Cognitive assessment of elderly people in long-stay institutions: a cross-sectional study
Vivian Carla de Castro1, Celmira Lange2, Vanessa Denardi Antoniassi Baldissera1, Eraldo Schunk Silva1, Lígia Carreira1
1State University of Maringa
2Federal University of Pelotas
ABSTRACT
Aim: To evaluate the cognition of elderly residents in long-term institutions and the association of cognitive status to sociodemographic variables and the domain of the Mini Mental State Examination (MMSE). Method: This is a descriptive, cross-sectional and quantitative study. Data were collected from 161 elderly, using the MMSE, between January and March 2013 and were analyzed using chi-square and Mann-Whitney tests. Results: 39.8% of the elderly had cognitive impairment, and worse cognitive performance occurred in females. The domains of the MMSE had a statistically significant association with cognitive decline, and orientation, attention, and calculation and evoked memory had greater influence on the presence of cognitive impairment. Conclusion: MMSE is a practical tool for cognitive evaluation of the elderly, and it can guide nursing interventions in order to foster standardization of the goals to be achieved in the attention to the institutionalized elderly.
Descriptors: Health of Institutionalized Elderly; Cognition; Homes for the Aged; Geriatric Nursing; Aged.
INTRODUCTION
Globally, the proportion of elderly has grown significantly, creating numerous social and economic repercussions, particularly in developing countries. In these, the supply of health needs is challenged by the limited resources, or the management of these is ineffective and depends on the development of specific and innovative policies for the elderly. Brazil is included in this group and has suffered successive declines in birth and mortality rates in recent decades. This has contributed to the current population accounting for 21 million people aged 60 or over(1,2).
The realization of successful aging has, among its features, the maintenance of cognitive abilities, which is associated with longevity, quality of life, physical and social well-being and, consequently, satisfactory levels of autonomy and independence(3,4). With biological aging, however, the central nervous system is one of the most compromised, particularly in regions responsible for cognitive functions, since brain hypotrophy and changes in the neurotransmitter system occur(5). Although structural changes are made, their intensity is strongly influenced by cultural and genetic factors, comorbidities, and the lifestyle to which the elderly are exposed(6).
Cognitive changes, commonly related to attention, memory, language, executive and psychomotor processing speed(3) represent a great impact on the lives of the elderly and their families. The progression of cognitive decline determines dementia, affecting 5 to 30% of elderly Brazilians, and interferes with their functionality and quality of life(6).
In the face of the demographic and epidemiological changes experienced, families have faced difficulties in caring for the elderly in their home, mainly by changes in family structure, such as the increased participation of women in the labor market and new family arrangements(1). Moreover, the presence of weakness, understood here as a geriatric multifactorial syndrome, whose development is linked to the changes associated with aging(2), when not identified and treated early, prevents the realization of activities previously carried out by the elderly(7), thus contributing to the increased demand for long-term care facilities (LTCF) for the elderly.
In Brazil, there are more than 80,000 elderly housed in approximately 3,500 LTCF. In addition to the factors mentioned, female elderly over 70 years of age, single, childless or widowed and who have a low income are more prone to be institutionalized(1). Although this is not always a bad option, it entails impairment to the physical and emotional health of the elderly, and the principal causes are lack of family and social support(8). It is therefore incumbent on LTCF to provide a qualified and focused geronto-geriatric attention aimed at the needs of the elderly, through the work of a multidisciplinary team/sup>(1) and taking into account the heterogeneity of its residents, whose needs can permeate the instrumental or basic activities of daily living(9).
From this perspective, the evaluation and monitoring of cognitive skills, using neuropsychological tests, allows the identification of the real needs of the institutionalized elderly and the adjustment of health care, considering the different processes of aging(10). Among the cognitive screening tests aimed at adults and older people, the Mini Mental State Examination (MMSE) is the most frequently used among geronto-geriatric professionals in the world. The original test publication is the most frequently cited in scientific journals in the neurology area and it has been used as the only tool or component of neuropsychological assessment batteries in research(11).
As a member of the multidisciplinary team, the nurse has the authority to perform multidimensional assessments of the elderly, making use of this and other strategies in order to investigate the mental, social, and functional state of the elderly(1,2). Nursing care for institutionalized elderly should be guided by systematized actions, based on the survey of the needs of those affected, with the support of nursing theories(12).
In this context, the following research questions emerged: What is the cognitive status of elderly residents in LTCF? Is the cognitive status associated with sociodemographic variables and domains of MMSE? In an attempt to answer them, the aim of this study was defined: To evaluate the cognition of elderly residents in LTCF and the association of the cognitive status of sociodemographic variables and domains of MMSE.
