Reduction of pain in clients with autoimmune bullous dermatoses: evaluation by fuzzy logic
Euzeli da Silva Brandão1, Iraci dos Santos2, Regina Serrão Lanzillotti2
1Federal University Fluminense
2State University of Rio de Janeiro
ABSTRACT
Aim: To evaluate the intensity of the client’s pain with autoimmune bullous dermatoses, before and after the protocol of nursing care is applied to a client with autoimmune bullous dermatoses. Method: The data were treated using fuzzy logic. Results: when associating the implementation of the protocol with pain reduction in the 14 study subjects the following stand out: in T0, seven subjects presented high levels of pain, with a pertinence of 1.0; in T1, 24 hours after intervention, eight presented a low level of pain, with pertinences ranging from 1.0 and 0.75, and only one with high level of pain; in T2, only one remained with a high level of pain. Discussion: The use of analgesics prior to application of the protocol demonstrates that change in pain intensity was not influenced by use of medication, but rather by the implemented care. Conclusion: Based on the classifications of fuzzy logic, there was a significant reduction of pain levels, especially in the first 24 hours.
Descriptors: Nursing; Nursing Care; Dermatology; Pemphigus; Pain.
INTRODUCTION
Autoimmune bullous dermatoses (ABD) are diseases in which blisters and vesicles are the primary and fundamental types of skin and/or mucous membranes lesion. These dermatoses are due to the activation of the immune system against the organism’s own constituents; in this case, antibodies are produced against specific skin structures, considered autoantigens(1,2). These autoantigens can be located in intraepidermal or subepidermal regions, being indispensable to the identification of its location for the classification of the type of autoimmune bullous dermatose(1,2).
The intraepidermal autoimmune bullous dermatoses characterize the pemphigus. There are different types of pemphigus: vulgaris, foliaceous, drug-induced, herpetiformis, paraneoplastic, and by immunoglobulin A (IgA); the first two are considered as major(1,2,3).
Among the autoimmune bullous dermatoses subepidermal are the bullous pemphigoid, pemphigoid of the mucous membranes, gestational pemphigoid, dermatitis herpetiformis, dermatose by linear IgA and epidermolysis bullosa acquisita(1,2).
These skin disorders can be extremely debilitating, making nursing care a challenge justified by the complexity of the disease, vulnerability to complications, in addition to the disfiguring and painful nature of injuries(4).
Thus, the responsibility of the nursing professional with this clientele is emphasized, even in non-specialized units, where therapeutic resources, personnel, equipment, environmental and structural conditions are not always favorable(5).
In this sense, it is worth noting that the practice of nursing care among clients with immunoblotting dermatoses has demonstrated the importance of this care in the prevention and minimization of aggravation and recovery of those affected(4).
Among these aggravations, pain stands out; a subjective and personal experience associated with actual or potential tissue damage. In the skin, the pain is characterized by a multidimensional experience, being able to vary in sensorial intensity, besides suffering affective-motivational interferences. Described as the fifth vital sign by the American Agency for Research and Quality in Public Health and the American Pain Society, acute or chronic pain should be assessed and recorded from the client's admission(6).
Despite this fact, there is a shortage of nursing publications on the subject. The rare nursing literature approaches the disease without privileging the fundamental aspects of care (4,7), among them, actions that can be implemented to reduce pain. The dissemination of such knowledge raises the need for nursing research, with significant evidence levels, to direct the use of protocols and technologies(4,7).
Thus, alternatives were developed aimed at evaluating the client integrally, as a consequence of the practical application of knowledge produced over a period of ten years(8), in addition to performing nursing actions to relieve pain and reduce complications in those who have presented a medical diagnosis of autoimmune bullous dermatose (AIBD). For this, a nursing protocol was proposed and subsequently published to assist clients with pemphigus(9).
