Figure 1. Thematic scheme of the research by category, prepared by the authors. Rio de Janeiro, 2014.
ORIGINAL ARTICLES
Perception of nurse midwives regarding their professional identity: a descriptive study
Marina Caldas Nicácio1, Andressa Lohan dos Santos Heringer1, Mariana Santana Schroeter1, Adriana Lenho de Figueiredo Pereira1
1State University of Rio de Janeiro
ABSTRACT
Aim: To describe the similarities and differences between the professional practice of nurse midwives in the birth center and in the hospital, identifying whether the specifics of this practice influence the perception of their professional identity.
Method: This was a descriptive, qualitative research conducted with nurse midwives in a birth center and a maternity hospital in the city of Rio de Janeiro. The interviews were analyzed using the thematic content analysis technique.
Results: Two categories were established: similarities and differences in professional practice, and perceptions of professional identity: acts of belonging and assignment.
Discussion: Professional socialization was determined by experiences in the limited scope of nursing. Perceptions of the professional identity do not change because the place of performance is the hospital or birth center.
Conclusion: The different characteristics of these institutions do not influence perceptions of the professional identity of nurse midwives.
Descriptors: Obstetric Nursing, Professional Practice. Nursing care.
INTRODUCTION
The hospital is the main scenario of the professional practice of nurse midwives in normal birth care in Brazil. The birth center is a public health institution that is physically distanced from the hospital. Nurses take full responsibility for the institution and there are no doctors in the team of professionals. In situations of maternal, fetal or neonatal risk, patients are transferred to the main maternity hospital.
The institutional characteristics of the birth center involve facilitating the development of professional autonomy and the possibilities of nursing care(1). In the hospitals, nurses experience professional conflict and obstacles to providing humane care due to the predominance of the biomedical model in care routines and actions centered on the physician. Despite governmental initiatives to increase the performance of these professionals in the country, the specialized qualification required still needs improvement in order to overcome the influences of this existing model and play an active role in transforming the prevailing obstetric model(2).
In addition to these weaknesses, there are frequently "accumulation" or "change-of-function" issues that challenge the professional practice of nurse midwives, such as relocation to other nursing functions in the institution, which causes work overload, frustration, demotivation, conformism, and submission. This set of factors has been listed as one of the possible causes for the development of a hybrid professional identity: a mix between "being a nurse" and "being a midwife", which is often cited as one of the reasons why these nurses experience obstacles to performing their specific duties in hospitals(3).
The sociologist Claude Dubar(4) suggests that the construction of the professional identity is inseparable from plans for training and employment and various professional relationships. This is not just about identities at work, but forms of identities within which training is as important as work and corporate knowledge is as structural as the actor's position. Identity is detached from the way workers express this interaction.
Identity and difference are strictly dependent on representation, a form of attribution of meaning and a meaning-making process. This process is influenced by history and culture; norms, traditions, and rules of the institutions; speech or dialogue with other actors in the professional field and experiences in affiliation groups. Thus, this identity construction is formulated and reformulated in response to social interaction in a particular professional context(5).
Identity is set in the perception of itself (real identity) and of what is assigned or proposed by others (virtual identity); that is, the acts of belonging and attribution are the result of continuous and constant movement in the socialization process, both that which arises from the personal trajectory (biographical) and from social interactions during training and work (relational). Thus, despite the sense of individuality, identity is correlated to the context of work, to everyday experiences, interaction and recognition of other social actors(4).
In order to identify himself, the individual uses acts of belonging, that is, meaning categories that express "what kind of man or woman you want to be." The virtual identity is defined by a relational process and the categories that define what kind of man or woman you are; that is, the attribution acts(4).
From this perspective, the experiences of nurse midwives in their professional practice can be differentiated when they exercise their labor activity in an environment with unique and distinct features, for example, the birth center and the hospital. As a result, the meanings of their professional identities in these situations can also be differentiated. Considering this presupposition and the theoretical concepts described above, the following question was established: do the specifics of the professional practice of the nurse midwife in the birth center and the hospital influence the perception of their professional identity? To answer this question, the current research was developed, aiming to describe the similarities and differences between the professional practice of nurse midwives in the birth center and the hospital, and identifying whether the specifics of this practice influence the perception of their professional identity.
