethical aspects, according to Resolution 466/12 of the National Health Council (Conselho Nacional de Saúde – CNS). The project was approved by the Research Ethics Committee (CEP, acronym in Portuguese) of the Federal University of Paraná (UFPR), under registry no. 853,129 and field feasibility provided by the CEP of the Municipal Health Department (SMS), under registry no. 916,256. The research participants were informed about the nature of the objectives, the research methods and the guarantee of confidentiality and anonymity.
RESULTS
To achieve the results of the first stage of the research, it was necessary to identify the BHNs in the context of MPC. The BHNs classified for this research are related to the sequence of the primary assessment in the MPC, as shown in Chart 1.
Chart 1 - Relationship between the primary evaluation sequence and the psychobiological BHNs affected in the context of MPC, 2015, Curitiba, Paraná, Brazil
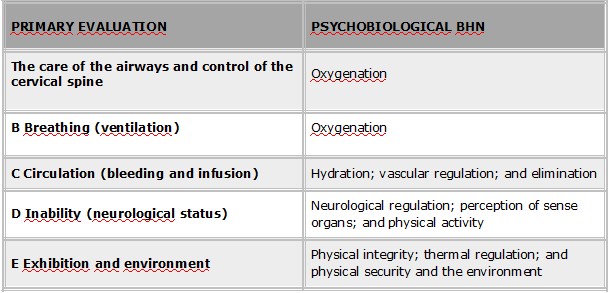
SOURCE: authors.
In this research, psychobiological needs are presented, described and subdivided into: oxygenation, hydration, vascular regulation, elimination, neurological regulation, sense organs perception, physical activity, physical integrity, thermal regulation, and physical security and environment. However, some BHNs were grouped with the purpose of synthesizing the information, so as to enable the construction of a synthetic nursing record instrument, so that it can be applied in professional practice.
After linking the BHNs with the primary evaluation in the context of MPC, the scientific literature was consulted to identify the empirical indicators related to the theme, based on scientific works(8,14,15,16,17); and international protocols(2,3).
Thus, as a result of the first stage of the research, 138 empirical indicators were identified and grouped into eight psychobiological BHNs, distributed as follows: oxygenation (27); hydration (13); vascular regulation (18); neurological regulation (32); perception of sense organs (13); physical integrity (18); thermal regulation (7); and physical security and environment (10).
It was possible to notice that the predominance of the indicators in the BHN of Neurological Regulation (n = 32). It was also found that most of the signs and symptoms of this BHN were in the Glasgow Coma Scale (GCS), which includes important findings to be identified in relation to the patient's level of consciousness in MPC. Two other indices of greater relevance appeared in the BHN of Oxygenation (n = 27) and in Vascular Regulation (n = 18); both highlighted by the sequence of care in the primary approach to patients, in which the priorities are airways, breathing and circulation.
It was observed that some empirical indicators were repeated in different BHNs, and similar indicators were also shown, which shows the amplitude of the representation of terms identified in the scientific literature, in order to allow the use of the most appropriate term for a given BHN, according to reality of MPC.
Regarding the second stage of the research, it should be pointed out that there were difficulties related to the application of the semi-structured questionnaire to the nurses participating in the research. One of the difficulties found was the fact that nurses were absent from their work base, assisting to an occurrence at the moment of delivery and collection of the research instrument.
It should be emphasized that there were also aspects that deserve attention regarding the application of the research instrument, such as the acceptance of participating in the research by all the nurses requested to answer the questionnaire, which demonstrated the interest of these professionals in collaborating for the improvement in the professional practice, as well as the importance of sharing knowledge and the need for valorization in their field of activity.
The nurses participating in the research demonstrated some difficulties of judgment in selecting the relevant empirical indicators. Five nurses pointed out less than five empirical indicators extracted from the scientific literature as "non-relevant" and one of them emphasized the difficulty in making the selection, due to the specificities and diversities of the types of services performed by SAMU, including the transfer of critically ill patients.
As a result of the second stage of the research, of a total of 138 indicators identified in the scientific literature, 96 remained "relevant" above 80%, after the collective selection performed by the participating nurses. The results obtained are listed in Table 1.