Thus, after the proposal was updated and enlarged this was presented in the “Nursing Care Protocol to the Client with AIBD (PCECDI – from the Portuguese “Protocolo de Cuidados de Enfermagem ao Cliente com Dermatoses Imunobolhosas”); the question is: what are the evidences of pain reduction in the client with AIDB before and after the application of this protocol? To consider this, the following objective was established: to assess the intensity of the client's pain with AIBD, before and after the application of PCECDI. This research was supported financially by CNPq.
METHOD
Almost experimental and interinstitutional study. In this case, it was identified the ethical and humanistic difficulty - to establish a control group with those with the same disease, but who wouldn’t benefit from an innovative nursing care that supposedly would promote the reduction of their. Thus, an alternative clinical trial design was used for a single, non-random group of the time series type. Measurements were taken with the participants before (T0), 24 hours after (T1), and one week after (T2). As there was no control group, each client was considered as their own control(10).
The study was conducted from June 2012 to April 2013, at the Pedro Ernesto University Hospital of the State University of Rio de Janeiro (HUPE/UERJ), at the Adventist Hospital of Pênfigo/Campo Grande/Mato Grosso do Sul (HAP/MS), and at the Hospital Antônio Pedro of the Federal University Fluminense (HUAP/UFF). The study was characterized as inter-institutional.
These research fields were selected by considering institutions that have dermatology wards, located in different Brazilian regions, or those that have beds specifically designed for this clientele, as in the case of HUAP/UFF.
For convenience, the study group was obtained by sampling(10), which included the following inclusion criteria: adult individuals with a diagnostic hypothesis or with a definitive diagnosis of active immunoblotting dermatosis, hospitalized in wards of the aforementioned institutions, in the period determined to carry out the research, regardless of a history of previous hospitalizations, gender, age group, and the use or not of systemic medication who, after understanding the objectives, risks and benefits of the research, agreed to participate. The following exclusion criteria were established: people on psychiatric treatment, disoriented in time and space, and who refused to participate in the research.
It is important to emphasize that the subjects were evaluated in an integral way, using a instrument validated by specialists(8). During this evaluation, the nursing diagnosis of pain was identified by the presence of defining characteristics according to NANDA-International(11). In patients with pemphigus vulgaris, evaluation of the extent of cutaneous and mucosal lesions was performed by an instrument also validated for this purpose, the cutaneous-mucosal involvement index of pemphigus vulgaris(12).
The data produced were treated using fuzzy logic(13). To evaluate pain intensity a form was elaborated based on the principles of this logic, which has a chromatic scale, with a white color, followed by shades of yellow, orange and red, corresponding to support the fuzzy sets(13,14).
The evaluation of pain favors the knowledge of its origin, considering emotional, motivational, cognitive and even personality factors. However, due to its subjectivity, no standard instrument exists for its objective measurement. Among the available methods to measure the perception/sensation of pain, there are those that evaluate only its intensity and/or severity, and are considered one-dimensional, using numerical/verbal and analogue-visual scales. In addition, there are scales that evaluate sensory factors and affective-emotional factors, which are considered multidimensional(15).
In this study, the chromatic scale was chosen, as it was considered that this would facilitate the understanding of the study subjects. Thus, each subject participant of this research marked a color corresponding to pain intensity at the three moments. An increase in color tonality meant greater intensity, and a reduction meant lower intensity. The group of fuzzy sets was used to evaluate the conditions of each subject in each of the three moments: during (T0), 24 hours after (T1), and one week after intervention (T2)(14).
In addition to the analysis of frequency distribution of the subjects regarding the pain attribute in the moments T0, T1 and T2, a detailed analysis was conducted regarding the attribute of linguistic terms (low, medium and high) with the respective pertinences, in the three moments when the measurements were made with the subjects.
Values related to the pertinences should be understood as an increasing scale in the range of zero to one(13,14). For example, if two clients were classified with the linguistic term “high” for the pain attribute, it should be observed the pertinence attributed to each of them because who obtain the highest level of pertinence should be considered in more intense pain situation.