METHOD
This was a descriptive and cross-sectional study using a quantitative approach, performed in seven long-stay institutions regularly registered at the Secretaria de Assistência Social e Cidadania (SASC) (Department of Social Welfare and Citizenship) of Maringá/PR, Brazil. These institutions have given written permission for the research.
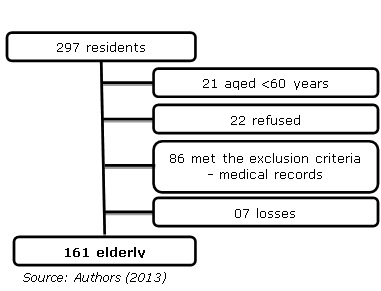
Of the 43,716 seniors who made up the population of Maringá, representing 12% of the total population, 297 (0.68%) reside in LTCF and they comprised the population of this study, from January to March 2013. Initially, the multidisciplinary medical records of each resident were analyzed, in order to select the subjects that participated in the study. The inclusion criteria adopted were: To be aged 60 years or older and not to present conditions that prevent them from answering questions in the MMSE. Thus, we excluded those elderly with hearing loss, aphasia or clinically significant mental impairment, according to the documented information in the medical records. It is noteworthy that, although residing in LTCF, 21 individuals were younger than 60, and did not reach the age criterion established.
During the initial selection of the sample (Figure 1) the responses of seven subjects were not considered for inclusion in the study as it was impossible to calculate the scores due to improper filling of the score on the instrument. Thus, the final sample consisted of 161 elderly.
Figure 1: Steps for the definition of the sample of the study elderly. Maringá/PR, 2013
Primary data were obtained by applying the MMSE(13), composed of questions grouped in the domains temporal orientation, spatial orientation, immediate memory, attention and calculation, evocation of memory, language, and visual constructive capacity. The total score ranges from zero to 30 points, indicating a greater or lesser degree of cognitive impairment, respectively. The elderly were classified with or without cognitive decline as the cutoffs proposed by the authors: score below 20 points for illiterate elderly; 25 points for seniors with one to four years of study; 26.5 for seniors with five to eight years of study; 28 points for the aged having 9 to 11 years of schooling; and 29 points for the elderly over 11 years of study(13).
The collection of sociodemographic data of the elderly was gathered from the medical records, using an instrument developed by the researcher and these data underwent descriptive statistical analysis. The scores from the MMSE were analyzed using the chi-square test for association with sociodemographic variables, and by means of the Mann-Whitney test (the sum of rank test) to test hypotheses regarding the cognitive decline in each domain of MMSE, using the Software Statistical Analysis System (SAS) 91.1. The significance level for the statistical tests was 5%.
This study is part of research in the nominated master's thesis "Attitudes of the elderly regarding leisure: a study carried out in long-stay institutions", approved by the Ethics Committee for Research Involving Human Beings of the State University of Maringá (COPEP/UEM) on 11/12/2012, under Opinion No. 160,445, according to Resolution 466/12. After the clarification of the research objectives, the elderly who agreed to participate in the study signed or marked their fingerprints on the Consent Terms in two ways.