METHOD
This work uses a descriptive and qualitative approach. The research was conducted in a maternity home and a hospital; both institutions belong to the public health network and provide an environment for service education for obstetrical nursing residents.
The hospital was a municipal maternity hospital, which primarily serves women whose obstetric profile is classified as normal risk. In 2011, nurses at the hospital attended 1,384 live births (LB) by normal delivery, corresponding to 47.1% of the 2,937 births performed vaginally. Whilst the research was being conducted, the institution had 11 nurse midwives, a diarist, and 10 physicians on duty distributed across day and night shifts.
In the birth center, there are currently 18 nurse midwives, and two day laborers who exercise managerial positions and the vice direction of the institution. The other nurses are selected for day and night shifts to provide care to women and families in the prenatal, normal delivery and postpartum and newborn infants whose evolution progresses within the physiological parameters. In 2011, a total of 215 LB were assisted.
The nurse midwives participating in the study were randomly selected: an active nurse was interviewed on each day shift, shifts from Monday through Friday, at both institutions. At the hospital, all five duty nurses were interviewed. On one of the day shifts, the nursing staff was incomplete since there was only one professional present. The same quantity of interviews was carried out in the birth center.
The inclusion criteria were as follows: a nurse midwife working in direct assistance to normal childbirth, regardless of employment bond. Exclusion criteria were as follows: nurse midwives who worked in this role, but also filled the position of head of the obstetrical center or direction of the institution.
Interviews were conducted in-depth from July to August 2012. We used an interview guide consisting of 30 open questions. The first part of this instrument consisted of questions relating to training and professional career; in the second part, the issues were related to professional practice in obstetric nursing in the investigated institutions.
The interviews were analyzed using thematic content analysis, which outlines the following stages: 1) pre-analysis; 2) material exploration and treatment of results; and 3) inference and interpretation. To preserve the anonymity of the participating nurses, a code was adopted to refer to the place where the obstetric nurses exercise their professional activity and they were numbered in the order of the interviews: Birth Center N1, Hospital N2, and so on.
The study was approved by the Council of Ethics in Research of the Municipal Health Secretariat of Rio de Janeiro (SMS-RJ), opinion No. 316A/2011.
It is noteworthy that the study has limits in terms of the scope of its results on perceptions of the group investigated and, therefore, the distinctive characteristics of the practice of nurse midwives in the profession in particular and bounded contexts.
RESULTS
The average age of the 10 interviewed nurses was 42.5 years, ranging from 28 to 51. In relation to the time they graduated in nursing, two nurses had been graduated for less than 10 years, three nurses for 17 years, and five had 20 to 30 years of experience. The average period of working in obstetrical nursing was 15 years, ranging from 4 to 27 years. Six nurses obtained their titles through qualifications in obstetrical nursing, and the others through lato sensu post-graduation.
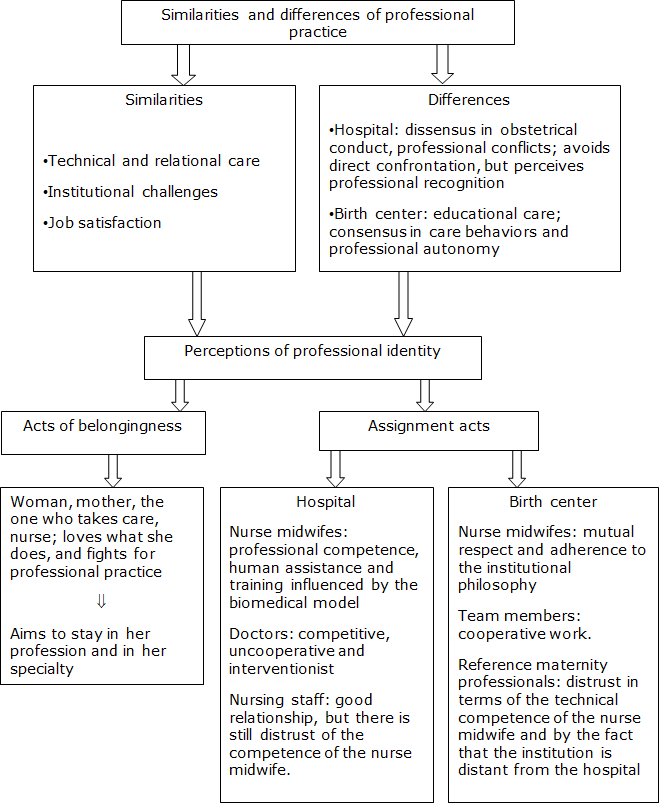
The analytical path generated two thematic categories: the first was Similarities and differences in professional practice, and the second was Perceptions of professional identity: acts of belonging and assignment.