The research was approved by the Committee of Ethics in Research of the Pedro Ernesto University Hospital/UERJ, according to the protocol 0258.0.228.000-11, meeting the norms of research with human beings, following Resolution 466/2012.
RESULTS
Due to the fact that these are rare diseases, the number of subjects who participated in the study is justified. Among them, nine had pemphigus vulgaris, two had pemphigus foliaceus, and three bullous pemphigoid, of which 11 clients were from HUPE/UERJ, two from HAP/MS and one from HUAP/UFF. Their ages ranged from 27 to 82 years, with 11 female subjects. Of 14, 12 patients presented a nursing diagnosis of acute pain from the following defining characteristics: expressive behavior, sleep standard disorder, observed evidence of pain, facial expression, protector gestures, position to avoid pain, and verbal report of pain.
Table 1 shows the moment T0 and the predominance of eleven clients who declared themselves with high and medium intensity pain; seven with high pain intensity and four with medium pain intensity. A noted expressive change in this condition occurred at moment T1, when only one subject declared himself with high pain intensity and eight declared low pain intensity. From moment T1 to T2 there was a predominance of subjects with low and medium pain intensity.
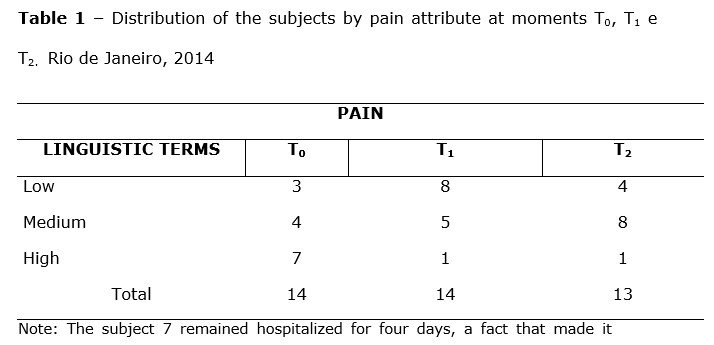
It should be noted that, of the three subjects who reported low intensity pain at moment T0, on Table 1, two had a medical diagnosis of pemphigus vulgaris, one female and one male, both 52 years old, and a mucosal cutaneous involvement index of pemphigus vulgaris of 30 and 40, respectively. The other subject had a medical diagnosis of bullous pemphigoid, and was elderly, with extensive exulcerated bullous lesions, distributed mainly in the upper and lower limbs.
A detailed pain analysis in relation to linguistic terms (low, medium and high), with respective pertinences at the three moments when the measurements were taken, can be visualized in Table 2. This shows that eight subjects presented a reduction of pain from the moment T0 to T1, and six remained in the same condition. From T1 to T2, three subjects experienced a reduced intensity of pain, but five reported an increase; four moved from low to medium intensity, and only one from low to high intensity of pain. The others remained in the same condition as in the previous period.
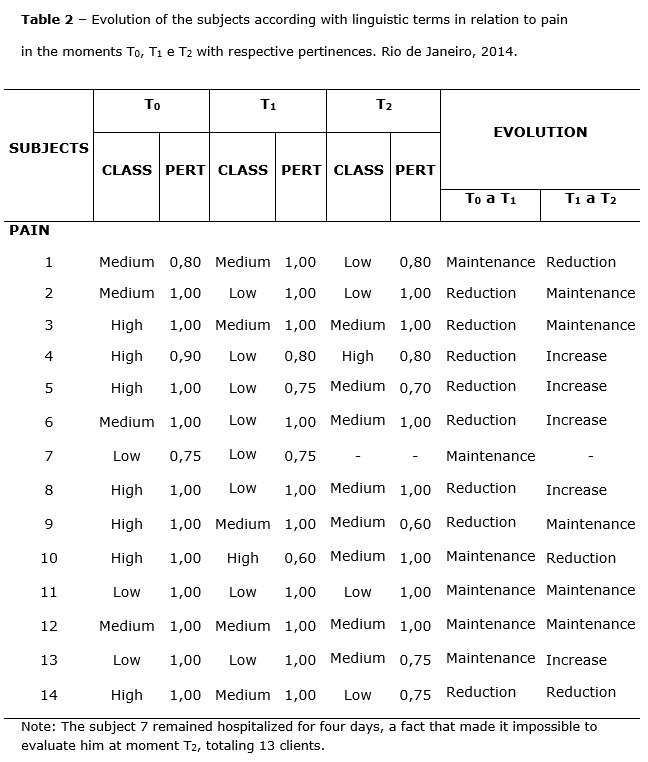
By associating the implementation of the PCECDI with pain reduction, highlighted in Table 2, at the moment T0, seven subjects presented high pain, with pertinence at 1.0. At the moment T1, 24 hours after the intervention, eight clients presented low pain, with pertinences ranging between 1.0 and 0.75, and only one with high pain. At the moment T2, only one subject remained with high pain.