RESULTS
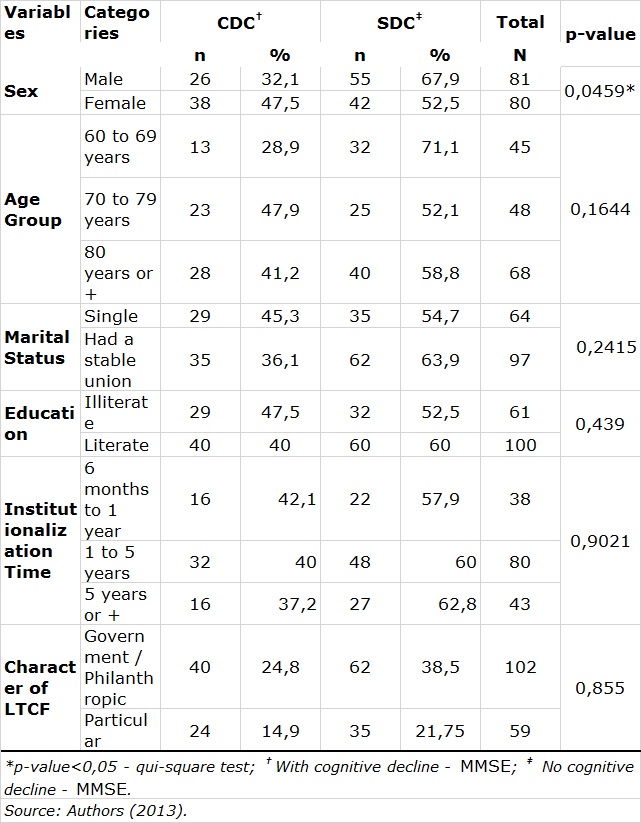
The study included 161 institutionalized elderly, comprising 81 (50.3%) males and 80 females (49.7%). Regarding the MMSE, the average for all seniors was 20.9 points (± 7.1). Sixty-four (39.8%) elderly people with cognitive decline, whose average on the MMSE scale was 13.6 points (± 4.9), were identified. There was a predominance of elderly aged 80 or older (42.2%). By relating age with cognitive decline, it may be highlighted that 47.9% of seniors aged 70 to 79 years and 41.2% of the elderly aged 80 or older had cognitive decline. Regarding marital status, it was found that most had or have had a stable union, which included married couples, widowed or separated (60.25%). In relation to cognitive state, it was noted that 45.3% of seniors who reported never having had a partner (a) showed cognitive decline.
Regarding the level of schooling, there was a prevalence of literate elderly (62.1%), who had apparently a better cognitive level compared to illiterate elderly. Although there is no statistical evidence, it is possible to observe a reduction in the percentage of individuals with cognitive decline of 47.5% to 40% when comparing illiterate and literate elderly, respectively. As to the time of institutionalization, most had resided for at least one year and a maximum of five years (49.7%) in LTCF, and the institutions that housed the largest number of elderly (63.3%) were governmental or philanthropic (Table 1).
Among the 64 elderly with cognitive decline, there was a predominance of females (59.4%), aged 80 years or older (43.75%) who had or have had a companion (a) (54.7%), who attended from one to eight years of formal education (46.9%) and who had between one and five years of institutionalization (50.0%). By associating the variable sex with cognitive decline, a statistically significant difference was observed (p=0.0459) between men and women, who obtained on the MMSE scale, respectively, the average scores of 14.8 and 12.8 for seniors with cognitive decline and 25.9 and 25.4 for older people without cognitive decline. For the other categorical variables there were no statistical differences in relation to cognitive decline (Table 1).
Table 1. Distribution of institutionalized elderly people with and without cognitive decline, according to sociodemographic characteristics. Maringá, PR, Brazil 2013
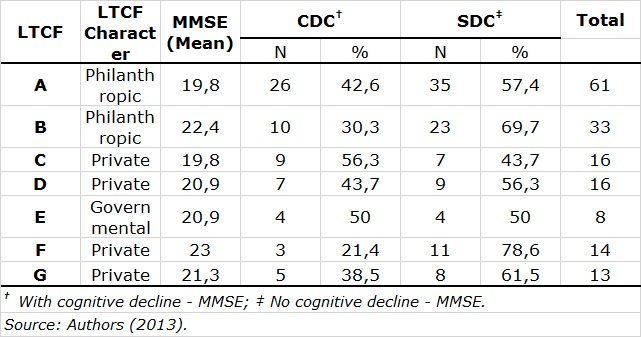
Regarding the cognitive decline of the elderly in the seven LTCF studied, it was found that of the two who obtained the lowest average on the MMSE scale (19.8), one also presented the highest percentage of elderly people with cognitive decline (56.3%). However, the highest average for the MMSE (23.0) was achieved only by a private institution, which had the lowest percentage of elderly people with cognitive decline (21.4%) (Table 2).
Table 2. Distribution of institutionalized elderly people with and without cognitive decline, according to long-term care facilities. Maringá, PR, Brazil 2013
With regard to the areas that make up the MMSE, it was found that all showed statistically significant differences with respect to cognitive decline in elderly subjects (Table 3).