Similarities and differences in professional practice
The common features of professional practice are the performance of care, typified as technical care, obstetric nursing techniques and procedures, and relational care such as attitudes of welcoming, listening, talking, supporting, encouraging the participation of the companion, and the link between mother and baby. It was only in the birth center that we had the opportunity to set up recording units related to educational activities, undertaken in individual sessions and with groups of pregnant women.
The nurses mentioned factors involved in professional practice, such as work overload, high demand for care for the limited number of professionals, and the accumulation of functions in both institutions, as expressed by the following statements:
Three activities have emerged in the shift: a labor, a prenatal consultation, and a transfer to the hospital. I said I would handle the transfer and the other colleagues wanted me to do other tasks. (Birth Center N4)
] Sometimes the [delivery] room is used as an office. When we have women hospitalized in labor and postpartum, the prenatal consultations get delayed. (Birth Center N3)
] We have to do several things and also the part that is the nursing’s responsibility in the obstetric center. (Hospital N6)
] With the antepartum full department, you can’t provide individualized attention. You have to meet this [woman in labor] first and then the other one. Sometimes you have to give attention to all at the same time. (Hospital N8)
The work at the hospital was characterized by disagreement over the conduct of obstetric care and the limitations of professional autonomy, as can be seen in the following statements:
You learn something in terms of [humanized care] theory, which can be applied. But it is very complicated to use; it is a constant struggle. (Hospital N9)
] If you need to apply oxytocin because labor is taking too long, is not evolving, you apply it and ask the doctor to prescribe it. [...] At the same time, when [the pregnant woman] arrives from the admission department, she already comes with oxytocin prescribed, and you cannot avoid it. So this lack of autonomy is what bothers me. (Hospital N7)
] When we came to the delivery room, we were the “Indian shaman". [...] (Hospital N9)
Despite this confrontational environment, there is a consensus in terms of professional practice acknowledgment:
They [doctors] recognize my work as valid and confident. (Hospital N8)
The birth center differs from the hospital. The care behaviors are established by consensus and there is freedom of action, as mentioned in the following statements:
Everyone follows the same [care] protocol. If we need to change something, we discuss until we find the best solution. (Birth Center N1)
] There is a freedom of action, of being able to implement, create, experiment, and encourage active labor. (Birth Center N4)
] Here we have an autonomy that I think no one has. (Birth Center N5)
Perceptions of professional identity: acts of belonging and assignment
Acts of belonging are related to perceptions about oneself, a person’s own identity. In both institutions, the interviewees stated that they are women and nurses who perform care. Such perceptions can be observed in the following statements:
I am a daughter, a mother, a wife and a nurse. (Birth Center N4)
& ⒯…] A nurse, a woman and mother of two children. (Hospital N8)
I'm the same nurse I've always been. For me, caring is the most important. So I am a caregiver. (Hospital N7)
Assignment acts develop from social relationships with other subjects. In the birth center, the nurse midwives perceive themselves as professionals who share the same vision about the care model and struggle to overcome the adversities of the profession:
We look like a big family. This facilitates everything; we speak the same language. The purpose and the end are the same. (Birth Center E4)
[...] Being here means breaking various barriers and facing various situations. (Birth Center E3)
[...] You have to prove that you know all the time; show that you know what you're doing (Birth Center E1)
[...] We have trouble even with our class [nursing]. Many do not accept our way of working [at the birth center]. We don't have difficulty in dealing only with the doctor. [...] So far we have managed to win great battles and we say that "we kill a lion a day." (Birth Center N5)
At the hospital, the nurse midwives consider themselves a distinct group due to the paradigmatic tendency of the training they had in their specialty and the distrust they face with regard to their professional competence:
We have several types of nurse midwives here. A group that began in biomedical vision and suddenly was placed in the world of physiological [delivery]. And there is that group that has already learned in this more humane, more physiological model. (Hospital N7)
[...] Some professionals [physicians and nurses] do not believe in the work of obstetric nursing. When we do our work, they see that it works, that it is possible. Then it becomes a little easier for us to cope with. [...] If you do not believe, you give up. So it's not an easy profession. (Hospital N6)
Because, well, of the 40 something doctors that we have here, you can risk 10, a fourth, that respects you as a professional. So it's a very difficult team to work with because the competition is too intense; the competition for power, of who gives more orders. So it's difficult. (Hospital N8)
Despite these difficulties experienced, all the nurse midwives interviewed expressed a desire to remain in the profession and in the specialty.
