Registration of the nursing process for patients with cardiovascular diseases: an integrative review
Allana Raphaela dos Santos Cardoso1,2, Ana Carla Dantas Cavalcanti1, Lyvia da Silva Figueiredo1, Paula Vanessa Peclat Flores1, Juliana de Melo Vellozo Pereira1, Bruno Bompet dos Santos1
1Fluminense Federal University
2Pedro Ernesto University Hospital
ABSTRACT
Aim: to identify the publications related to the registration of the nursing process for patients with cardiovascular diseases. Method: integrative review, carried out using the MEDLINE, CINAHL and LILACS databases, based on a 10-year temporal cut-off. Seven articles, divided into two categories and analyzed according to the theme, were selected. Result: after reading the full text, seven articles were included and two categories were created. Discussion: all studies discussed standardized language systems. Two studies described the interconnection of diagnostic languages, interventions and outcomes. On the other hand, five studies dealt with only one standardized language. Conclusion: nursing process registry studies have been identified for patients with cardiovascular diseases. However, the literature is still limited and of low methodological rigor.
Descriptors: Cardiovascular Diseases; Nursing Processes; Nursing Diagnosis; Nursing Records.
INTRODUCTION
Cardiovascular diseases (CVD) are part of the group of chronic non-communicable diseases which are characterized by having no known etiologic agent and no cure. However, treatment is available but with multicausal risk factors which may or may not be controlled, and a slow and silent pathogenesis. Worldwide, chronic non-communicable diseases are the leading causes of death and disability(1) and represent 30% of morbidity and mortality in Brazil and one-third of all deaths worldwide(2).
Given the importance of these diseases, as determinants of the limitation of the quality of life of the population and the magnitude of morbimortality, it is necessary that the nursing process, both in an outpatient settings and hospital settings, is focused on the patient's responses to the disease process.
The nursing record documents the nursing process, being essential for interventions being planned, implemented and evaluated in safety. Thus, registration supports the continuity of care and ensures communication within the multidisciplinary team(3-6).
The aim of this study is to identify the knowledge produced and published regarding the nursing process in terms of registration of patients with cardiovascular diseases.
METHOD
This is an integrative review of the literature, carried out using the MEDLINE, CINAHL and LILACS online databases. The following steps were used: elaboration of the research question, establishment of criteria for the inclusion and exclusion of studies, categorization of studies, evaluation of included studies, interpretation of results and synthesis of knowledge(7).
The research question considered was: What has been published in terms of nursing records for patients with cardiovascular diseases? Along with this question, the descriptors used to perform the searches were: heart diseases, nursing process, nursing diagnosis and nursing records. The search was conducted in September and October 2015, using the following inclusion criteria: articles in Portuguese, Spanish and English that answered the research question, published in the last ten years.
The following search strategies were used with regard to the MEDLINE, CINAHL and LILACS databases: "heart diseases" AND "nursing process" AND "nursing diagnosis" AND "nursing records". Articles that addressed children with heart diseases, articles without abstracts, articles repeated in the databases, in editorial format, letters to the editor and reflective articles were excluded.
Thirty studies were identified in the MEDLINE, LILACS and CINAHL databases, and were referred to two researchers for consensus selection of the studies to be screened. After the titles and abstracts were read there were no duplications, and 16 articles were excluded. Among these articles, one was excluded for lack of a summary, two articles for involving children, and three for not being published within the period under consideration. Eight studies were chosen for the reading of the full text in order to answer the research question. One article was excluded because it did not respond to the question. In total, seven papers were included for analysis and interpretation.
Evidence-based practice advocates classification systems, depending on the methodological approach adopted, which is based on the study design(8). Level 1 is applied to evidence resulting from meta-analyzes of multiple randomized controlled trials; Level 2 for evidence obtained in individual studies involving an experimental design; Level 3 for evidence from quasi-experimental studies; Level 4 for evidence from descriptive (or non-experimental) studies or ones adopting a qualitative approach; Level 5 for evidence from case or experience reports; and level 6 for evidence based on expert opinion, according to Agency for Healthcare Research and Quality categorization(8).
The studies were divided into two categories for analysis according to the subject matter. These were termed as: studies that associated standardized NNN languages and studies that addressed a single standardized language.