Table 3. Cognitive assessment of institutionalized elderly, according to domain of MMSE . Maringá, PR, Brazil 2013
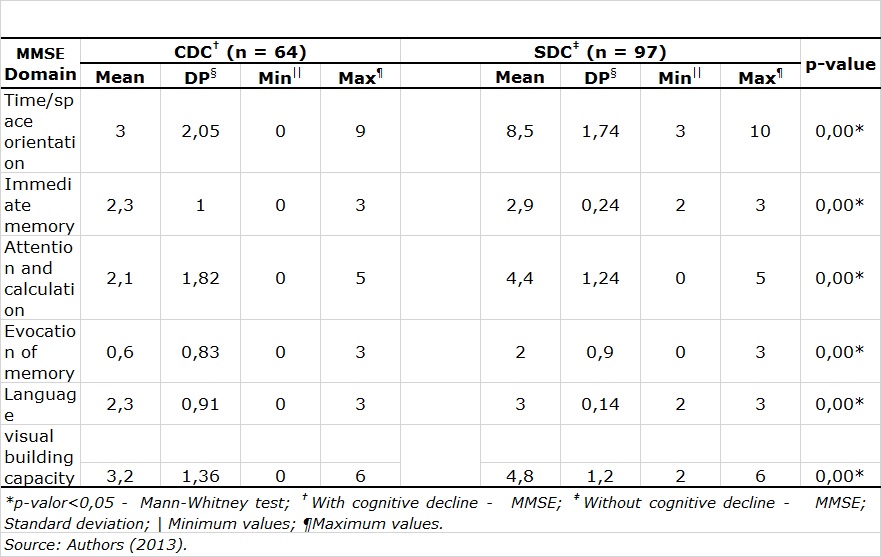
Especially in the categories time and space orientation, attention and calculation, and evoked memory, you can see that the averages for elderly people with cognitive decline are lower than half the average obtained by those who did not have cognitive decline (Table 3).
DISCUSSION
The feminization of the age group of the elderly, resulting from the difference between the life expectancy of men and women, exposes women to poverty, loneliness, and risk of morbidity(7,14), since female presence is more frequent than male in LTCF(7,12,14). However, among older people included in this study there was no predominance of any sex, a condition that may be linked to the selection of subjects, based on inclusion and exclusion criteria.
It is also necessary to consider the variability of the composition of the collective households, as there are constant entries and exits of elderly people, especially for the high mortality in this population, as shown by the survival analysis conducted in England and Wales, in which the outcome was four times higher among institutionalized elderly than in community-dwelling senior adults(15).
Advancing age entails the increased risk of disability, as well as the occurrence of chronic diseases and hospital admissions, thus indicating a tendency to increase the chance of institutionalization(14), making the prevalence of older elderly in LTCF(12) common, as evident in the results of this research.
With regard to cognitive decline, it was found that 39.8% of the elderly presented this condition. This number is significant when considering that of the elderly who attended community groups in the city of Santa Maria/RS, Brazil(10), 23.6% had cognitive decline. It is argued, however, that all participants of the study were schooled. On the other hand, the result of a study conducted in an LTCF in Londrina/PR, Brazil(7) is similar to that found in Maringá/PR, Brazil, since 39.3% of the elderly had cognitive impairment.
Another noteworthy finding in this study refers to the 47.9% of seniors aged 70 to 79 years who had cognitive decline, a percentage higher than that among those aged 80 and over (41.2%).
The same condition was identified in the study conducted in Londrina/PR, Brazil(7), abovementioned, in which the authors attributed this event to the inability of some older seniors to respond to the MMSE, a situation that also occurred in the LTCF of Maringá/PR , Brazil. A cohort developed in São Paulo/SP, Brazil, stressed that advancing age causes a reduction in the percentage of cognitive performance above average, due to the decreased brain plasticity(4).
It is noteworthy that almost half of single elderly (45.3%) had cognitive impairment according to the MMSE. A study conducted in the state of Rio Grande do Sul, Brazil, compared the cognitive performance of elderly people with and without a partner. The first had a prevalence of 45% lower cognitive deficit, which could be related to the possibility of involvement of the partner in health care(6), according to the justification of the authors.
In the population in question, there was no significant association, from a statistical point of view, between educational level and cognitive decline. The literature points out that low educational level is associated with the presence of cognitive impairment(6,7), suggesting that the improvement in the education of individuals could delay the onset of dementia(16). An integrative analysis of longitudinal studies of aging(17) emphasizes that, although more years of education are associated with higher baseline scores of MMSE, there was no significant changes in scores of the intrapersonal MMSE associated with education over time in the six cohorts analyzed.
The finding of this research is confirmed by a study carried out in Londrina/PR, Brazil(7), which highlighted that the lack of association does not disregard the perception, through descriptive analysis, that more years of formal education lead to better cognitive status. In this sense, the nurse should be aware of the ability of older people with low education to understand the health information, in order to elaborate interventions that will minimize possible losses on cognition(6).