This set of results was synthesized in the thematic scheme of the research presented in Figure 1.
|
Figure 1. Thematic scheme of the research by category, prepared by the authors. Rio de Janeiro, 2014. |
DISCUSSION
The experiences lived by the subjects involve a process that is dynamic, individual and collective, subjective and objective, biographical and structural, and resulting from the socialization process, which expresses the culture, the roles, values and other meanings that determine their identity(4).
Care is an existential, relational and contextual phenomenon that involves ethical attitudes and humanist values. In the specific field of nursing, care is regarded as the essence of the profession(6) and the epistemic center in the theory and practice of the area(7). Nurse midwives express these theories about themselves as a distinctive way of being, knowing and acting within the health professions.
One study of nursing practice in the obstetric center has identified that there is work overload due to the increased demand for care and the lack of professionals, which causes physical exhaustion, psychological distress, and job dissatisfaction(8). These work characteristics are observed in all areas of operation of the nursing staff, and are related to the influence of political cost containment and the limitation of public resources for health(9).
There are also gender inequalities in everyday relationships of nursing work, which underlie professional conflicts and power struggles in the hospital. One study found that nurses have increased workload compared to their working time. These professionals have higher stress rates, fatigue and work overload than their male counterparts(10).
It is noteworthy that the birth center nurses also described excessive workload in terms of care demand, revealing that they have common issues regarding work in the hospital. However, the fact that this institution is a female dominated environment, where care is managed and conducted by nurses, can lead to more symmetrical working relationships since there is not the same gender division of labor observed in the hospital. The singularities of nursing work at the birth center should be investigated further.
As women nurses in the field of obstetrics, professional socialization has been influenced by the historical process of this particular field. Since the beginning of civilization, daily care has been allocated to women. Female participation has also been crucial in the history of patient care and nursing, as well as in obstetrics, which was particularly marked by feminine home care.
Throughout the twentieth century, Brazilian obstetrics suffered from the progressive process of institutionalization. The hospital began to prevail as the labor and birth environment in the country from the 1940s, represented as a symbol of modernity, civility, and social advancement at this time. This process was consequent to the regulation of the state on maternal and child health, which boosted the supply of public and insurance medical services for prenatal care and childbirth in the country(11).
The professionalization of the nurses interviewed had occurred exclusively in the field of nursing and their move to obstetrics was in the context of hospital care of the 1990s, which was already under the influence of the Humanization of Childbirth social movement. Considering that midwifery training was interrupted in the last decades of the twentieth century and only resumed from 2005(3), it is assumed that nurses had no interaction with the professionals in the workplace. Therefore, the professional socialization of the interviewees was clearly marked by the labor field of nursing.
It is important not to confuse socialization with schooling. Blurring the two does not help to understand the mechanisms of building oneself by means of work activity. Work can provide training, can be a source of experience, of new skills and knowledge for the future, but it is also under the influence of the vicissitudes of the economic system, cultural traditions, and the social policies of each country(4).
In this sense, the work experience of nurses participating in the study was confined to public institutions of obstetric care, where the political, legal, and organizational planning is under the auspices of the health policy of the Brazilian state.