RESULTS
The sample comprised 7 studies, selected as shown by the published selection flowchart (Figure 1).
Figure 1. Flowchart explaining the selection of articles. 2016, Niterói/RJ.
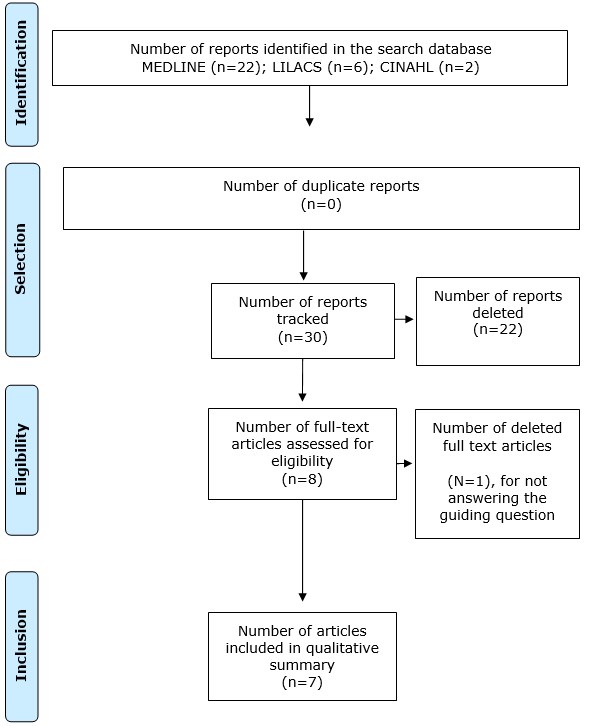
Source: authors.
Evaluating the seven publications in terms of origin, three are from international and four are from national journals. International publications were all written in English. As for the type of publication, all are scientific articles.
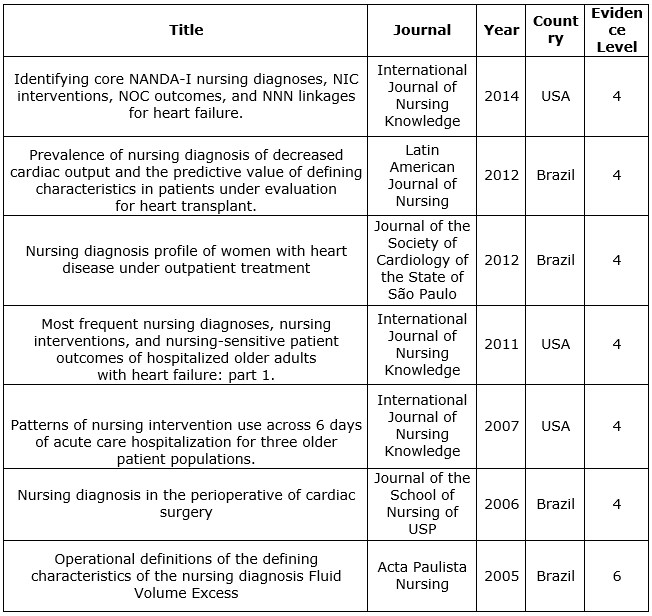
Table 1 presents the identification characteristics of the publications regarding title, journal, year, country of publication and level of evidence. From the sample included in this review, six studies provide Level 4 evidence and one publication provides Level 6 evidence.
Table 1. Identification characteristics of the publications regarding title, journal, year, country of publication and level of evidence. (n=7) Niterói, 2016.
Source: authors.
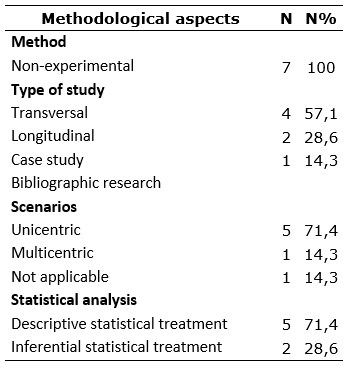
Regarding the topic, five publications studied nursing diagnoses using the NANDA International taxonomy, one article studied the relationships between diagnoses (NANDA-I), interventions (NIC) and nursing outcomes (NOC) in patients with heart disease and one article presented nursing interventions as the objects of the study. Table 2 presents the main methodological aspects of the analyzed studies:
Table 2. Main methodological aspects of the analyzed studies (n=07). Niterói, 2016.