Table 1 - Empirical indicators with relevance above 80%, according to the nurses participating in the research, 2015, Curitiba, Paraná, Brazil
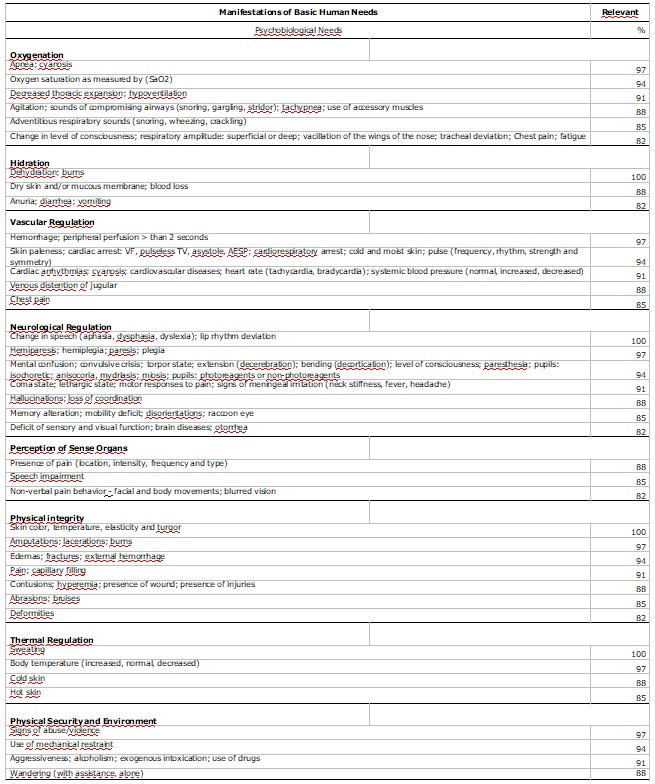
SOURCE: authors.
After analyzing the results shown in Table 1, the need to synthesize the indicators appeared. In addition, empirical indicators have been regrouped and reorganized for best applicability based on a rapid primary assessment, as advocated by international protocols and scientific literature, as shown in Table 2.
Chart 2 - Empirical indicators regrouped and reorganized, 2015, Curitiba, Paraná, Brazil
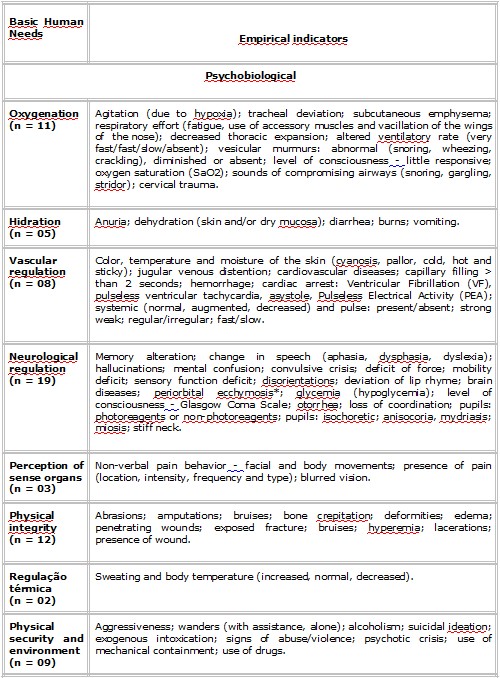
SOURCE: authors based on scientific literature.
After analyzing, reorganizing and regrouping, 69 empirical indicators of the total of 96 were selected as "relevant" by the participating nurses.
DISCUSSION
To approximate the BHNs from the MPC context, it became necessary to consider the primary evaluation, which, according to the ACLS(3), should be done through a quick inspection in the patient in less than 60 seconds, and it can last longer if there is a need to provide emergency care at any time, considered as Basic Life Support (BLS). This evaluation aims to identify the presence of life-threatening problems and immediately correct them, that is, "treat it as you discover", and evaluation and treatment occur simultaneously and evaluation needs to be repeated periodically(3). With the didactic purpose, the primary evaluation of the priorities and the initial maneuvers are presented in a sequence that facilitates the memorization, and they are represented by the mnemonic method ABCDE, according to the PHTLS protocol(2).
It was observed that the empirical indicators that obtained 100% of "relevance" were: dehydration; burns; change in speech; deviation of lip rhyme; color, temperature, elasticity and turgor of the skin; and sweating; however, these signs and symptoms are not a priority in the primary approach to the patient, except skin changes. According to the PHTLS protocol(2), the priorities are: alteration in upper airways, and aspects of breathing, circulation and level of consciousness, which should be 100%.