The statistical analysis found an association between sex and cognitive decline, with poorer performance on the part of the women of the studied population. Although no statistical significance was found in this association, a study of the elderly in Rio Grande do Sul, Brazil(6), showed prevalence of deficit 22% higher among women. As a possible explanation, the authors pointed to the longer life expectancy of females compared to males. On the other hand, international integrative analysis argues that this result varies depending on the sample involved, as two studies in which women had higher scores than men on the MMSE and two others that observed greater cognitive decline in females, were analyzed(17).
Of the averages of MMSE scores calculated for the seven LTCF, two were below the minimum cutoff set by educational level (20 points) and five were located between the first and the second cutoff point (25 points) for individuals who attended from one to four years of formal education. It is believed that this is due to the large number of illiterate elderly. It is noteworthy, in this case, that greater opportunities for access to literacy means could contribute to promote the health of older people living in the institutional context(14).
The score analysis in each MMSE domain helps to relate the profile of cognitive performance with different outcomes, such as a survival analysis with Korean elderly, which showed that the domains temporal orientation and attention and calculation were statistically associated with mortality(18). However, a prospective longitudinal case-control study in elderly hospitalized in Colombia, pointed out that low scores in the domains spatial and temporal orientation at admission were risk factors for the occurrence of delirium(19). Another study, conducted in Taiwan, noted that worse performance in the domains orientation and visual constructive capacity were risk factors for hip fracture(20).
In this study, the domains temporal and spatial orientation, memory recall and attention and calculation obtained the biggest differences between the mean MMSE scores for older adults with and without cognitive decline. The orientation test is part of the routine of the mental state examination, from the clinical point of view, and even small errors are useful for screening for cognitive impairment and alerting to the need for intervention(18,19).
Temporal orientation is more susceptible to change than spatial orientation due to its deficiency at the beginning of the cognitive decline process. Furthermore, it is the domain that presents the most intense changes in the course of Alzheimer's disease. This is because the judgment about the time interval depends on access to both key markers of episodic and semantic memory(18,20). Regarding the domain attention and calculation, it is considered the most difficult among all MMSE items, since the skills needed to run the commands are subject to deterioration in normal aging and, therefore, this area is useful to assess the age-related decline(18).
The MMSE has been widely used as a screening tool for cognitive decline; however, it is known that it can also be used in monitoring the evolution of diseases and in the supervision of pharmacological and non-pharmacological treatments(11). In the latter case, analysis of the MMSE scores of each domain is important in order to distinguish, for example, problems related to dementia, to the stage of Alzheimer's disease or cognitive decline frame(20). In this sense, the MMSE provides an opportunity to cover different populations in different contexts, although there is still little research exploring the specific contribution of each domain or their combination for cognitive evaluation of the individual.
The nursing care geared to the elderly has its singularities, which are more evident when it comes to the institutional context, and these singularities are configured as challenges for the professionals. Nurses must be able to develop clinical reasoning and carry out the overall assessment to interpret the peculiarities of the health conditions of the elderly, and to prepare the appropriate care plan based on gerontology-geriatric knowledge(12). The use of validated tools for measuring cognitive impairment provides reliable data for nursing intervention and favors the standardization of the goals to be achieved in the attention to the institutionalized elderly.
CONCLUSION
In the LTCF studied there was a predominance of elderly aged 80 or older, literate and who have or have already had a partner. The institutionalization period ranged from one to five years and the institutions were mostly governmental or philanthropic. Of the elderly, 39.8% had cognitive impairment, according to the MMSE, and this percentage varied between 21.4% and 56.3% in institutions, with a minimum average obtained by the MMSE of 19.8 and maximum of 23.0. Among the variables gender, age, marital status, education, institutionalization time, and character of LTCF, only the first showed a statistically significant association with respect to cognitive decline, and it was more present among women. The domains that make up the MMSE had a significant association with cognitive decline, and the domains orientation, attention and calculation and memory evocation showed the most evident differences for older people with and without cognitive impairment.
The MMSE has proved to be a practical tool for assessing the cognition of institutionalized elderly in this study and, from the score achieved, the association of cognitive decline to the sociodemographic characteristics and the instrument domains were notable, using a considerably significant sample in order to add benefits to the body of knowledge existing in this perspective. However, the research also has limitations, such as the non-inclusion of a variable regarding the health conditions of the elderly, which could influence their cognitive performance.
REFERENCES
- Oliveira PB, Tavares DMS. Condições de saúde de idosos residentes em instituição de longa permanência segundo necessidades humanas básicas. Rev. Bras. Enferm. 2014; 67(2): 241-6.