Source: authors.
The most frequent studies are methodologically non-experimental, transversal, unicentric and incorporating descriptive statistics (use of mean, standard deviation and percentages). It is noteworthy that, with regard to the cross-sectional studies, most (three articles) adopted a retrospective approach, with a chart analysis. It should be noted that with regard to the studies involving inferential analysis that sought associations, the following statistics were used: Odds Ratio calculations (study 2) for the purpose of verifying the predictive value of defining characteristics for a given nursing diagnosis, and calculation of the Friedman, Kenall and Kappa Tests in study 6.
DISCUSSION
STUDIES THAT ASSOCIATE NNN STANDARDIZED LANGUAGES
Of the seven articles found, two involved a description of the three standardized languages, Nanda International (NANDA-I), Nursing Interventions Classification (NIC) and Nursing Outcomes Classification (NOC) as to how they were associated and interconnected. The use of standardized languages has been mentioned in the publications regarding its benefits to promote quality nursing record and, consequently, safer and more systematized nursing care.
A descriptive, retrospective study in which 272 hospitalization records were analyzed, aiming to identify links of diagnosis, interventions, results and links of real clinical data using standardized language systems such as NANDA-I, NIC and NOC for patients with Heart failure (HF), identified ten NNN connections for patients with more frequent HF as a result of a survey of medical records. The use of NNN terminology was described in more than 50% of the medical records, especially regarding the nursing diagnoses for the HF patients(9).
This study has also demonstrated that the four most common nursing diagnoses in patients with heart failure were knowledge deficit, decreased cardiac output, impaired tissue integrity risk, and ineffective respiratory pattern. These four were responsible for almost 50% of the most common nursing diagnoses for HF patients. Ten NIC interventions accounted for 51.03%, including fluid monitoring, cardiac care, and teaching: procedure/treatment, fall prevention and emotional support were used particularly frequently(9).
Another descriptive, comparative and multicenter study aimed to report the ten most frequently documented NNN connections by nurses for patients aged 60-89 years with a diagnosis of HF, and to evaluate and describe recovery, quality and limitations in terms of the efficacy of nursing outcomes. The result of the analysis of the 302 records of hospitalized patients was the knowledge that, of the ten NNN connections, only 4 were commonly used by the three hospitals: activity intolerance, decreased cardiac output, poor knowledge and risk of falls. As for interventions, two were similar in two hospitals: the treatment of pain and skin surveillance.
Both studies have demonstrated how important it is to use standardized language to produce and use data that support the practice, research, or improvement of evidence-based quality.
However, the second study mentioned pointed out that the use of electronic records is a facilitator of the work of the diagnosing nurse, as long as the electronic medical record has been built based on standardized language systems. This information does not corroborate with most of the publications, perhaps because the electronic record facilitates the work of the nurse who performs the nursing process, and is not always analyzed exhaustively and in detail in relation to all its aspects(10).
It is a fact that the use of electronic records associated with the use of standardized languages in nursing has numerous benefits, because such use improves communication between professionals. In addition, it makes possible patient and nursing assistance follow-up in a more consistent and practical way, especially when it comes to care for patients with cardiovascular disorders(10).
The studies that investigated the major NNN connections related to patients with HF and who were predominantly elderly. The standardized NNN language allows the comparison of nursing data between sites and specialties, aimed at improving patient care. In the second study there was also a notable absence of diagnoses related to the psychosocial aspect, with a predominance of connections referring to physiological aspects.
STUDIES ADDRESSING A SINGLE STANDARD LANGUAGE
The diagnostic language describing the responses of patients with cardiovascular diseases was identified in 5 studies.
A study with retrospective documentary analysis identified the prevalence of defining characteristics for nursing diagnoses with regard to reduced cardiac output. Data were obtained through documentary analysis of the clinical records of 38 patients undergoing cardiac catheterization(11). The defining characteristics were particularly related to the alteration of afterload(11).