It was observed that the indicators related to the primary approach to the patient presented lower indices of relevance, demonstrating disagreement with the PHTLS protocol(2). The empirical indicators cited were: sounds of compromising airways (snoring, gargling, stridor) (88%), blood pressure (88%), hypoventilation (91%), pulse (frequency, rhythm, strength and symmetry) (94%), level of consciousness (94%), apnea (97%), hemorrhage (97%) and peripheral perfusion > than 2 seconds (97%). It should be noted that, for the nurses participating in the research, the indicator "vesicular murmurs" had a "relevance" index (76%) lower than expected. These results can demonstrate that nurses in their professional practice in MPC, when performing nursing care, need to act based on international protocols.
Nurses' decision-making should be based on the careful evaluation of signs and symptoms presented by the patient, and on the understanding of their relation to each other and their relevance to care, based on a logical rationale(18). The constant improvement of clinical reasoning is a challenge for all health professionals(19).
The participants of the research suggested the addition, to be considered in the context of MPC, of the following empirical indicators: glycemia in the BHN of neurological regulation; penetrant injuries (knife and gunshot wounds) at the BHN of physical integrity; subcutaneous emphysema in BHN oxygenation; and suicidal ideation in physical security and environment BHN. Specifically in the glycemia indicator, the identification of hypoglycemia was considered important, according to PHTLS(2), since this establishes that in the pre-hospital environment the major focus is for the stabilization of hypoglycemia, considering that the physiological threat caused by the low sugar level is more immediate than high blood sugar.
It is worth noting that the researcher included in the list of selected empirical indicators the "cervical trauma" indicator in the BHN of oxygenation, because in cases of traumatic brain injury, cervical spine fractures occur in about 2% to 5 % of victims and can significantly interfere with ventilation(2).
In the fracture indicator, the term "exposed" was added, considering that the closed fracture is characterized by the other indicators listed: pain, deformities, bruising, and crackling(2). Thus, the "crackle bone" indicator was also included in the BHN of physical integrity.
There was a need to add the indicator of "psychotic crisis" in the BHN of physical security and environment, due to the characteristic of the service provided to patients of this nature. According to Administrative Rule no. 1,864/GM of 2003(20), the SAMU has the duty to perform psychiatric consultations, with the purpose of accompanying mental health situations in crisis until the emergency care network.
It is worth pointing out some limitations identified in the research. The nurses participating in the study did not select the empirical indicator of "vesicular murmurs as "relevant": increased, decreased, or absent; "however, the protocols recommend that breath sounds are important in the primary assessment because, in relation to pulmonary auscultation, decreased vesicular murmur may indicate pneumothorax or hemothorax(2). Thus, this indicator was grouped with the indicator of "adventitious respiratory sounds (snoring, wheezing, crackling)", which was selected by the nurses and remained as "vesicular murmurs: abnormal (snoring, wheezing, crackling), diminished or absent", in the BHN of oxygenation.
Also, two indicators selected as "relevant" by the nurses participating in the research were maintained; however, it should be pointed out that they are in disagreement with the PHTLS protocol(2), taking into account the need to evaluate the priorities in the MPC. It is understood that the indicator of "diarrhea" that presented 82% of relevance, does not represent an imminent risk of life and that the "anuria" indicator, which also presented 82% of relevance, is not possible to evaluate in the MPC, since it is necessary to perform a measurement of urine output.
Finally, it was noticed a difficulty on the part of the nurses who work in the MPC in selecting the priority empirical indicators. This difficulty may be related to the lack of a systematization of nursing care in the service based on international protocols, which suggests the need for training and capacity-building courses.
CONCLUSIONS
The proposed objectives were achieved with the identification of 138 empirical indicators extracted from the scientific literature in the context of MPC, which were grouped into eight psychobiological BHNs. After the collective selection performed by the participating nurses, 96 empirical indicators of greater relevance remained, and they were grouped and reorganized by the researcher, totaling 69 indicators. With a view to considering the BHNs of the patients served by the ALSU of SAMU, the empirical indicators are indispensable and allow establishing a relationship with the BHNs and the sequence of care in the primary approach based on international protocols, which favors the accomplishment of a survey of the terms used in MPC. Thus, it becomes possible to provide individualized nursing care directed to the priorities of patients.
This research also allowed us to conclude that national and international scientific literature deals largely with empirical indicators in the context of MPC, and that there is some difficulty on the part of nurses participating in the research to select the priority empirical indicators, which suggests the need for training and capacity-building courses.