- Leonardo KC, Talmelli LFS, Diniz MA, Fhon JRS, Fabricio-Wehbe SCC, Rodrigues RAP. Avaliação do estado cognitivo e fragilidade em idosos mais velhos, residentes no domicílio. Cienc Cuid Saude. 2014; 13(1): 120-7.
- Vance DE, Graham MA, Fazeli PL, Heaton K, Moneyham L. An Overview of Non-pathological Geroneuropsychology: Implications for Nursing Practice and Research. J Neurosci Nurs. 2012; 44(1): 43–53.
- Silva HS, Duarte YAO, Andrade FB, Cerqueira ATAR, Santos JLF, Lebrão ML. Correlates of above-average cognitive performance among older adults: the SABE study. Cad. Saúde Pública. 2014; 30(9): 1977-86.
- Cruz DT, Cruz FM, Ribeiro AL, Veiga CL, Leite ICG. Associação entre capacidade cognitiva e ocorrência de quedas em idosos. Cad. Saúde Colet. 2015; 23(4): 386-93.
- Zortea B, Gautério-Abreu DP, Santos SSC, Silva BT, Ilha S, Cruz VD. Avaliação cognitiva de pessoas idosas em atendimento ambulatorial. Rev Rene. 2015; 16(1): 123-31.
- Mello BLD, Haddad MCL, Dellaroza MSG. Avaliação cognitiva de idosos institucionalizados. Acta Scientiarum. 2012; 34(1): 95-102.
- Vicente FR, Santos SMA. Avaliação multidimensional dos determinantes do envelhecimento ativo em idosos de um município de Santa Catarina. Texto contexto – enferm. 2013; 22(2): 370-8.
- Maseda A, Balo A, Lorenzo–López L, Lodeiro–Fernández L, Rodríguez–Villamil JL, Millán–Calenti JC. Cognitive and affective assessment in day care versus institutionalized elderly patients: a 1-year longitudinal study. Clin Interv Aging. 2014; 9: 887–94.
- Leite MT, Hildebrandt LM, Kirchner RM, Winck MT, Silva LAA, Franco GP. Estado cognitivo e condições de saúde de idosos que participam de grupos de convivência. Rev Gaúcha Enferm. 2012; 33(4): 64-71.
- Melo DM, Barbosa AJG. O uso do Mini-Exame do Estado Mental em pesquisas com idosos no Brasil: uma revisão sistemática. Ciência e Saúde Coletiva. 2015; 20(12): 3865-76.
- Oliveira JMM, Nóbrega MML, Oliveira JC. Diagnósticos e resultados de enfermagem para a pessoa idosa institucionalizada: pesquisa metodológica. Online Braz J Nurs (Online) [internet]. 2015 [Cited 2016 Mar 23] 12(2). Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/5151/html_679.
- Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr. 2003; 61(3B): 777-81.
- Del Duca GF, Silva SG, Thumé E, Santos IS, Hallal PC. Indicadores da institucionalização de idosos: estudo de casos e controles. Rev. Saúde Pública. 2012; 46(1): 147-53.
- Shah SM, Carey IM, Harris T, DeWilde S, Cook DG. Mortality in older care home residents in England and Wales. Age Ageing. 2013; 42(2): 209-2015.
- Terrera GM, Minett T, Brayne C, Matthews FE. Education associated with a delayed onset of terminal decline. Age Ageing. 2014; 43(1): 26-31.
- Piccinin AM, Muniz-Terrera G, Clouston S, Reynolds CA, Thorvaldsson V, Deary IJ, et. al. Coordinated analysis of age, sex, and education effects on change in MMSE scores. J Gerontol B Psychol Sci Soc Sci. 2013; 68(3): 374-90.
- Park MH, Kwon DY, Jung JM, Han C, Jo I, Jo A. Mini-Mental Status Examination as predictors of mortality in the elderly. Acta Psychiatr Scand. 2013; 127: 298–304.
- Francoa JG et. al. MMSE items that predict incident delirium and hypoactive subtype in older medical inpatients. Psychiatry Research. 2014; 220: 975–81.
- Tseng WJ, Hung LW, Lin J. Time Orientation and Visual Construction Subdomains of the MMSE as Independent Risk Factors for Hip Fractures. Orthopedics. 2013; 36(7): 869-76.
All authors participated in the phases of this publication in one or more of the following steps, in According to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the versión submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 03/29/2016 Revised: 06/22/2016 Approved: 06/29/2016