The majority of the characteristics of nursing diagnoses were more frequent in subjects with reduced cardiac index. In these individuals, the most frequent were increased systemic vascular resistance with OR=4.533, the third bulge OR=3.429 IS THIS CORRECT? and the decreased ejection fraction OR=2.850 being those related to the altered afterload(11). The ones with the highest odds in terms of predictive value were the third bulge and bradycardia related to the category of noninvasive evidence, increased pulmonary vascular resistance and increased systemic vascular resistance, decreased pulmonary vascular resistance, and decreased ejection fraction in the category of invasive evidence(11).
Another cross-sectional study identified the Nursing Diagnoses (ND) of women with heart disease, in outpatient care, as well as the defining characteristics and related risk factors of ND in this population with a prevalence greater than 50%. Twenty-one women were studied of whom 7.9 ND/patients were identified, with a prevalence of more than 50%, as follows: sedentary lifestyle, ineffective health self-management, risk of falls and chronic pain(12).
These studies expressed what has been published in the scientific literature on nursing diagnoses with regard to patients with adult cardiovascular disorders, both of which raised the question regarding the need for further studies using the standard NANDA-I language, relating the detailed and quantitative analysis of the defining characteristics of the most prevalent diagnoses in patients with cardiovascular diseases, aiming to promote nursing care that is particularly focused on the needs of patients based on scientific evidence(11-12).
A study conducted in São Paulo/Brazil identified the main nursing diagnoses of patients during the perioperative period of cardiac surgery, and evaluated the concordance between the diagnoses drawn by the first nurse, the author of the study, and other nurses. In the preoperative period, there was agreement between the author and the nurses in only 3 of the 9 diagnoses; in the transoperative period there was 100% agreement in 7 of the 9 diagnoses; there was no agreement in period 2; in the postnatal periods, 10 of the 15 diagnoses presented complete agreement; in one diagnosis there was total disagreement; and in 4 there was no statistically significant agreement. Although not aimed at implementing the interventions, this study helps the nurse to chart the patient care plan in the perioperative period(13).
Among the nursing diagnoses found in the preoperative period, we can highlight a frequency of more than 70% in terms of activity intolerance, risk of Peripheral Neurovascular Dysfunction, Risk of Infection, Ineffective Respiratory Pattern, Pain and Impaired Cardiopulmonary Tissue Perfusion. In the transoperative period, nine diagnoses stand out, among which eight have a frequency of 100%, including Risk of Imbalance in the Volume of Fluid, Risk of Aspiration, Risk of Impaired Skin Integrity, Impaired Gas Exchange among others, and during the post-operative period, ten stand out among the 15 with a frequency of 100%. These include Impaired Physical Mobility, Aspiration Risk, Deficit in Self-Care Bathing and Hygiene, and Impaired Skin Integrity.
A review of the literature from 1985 to 2001 was carried out. Its purpose was to elaborate operational definitions for the defining characteristics of the nursing diagnosis of excessive fluid volume. The definitions were based on the concepts of scholars; then 4 "expert" nurses were consulted for the analysis and contribution to the creation of operational definitions.
The operational definitions were sent to a scholar in the subject and thus defined. The purpose of the study was the elaboration of a database to measure the defining characteristics in order to help formulate the nursing diagnosis, favoring the understanding of each defining characteristic(14).
Only one article identified interventions for patients with HF who were over 60 years of age. This study was extremely important in terms of differentiating the NIC interventions of patients with HF from the interventions of other groups of patients of the same age group(15).
CONCLUSION
Studies on nursing process registration for patients with cardiovascular diseases were identified. However, the literature is still limited and of low methodological rigor, making it impossible to construct evidence for the elaboration of protocols and consensus on nursing diagnoses, interventions and results. It should be noted that the SLPs found were NANDA-I, NIC and NOC.