REFERENCES
- Brasil. Ministério da Saúde. Portaria nº 2.048/GM, de 5 de novembro de 2002 [Internet]. Brasília: Ministério da Saúde; 2002[cited 2014 Feb 10]. Available from: http://dtr2001.saude.gov.br/sas/PORTARIAS/Port2002/Gm/GM-2048. htm.
- National Association of Emergency Medical Technicians (NAEMT). PHTLS: Prehospital Trauma Life Support. 8th ed. Rio de Janeiro: Artmed, 2016.
- Aehlert B. ACLS: Suporte Avançado de Vida em Cardiologia. 7th ed. Rio de Janeiro: Elsevier; 2017.
- Alligood MR. Introduction to nursing theory: its history, significance, and analysis. In: Nursing theorists and their work. 8th ed. Missouri: Elsevier; 2013. p. 2-13.
- Lucena ICD, Barreira IA. Revista Enfermagem em Novas Dimensões: Wanda Horta e sua contribuição para a construção de um novo saber da enfermagem (1975-1979). Texto Contexto Enferm. 2011 Jul; 20(3):534-540.
- Horta WA. Processo de enfermagem. Colaboração de Brigitta E. P. Castellanos. Rio de Janeiro: Guanabara Koogan; 2011.
- Mazzo MHSN, Brito RS. Empirical indicators of the affected human needs of puerperal women: a methodological study. Online braz j nurs [internet]. 2015 Mar [cited 2015 Oct 15];14(1):41-50. Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/4602.
- Benedt SA, Bub MBC. Manual de diagnóstico de enfermagem: uma abordagem baseada na teoria das necessidades humanas básicas e na classificação diagnóstica da NANDA. 2nd ed. Florianópolis: Bernúncia Ed.; 2001.
- Conselho Federal de Enfermagem (COFEN). Resolução no 429/2012: Dispõe sobre o registro das ações profissionais no prontuário do paciente, e em outros documentos próprios da enfermagem, independente do meio de suporte - tradicional ou eletrônico [Internet]. Brasília: COFEN; 2012[cited 2014 Jan 22]. Available from: http://www.cofen.gov.br/resoluo-cofen-n-4292012_9263.html
- Polit DF, Beck CT. Fundamentos da pesquisa em enfermagem: avaliação de evidências para a prática de enfermagem. 7th ed. Porto Alegre: Artmed; 2011.
- Andrade LLA. et al. Nursing diagnoses for clients hospitalized in an infectious disease clinic. Rev Esc Enferm USP [Internet]. 2013 Apr [cited 2014 Aug 19];47(2):441-7. Available from: http://www.scielo.br/pdf/reeusp/v47n2/en_25.pdf
- Santana JS, Soares MJG, Nóbrega MML. Empirical indicators for nursing consultation of hypertensive patients in family health units. J Nurs UFPE on line. 2014 Jul; 8(7):1947-55.
- Silva AF, Nóbrega MML, Souto CMRM. Instrument for documentation of nursing process during postpartum. Cienc Cuid Saude [Internet]. 2015 Jul [cited 2015 Jan 10];14(3):1385-93. Available from: http://periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/20227/15373
- Atkinson LD, Murray ME. Fundamentos de enfermagem: introdução ao processo de enfermagem. Rio de Janeiro: Ed. Guanabara; c1989.
- Ball, J. Seidel’s Guide to Physical Examination. 8th ed. Missouri: Elsevier; 2015.
- Garcia TR, Cubas MR. (Org.). Diagnósticos, intervenções e resultados de enfermagem: subsídios para a sistematização da prática profissional. Rio de Janeiro: Elsevier; 2012.
- Potter PA, Perry AG. Fundamentos de enfermagem. 8th ed. Rio De Janeiro: Elsevier; 2013.
- Bittencourt GKGD, Crossetti MGO. Critical thinking skills in the nursing diagnosis process. Rev Esc Enferm USP. 2013;47(2):341-7.
- Cerullo JASB, Cruz DALM. Clinical reasoning and critical thinking. Rev. Latino-Am. Enfermagem. 2010 Jan;18(1):124-9.
- Brasil. Ministério da Saúde. Portaria no 1.864/GM de 29 de setembro de 2003. Institui o componente pré-hospitalar móvel da Política Nacional de Atenção às Urgências, por intermédio da implantação de serviços de atendimento móvel de urgência em municípios e regiões de todo território brasileiro: SAMU - 192. Brasília: Diário Oficial da União; 2003.
All authors participated in the phases of this publication in one or more of the following steps, in according to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the version submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 08/14/2016 Revised: 08/26/2018 Approved: 09/17/2018