DISCUSSION
Due to extensive lesions, normally presented by the study subjects, we consider relevant the change on the intensity of pain after the application of PCECDI. From the seven subjects who reported a high intensity of pain at moment T0, only one (subject 4) returned to this condition at moment T2. It is important to note that the same subject had a medical diagnosis of pemphigus vulgaris, with a maximum mucosal cutaneous involvement index(12) – MMCIIPV=100. When evaluated by the researcher, he had 16 days of hospitalization and did not respond to drug therapy.
Despite the increase in pain from the moment T1 to T2 in two subjects, the pain did not return to the high condition of moment T0, remaining in the condition of medium intensity, showing a positive evolution.
Regarding medications for pain relief, it is pointed out that four subjects, in their prescription, had an indication of the use of tramadol hydrochloride. Of these, three also had an indication of dipyrone for use in the presence of complaints. Five subjects had only an indication of dipyrone and five without indication of analgesic medication.
Tramadol hydrochloride is an opioid with a considerable central acting analgesic effect, indicated to relieve moderate to severe intensity pain of the acute, subacute or chronic type, with onset of action approximately one hour after administration. Depending on the intensity of the pain, the effect lasts from four to eight hours(16). Of the four clients who had a prescription for this analgesic, only two used 50mg intravenously every six hours. For the third subject, daily use was indicated only before the bath with a dose of 100 mg subcutaneously. For the fourth, the medication was prescribed for administration in the presence of complaints, being 50 mg orally. In the latter, an absence of check was observed, a fact that reveals that the medication was not administered during the period of the research.
Thus, it is worth mentioning that of the three subjects in the study using tramadol hydrochloride, only in two cases the use of medication can be considered a confounding factor in relation to the change in pain intensity during the research, since both interventions (Medication administration and PCECDI application) occurred concomitantly. In the case where the use of the medication was prescribed at the dose of 100 mg subcutaneously before the bath, it is important to note that the client had already been hospitalized for 16 days and was receiving the medication, thus, it was possible to evaluate the change in pain intensity from the nursing interventions.
Of the eight subjects who had dipyrone in their prescription, six indicated their use in the presence of complaints. Only two subjects presented prescriptions with an indication of regular use every six hours. Of these, one used the medication concomitant to the beginning of the research, another one used it before, i.e. 24 days before the beginning of the nursing interventions. The use of this medication regularly, and before the beginning of the nursing actions proposed in the PCECDI, demonstrates that the change in pain intensity, in this specific case from high to low in the first 24 hours after interventions, was not influenced by the use of the medication, but of the care taken. This fact can also be considered in relation to the five subjects who did not present in their prescriptions the indication of analgesic medications.
CONCLUSION
Based on the fuzzy logic classifications, a significant reduction of pain was observed, especially in the first 24 hours. This was mainly attributed to the application of the dressing proposed in PCECDI, which promotes the maintenance of a wet environment, avoiding the dryness of the bed of the lesions, besides preventing adhesion of the same ones in personal clothing and bedding. As pain reduction occurred, they increased mobility and sleep pattern, providing greater comfort and client disposition for self-care and coping with the disease.