REFERENCES
- Beatty A. Country-Level Decision Making for Control of Chronic Diseases: Workshop Summary. Washington, D.C. National Academy of Sciences. [internet]. 2013 [Cited 2016 Apr 29] Available from: http://www.nap.edu/read/13337/chapter/1
- Ministério da Saúde (BR). Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis no Brasil 2011-2012 [internet]. Brasília; 2011. [Cited 2016 Apr 29] Available from: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf
- Carvalho EC, Cruz DALM, Herdman HT. Contribuição das linguagens padronizadas para a produção do conhecimento, raciocínio clínico e prática clínica da Enfermagem. Rev. bras. Enferm (Online) [internet]. 2013 Sep; 66(spe): 134-141. [Cited 2016 Apr 29] Available from: http://www.scielo.br/pdf/reben/v66nspe/v66nspea17.pdf
- Barral LN, Ramos LH, Vieira MA, Dias OV, Souza LP. Análise dos registros de enfermagem em prontuários de pacientes em um Hospital de Ensino. Rev Min Enferm (Online) [internet]. 2012 feb; 16(2): 188-193. [Cited 2016 Apr 29] Available from: http://www.scielo.br/pdf/ape/v22n3/a12v22n3.pdf
- Moorhouse MF, Doenges ME, Murr AC. Diagnósticos de Enfermagem, Intervenções, Prioridades e Fundamentos 12.ed. Rio de Janeiro: Guanabara Koogan; 2012.
- Querido DL, Almeida VS, Esteves AP, Bornia RB, Júnior JA, Silva RW. Qualidade dos registros de enfermagem em uma Maternidade Escola: um estudo descritivo. Online Braz J Nurs (Online) [internet]. 2015 Dec [cited 2016 apr 29]; 14 (suppl.):437-9. Available from: http://www.objnursing.uff.br/index.php/nursing/article/viewFile/5366/pdf_906
- Sasso MKD, Pereira SRCC, Maria GC. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto contexto enferm (Online) [internet]. 2008 Dec [Cited 2016 Apr 29]; 17(4): 758-764. Available from: http://www.scielo.br/pdf/tce/v17n4/18.pdf
- Burns PB, Rohrich RJ, Chung KC. The Levels of Evidence and their role in Evidence-Based Medicine. Plast Reconstr Surg (Online) [internet]. 2011 July [Cited 2016 Apr 29]; 128(1): 305–310. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3124652/pdf/nihms288127.pdf
- Parque H. Identifying core NANDA-I nursing diagnoses, NIC interventions, NOC outcomes, and NNN linkages for heart failure. Int. J Nurs Knowl 2014 Feb; 25(1):30-8 [included in the review]
- Scherb CA, Head BJ, Maas ML, Swanson EA, Moorhead S, Reed D. Most frequent nursing diagnoses, nursing interventions, and nursing-sensitive patient outcomes of hospitalized older adults with heart failure: part 1. Int J Nurs Terminol Classif. 2011 Jan-Mar; 22(1):13-22 [included in the review]
- Matos LN, Guimarães TF, Brandão Marcos AG, Santoro DC. Prevalence of nursing diagnosis of decreased cardiac output and the predictive value of defining characteristics in patients under evaluation for heart transplant. Rev. Latino-Am Enferm. (Online) [internet]. 2012 Apr [Cited 2016 Apr 29]; 20(2): 307-315. Available from: http://www.scielo.br/pdf/rlae/v20n2/pt_13.pdf [included in the review]
- Silva ACLR da, Andrietta MP, Lopes JL, Mansur AP, Silva RCG. Nursing diagnosis profile of women with heart disease under outpatient treatment. Rev. Soc. Cardiol. Estado de São Paulo. 2012, 22(2, supl, A): 8-13 [included in the review]
- Galdeano LE, Rossi LA, Santos CD dos, Dantas RAS. Nursing diagnosis in the perioperative of cardiac surgery. Rev Esc Enferm USP (Online) [internet]. 2006 [Cited 2016 Apr 29]; 40(1): 26- 33. Available from: http://www.scielo.br/pdf/reeusp/v40n1/a03v40n1.pdf [included in the review]
- Boery RNSO, Guimarães HCQCP, Barros ALBL Operational definitions of the defining characteristics of the nursing diagnosis Fluid Volume Excess. Acta Paulista de Enferm SP (Online) [internet]. 2005[Cited 2016 Apr 29]; 18(2): 197- 202. Available from: http://www.scielo.br/pdf/ape/v18n2/a13v18n2.pdf. [included in the review]
- Shever LL, Title M, Dochterman J, Fei Q, Picone DM. Patterns of nursing intervention use across 6 days of acute care hospitalization for three older patient populations. International Journal Of Nursing Terminologies and Classification. 2007; 18(1): 18- 29[included in the review]
All authors participated in the phases of this publication in one or more of the following steps, in according to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the version submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 04/05/2016 Revised: 01/31/2017 Approved: 02/02/2017