The results suggest that the hospital is the most difficult environment for the professional practice of obstetric nursing, where the intervention procedures and biomedical technologies are most valued and doctors are the most influential professionals in the conduct of care. This setting adversely influences the performance of midwives and nurse midwives in comparison to the home space and normal birth centers(12).
At the hospital, there is a tendency to adopt a more interventionist approach and apply restrictions in terms of the decision-making of the hospital professionals, which has caused criticism from recent social movements of women and the search for other environments for the birth of their children(13-14).
The birth center is found to be a better place for the nurses to exercise autonomy in the conduct of obstetric care. This ability to use their knowledge and skills to assess and meet the needs of customers determines the perception of autonomy(15). However, the nurses in the birth center experience professional challenges similar to those reported by hospital nurses, such as conflicts between the care model that they seek to adopt and the hegemonic obstetric model in the health system, as well as the perception of mistrust of health professionals in terms of their professional competence.
Such problems are similar to those experienced by other nursing professionals in general, relating to having little social visibility, limitations in terms of professional autonomy and low recognition of the scientific basis of the profession(16). Despite this problem, the nurses interviewed manifest coping attitudes and struggle to overcome these challenges.
It should be noted that some nurse midwives consider that their expertise is recognized by the medical team at the hospital. This fact may denote that the obstetrical field is undergoing a paradigmatic transition in knowledge and care practices, which advances towards the principles of humanization and "medicalization" of normal delivery assistance. With this advance, the modification of social relationships are enhanced through more symmetrical relationships between the professionals and the women, and between doctors and nurses(17).
The struggle of these nurse midwives to ensure their professional practice in obstetrics and the implementation of humanized care has been investigated in national and international scientific literature(18-19-20). This literature deals with the transformations of public policies in obstetrics and the resulting impact on the inclusion of such professionals in the labor and birth scenarios, as well as the strategies adopted to overcome the challenges and constraints faced in the obstetrical service in the country.
Study participants identified themselves as nurses and they had significant experience in the framework of nursing and the Brazilian health system. Whether it occurs in the hospital or at the birth center, labor practice is related to the public health system, which is the locus of the construction of personal and collective subjectivities in the professionalization process of Brazilian obstetric nursing.
CONCLUSION
The professional experience of nurse midwives is marked by socialization in the limited scope of nursing and perceptions of their professional identity are not differentiated based on whether their work place is the hospital or the birth center.
The hospital remains an institution organized under rational logic and determining the persistence of powerful symbolic structures of the hegemonic obstetric model, which hinders the process of changing care behaviors and limits the autonomy of the obstetrics nurses in performing their unique care.
The birth center is not configured as an idyllic setting of professional practice. Although nurses consider that they have autonomy in the conduct of care in the birth center, there are challenges and consequent professional boundaries to these symbolic structures, that is, the prevailing common perception that this care space is unsafe for the health of mothers and their babies.
Nurse midwives perceive themselves as nurses, regardless of where they exercise their profession and specialty, which indicates that their professional identity is constructed during their training and demarcated by its trajectory in nursing exercise.
It should be noted that the study results in this work are not generalizable and they reveal meanings constructed by a group that is part of a specific care context. However, they contribute to revealing a set of meanings and values resulting from social and professional relationships and can provide support for future research on professional practice in obstetric nursing, especially in different areas of the hospital.
REFERENCES
1. Zveiter M, Souza IEO. Solicitude constituting the care of obstetric nurses for women-giving-birth-at-the-birth-house. Esc. Anna Nery. 2015; 19(1): 86-92.
2. Gualda DM, Narchi NZ, de Campos EA. Strengthening midwifery in Brazil: education, regulation and professional association of midwives. Midwifery. 2013 Oct;29(10):1077-81.
3. Costa AANM, Schirmer J. A atuação dos enfermeiros egressos do curso de especialização em obstetrícia no nordeste do Brasil: da proposta à operacionalização. Esc. Anna Nery. 2012; 16(2): 332-39
4. Dubar C. A construção de si pela atividade de trabalho: a socialização profissional. Cad. Pesquisa. 2012; 42 (146):351-67
5. Cardoso MIST, Batista PMF, Graça ABS. A identidade do professor: desafios colocados pela globalização.Rev Bras Educ. 2016;21(65): 371-90.
