ORIGINAL ARTICLES
Physical Fitness and quality of life of the elderly: a transversal study
Tauan Nunes Maia1, Edmundo de Drummond Alves Junior1, Julianne Quinellato Louro1, Elciana de Paiva Lima Vieira1, Jonas Lírio Gurgel1
1Fluminense Federal University
ABSTRACT
Aim: To evaluate the association between the quality of life and performance in physical fitness tests.
Method: This is a study adopting a quantitative and transversal approach, with a group of elderly residents living in the Souza Soares and Beltrão slum communities.
Results: The results demonstrate a general profile of elderly individuals who do not show any motor fragility, and a classification near to regular in terms of their quality of life index. To find this score, a WOOQOL-Bref questionnaire was used, together with the following tests: functional range; reaching the feet while seated, standing up and walking; standing up from a chair in 30 seconds. To analyze the data obtained, this research used the Saphiro-Wilk normality test, and the Spearman correlation test. For all the tests, the level of significance was established as α ≤ 0.05.
Conclusion: There is no correlation between quality of life and physical fitness with regard to the studied population.
Descriptors: Elder; Motor Activity; Physical Fitness.
INTRODUCTION
Today, it is evident that we are experiencing a demographic transition, leading to a change in age patterns in society. This transition occurs when there is a rise in life expectancy and a reduction in birth rates, thus leading to a possible inversion of the population pyramid. In Brazil, people 60 years of age or more make up 10.6% of the population. This high level generates worries related to the consequences of the process of aging on the part of the individuals (1-2).
Among the many opinions found in the literature, it is common to find chronologic references being used to support public policies(3). In some cases, in developed countries, the elderly are considered people aged 65 years or more; in developing countries, the benchmark is established at the age of 60 (3).
Aging is a dynamic, progressive and individual process, with morphologic, biochemical, functional and psychological modifications, which involve a reduction in the capacity of the adaptation of the individual to the environment(4). These losses, influenced by phenotype and genotype factors, increase the vulnerability of the elderly in terms of developing pathogen processes that can lead to death(5).
Within this context, such functional decline can negatively affect the quality of life of the elderly, in that it compromises both their autonomy and their independence. On many occasions, it develops into events which have a direct impact in the health of the elderly, such as accidents caused by falling. Therefore, quality aging in life, aimed at preserving as much of the functional capabilities as possible, is extremely important in terms of performing physical exercise(6).
Studies suggest there is an association between regular physical exercise and a higher aptitude for these physical exercises. While adopting such a routine, mortality rates and age-associated comorbidities tend to decline, which would lead to the idea that such activities increases the levels of quality of life(7,8). The number of studies that suggest that physical activity and physical fitness are related to quality of life has increased considerably in recent years, adding to these practices the capacity to rehabilitate and prevent illnesses.
As the result of a systematic review, it was found that authors synthesized and analyzed evidence in the literature related to the association between physical activity and quality of life(9). After examining 38 studies, the authors concluded that despite indicators that vary according to the chosen indexes of quality of life, the connection between the two is positive.
This scenario brings up the discussion regarding a decreased amount of physical activity, which can cause the individual to develop functional incapacities, reducing that individual’s quality of life. In this sense, tests of physical fitness can help to evaluate functional capacity, given that they are specific and work to measure and evaluate the physical variables that are related with the independence of the individual(10).
The routine practice of physical exercises extrapolates the physical benefits, as it has a direct connection with functional capacity, social interaction, emotional state, intellectual activity, self-care, the health state, and the cultural, ethic and religious practices of the individual(7). The project “Promotion of health for individuals above 50 years of age in the municipality of Niterói” (Brazil), based on a partnership between the Fluminense Federal University and the Municipality of Niterói, Brazil, works inside the slum communities of Souza Soares and Beltrão. Based on the fact that these areas have an estimated 1,200 elderly residents, and that until this moment has been no study involving this population, it is important to investigate their physical fitness and quality of life. Through this study it will be possible to reorient the health services provided to these individuals.
METHOD
This is a research project adopting a quantitative and transversal approach, linked to the project “Promotion of health in individuals above 50 years of age in the municipality of Niterói”, inside the slum communities of Souza Soares and Beltrão (in Niterói, Brazil), during 2012. A pilot-study was performed, with a population similar to the one studied, in which the methods and materials were tested. In both the pilot-study and in the current study, the evaluators were trained. All the volunteers who made up the sample group signed a consent agreement authorizing the research, according to the resolution 466/2012 of the Brazilian National Health Council. As a compromise with these individuals, the researchers kept the information regarding the identification of these individuals private. This research project was approved by the Committee of Ethics and Research of the Fluminense Federal University – College of Medicine (CEP – UFF - Protocol 265/2009).
The investigated communities were chosen because they are areas of work of the researchers who are involved in a regular program that promotes physical exercise, entitled “Healthy life in Niterói and São Gonçalo”. In order to support the recruitment of the sample, the study used the local printed press and a partnership with the local Family Physician program, later visiting the homes of the target population by accompanying the local community agents while disclosing the evaluations and proceedings that were to be adopted. The sample was build at the convenience of the individuals.