The evidence points to the truth of the hypothesis formulated: PCECDI contributes to the reduction of pain in clients with AIBD, bringing a significant impact on the practice of care.
REFERENCES
- Hanauer L, Azulay-Abulafia L, Azulay RD, Azulay DR, Azulay RD. Doenças vesicobolhosas. In: Azulay RD, Azulay DR, Azulay-Abulafia L. Dermatologia. 5ª ed. Rio de Janeiro: Guanabara Koogan; 2013. p. 145-61.
- Carvalho CHP, Vieira CC, Santos PPA, Santos BRM, Lima ENA, Freitas RA. An epidemiological study of immune-mediated skin diseases affecting the oral cavity. An Bras Dermatology. 2011;86(5):905-9.
- Gonçalves GAP, Salathiel AM, Alves D, Britto MMC, Ferraz TS, Roselino AMF. Incidence of pemphigus vulgaris exceeds that pemphingus foliaceus in a region where pemphigus foliaceus is endemic: Analisis of a 21-yer historical series. An Bras Dermatology. 2011;86(6):1109-12.
- Brandão ES, Santos I dos. Evidences related to the care of people with pemphigus vulgaris: a challenge to nursing. Online Braz J Nurs [internet] 2012 Sept [cited 2016 jan 27];12 (1): 162-77. Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/3674. doi: http://dx.doi.org/10.5935/1676-4285.20133674.
- Santos I dos, Brandão ES, Clos AC. Dermatology nursing: sensitive listening skills and technology for acting in skin care. Rev enferm UERJ. 2009; 17(1):124-30.
- Bottega FH, Fontana RT. Pain as the fifth vital sign: use of the assessment scale by nurses in general hospital. Texto contexto enferm. 2010;19(2):283-90.
- Brandão ES, Santos I dos, Carvalho MR, Pereira SK. Nursing care evolution to the client with pemphigus: integrative literature review. Rev Enferm UERJ. 2011; 19(3):479-84.
- Brandão ES, Santos I dos, Lanzillotti RS. Validation of a instrument to assess patients with skin conditions. Acta Paul Enferm. 2013; 26(5):460-6.
- Brandão ES. O cuidar do cliente com pênfigo: um desafio para a enfermagem. In: Brandão ES, Santos I dos. Enfermagem em dermatologia: cuidados técnico, dialógico e solidário. Rio de Janeiro: Cultura Médica; 2006. p. 109-30.
- Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Delineando a pesquisa clínica: uma abordagem epidemiológica. 3.ed. Porto Alegre (RS): Artmed;2008.
- Diagnósticos de Enfermagem da NANDA: definições e classificação 2012-2014/ [NANDA International]; Porto Alegre: Artmed;2013.
- Souza SR, Azulay-Abulafia L, Nascimento LV. Validação do índice de comprometimento cutaneomucoso do pênfigo vulgar para avaliação clínica de pacientes com pênfigo vulgar. An Bras Dermatol. 2011; 86(2): 284-91.
- Zadeh LA. Fuzzy sets. Inform Contr. 1965;8:338-53.
- Brandão ES, Santos I dos, Lanzillotti RS, Moreira Júnior A. Proposal for recognition of the comfort pattern in clients with pemphigus vulgaris using fuzzy logic. Rev Esc Enferm USP. 2013; 47(4):958-64.
- Sousa FAEF. Pain: the fifth vital sign. Rev Latino-am Enfermagem. 2002;10(3):446-7.
- Ministério da Saúde. Consultoria Jurídica. Advocacia Geral da União. Nota Técnica 129/2012. On line [Internet]. 2012 [cited 2015 Dez 01]. Avaiable from: http://portalsaude.saude.gov.br/portalsaude/arquivos/pdf/2012/Dez/12/tramadol.pdf
All authors participated in the phases of this publication in one or more of the following steps, in According to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the versión submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 01/28/2016 Revised: 11/03/2016 Approved: 11/04/2016