6. Piérrez AHF, Merighi MAB, Muñoz LA. Perceptions and expectations of nurses concerning their professional activity. Acta Paul Enferm. 2013; 26(2):165-71
7. Sebold LF, Carraro TE. Modos de ser enfermeiro-professor-no-ensino-do-cuidadode-Enfermagem: um olhar heideggeriano.Rev Bras Enferm. 2013; 66 (4): 550-56
8. Copelli FHS, Oliveira RJT, Erdmann AL, Gregório VRP, Pestana AL, Santos JLG. Understanding nursing governance practice in a obstetric center. Esc. Anna Nery. 2015;19(2):239-45.
9. Umann J, Guido LA, Silva R. Stress, coping and presenteeism in nurses assisting critical and potentially critical patients. Rev Esc Enferm. USP. 2014;48(5):891-98.
10. Pereira AV. Nurses' daily life: gender relations from the time spent in hospital. Rev Latino-Am Enfermagem. 2015;23(5): 945-53.
11. Leister Nathalie, Riesco Maria Luiza Gonzalez. Childbirth care: the oral history of women who gave birth from the 1940s to 1980s. Texto Contexto Enferm. 2013 Mar; 22(1):166-74.
12. Bourgeault IL, Sutherns R, Macdonald M, Luce J. Problematising public and private work spaces: midwives' work in hospitals and in homes. Midwifery. 2012;28(5):582-90
13. Everly MC. Facilitators and Barriers of Independent Decisions by Midwives During Labor and Birth. J Midwifery Womens Health. 2012;57(1):49–54
14. Sanfelice CFO, Shimo AKK. Home childbirth: progress or retrocession? Rev Gaúcha Enferm. 2014;35(1):157-60
15. Alidina K. Professionalism in post-licensure nurses in developed countries. J Nurs Educ Practice. 2013; 3(5): 128-37
16. Avila LI, Silveira RS, Lunardi VL, Fernandes GFM, Mancia JR, Silveira JT. Implications of the visibility of professional nursing practices. Rev Gaúcha Enferm. 2013;34(3):102-109
17. Gomes, Maysa Luduvice; Moura, Maria Aparecida Vasconcelos; Souza, Ivis Emília de Oliveira. Obstetrical practice by nurses in institutional childbirth: a possibility for emancipatory knowledge. Texto Contexto Enferm. 2013;22(3):763-71
18. Oliveira AS, Damasceno AKC, de-Moraes JL, Moreira KAP, Teles LMR, Gomes LFS. Technology used by companions in labor and childbirth: a descriptive study. Online braz j nurs [ Internet ]. 2014 March [ Cited 2015 Mar 28 ] 13 (1): 36-45. Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/4254.doi:http://dx.doi.org/10.5935/1676-4285.20144254
19. Pereira ALF, Moura MAV. Proceso de implementación de la Casa de Parto en el Sistema Unificado de Salud, Rio de Janeiro, Brasil. Av Enferm. 2012;3(3):29-36
20. Vargens OM, Silva AC, Progianti JM. Non-invasive nursing technologies for pain relief during childbirth--the Brazilian nurse midwives' view. Midwifery.2013;29(11):e99-e106.
All authors participated in the phases of this publication in one or more of the following steps, according to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial participation in the planning or preparation of the manuscript or the collection, analysis or interpretation of data; (B) elaboration of the work or performance of critical review of the intellectual content; (C) approval of the submitted version. All authors declare for any purposes that the content related to all aspects of the manuscript submitted to OBJN is their responsibility. They ensure that the issues related to the accuracy or completeness of any part of the article have been properly investigated and resolved; thus exempting the OBJN of any joint participation in any imbroglios on the matter at hand. All authors declare that they have no conflict of interest, whether financial or relationship, to influence the drafting and / or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_final_13-06-2013.pdf
Received: 10/04/2015
Revised: 05/20/2016
Approved: 05/22/2016