As criteria for inclusion, the individuals who were 60 years old or more that were present on the day of the analysis, and who did not present any physical, hearing, or visual impairment that prevented them from performing the tasks related to the evaluation were considered as being appropriate to participate in this research. In terms of criteria for exclusion there were the elderly who had any sort of illness that could compromise the performance of the physical tests; those who did not finish filling in the information required in the questionnaire; those who were diagnosed with Parkinson’s or Alzheimer’s disease, or even dementia; those wearing prosthesis on their lower limbs; or those with some sort of medical advice against the practice of any physical exercise.
The quality of life was evaluated based on a WOOQOL-Bref questionnaire which was filled in during the interviews. It is composed of 26 questions that involve physical and psychological areas, social relationships, and the local environment. The proceeding used for these interviews was that the researcher placed himself in front of the interviewee, and the this researcher read the questions and the alternative answers, word by word. If the individual did not understand the question, the researcher would explain the procedures again and reread the question and the alternative answers, in order not to influence the answer given.
The physical fitness of the elders was evaluated based on a set of physical tests, which were:
1) test of functional reach;
2) test of reaching the feet;
3) test of sitting, standing up and walking;
4) test of standing up from a chair within 30 seconds.
All tests were validated and classified according to the scores proposed by the researchers.
To perform the test of functional reach, a measuring tape placed horizontally on a wall at the acronym height of the person to be evaluated was used. Before the test started, the person being evaluated was placed 10cm away from the wall, with his feet in a parallel position and shoeless, in a comfortable position. The dominant superior limb was flexed at around 90º, elbow extended, wrist in a neutral position, and fingers extended. The test was designed to make the individual reach the furthest position possible, measured by the tape, without moving his heels off the floor, losing balance, or taking a step forward. Participants who left their original position had to redo the task. The result was registered in centimeters.
The material used in the test of reaching the feet was a chair 43.18 cm tall. The individual was asked to take a seat on the chair and then extend his legs, one at a time. At a sign, the individual had to flex his torso reaching his elbows to the extended knee as much as possible. In terms of results, the largest distance, between the toes and the tip of the middle finger was measured.For the test of standing up from a chair in 30 seconds (to evaluate the strength of the lower limbs), a chronometer and a chair with a backrest, or a hinged chair without armrests, 43.18 centimeters tall were used. With the chair against the wall, the individual sat with his back straight and feet flat on the floor and the arms were crossed on the torso. At the evaluator’s signal, the volunteer had to stand up to a full standing position and then return to the full seated position, as many times as possible, during a period of 30 seconds. The results were verified based on the number of repetitions within 30 seconds, compared to the reference values suggested by Rikli and Jones.
For the test that evaluated the participant’s agility and balance (tests of seating, standing up and walking), a foldable chair 43.18cm tall, a chronometer, a measuring tape and a cone were used.
The participant sat with one foot slightly ahead of the other and the body slightly inclined to the front. At a sign, the participant had to stand up and walk as fast as possible around the cone (placed 2.5 meters away) and then sit back on the chair. The time was recorded in seconds.
To analyze the data collected, a Shapiro-Wilk normality test was used to evaluate the normality of the sample. The correlation was done under the Spearman test. The results are presented in medians, interquartile intervals, and minimum and maximum values. The calculation was done using the GraphPad Prism software, version 5.0. The level of significance adopted to all tests was α ≤ 0.05.
RESULTS
29 individuals of both sexes were selected. They agreed with the investigative proposal and were in agreement with regard to the criteria of inclusion and exclusion. The age of the participants averaged 69.6±11.2 years. With regard to the environmental characteristics, the largest part of the elderly population of the studied slum communities lived on hills, and were thus used to going up and down stairs, and walking on steep and rugged terrain.
Table 1 presents the median distribution and the interquartile intervals related to the motor test produced. It is possible to see that the majority of the population studied achieved average performance results in the tests involving sitting and reaching the feet, and the test of standing up from a chair; in terms of the results of the test of standing up and walking, the results were above normal levels. The result of the evaluation of the test of functional reach demonstrated that the elderly included in the sample did not present any evidence of fragility.
Table 1: Distribution of the averages and standard deviations related to each motor test on the part of the residents of the slum communities of Souza Soares and Beltrão, Brazil, 2012. |
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
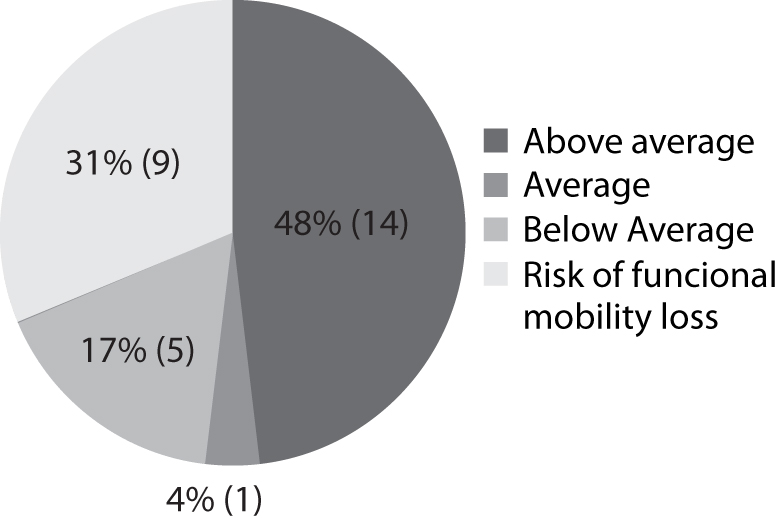
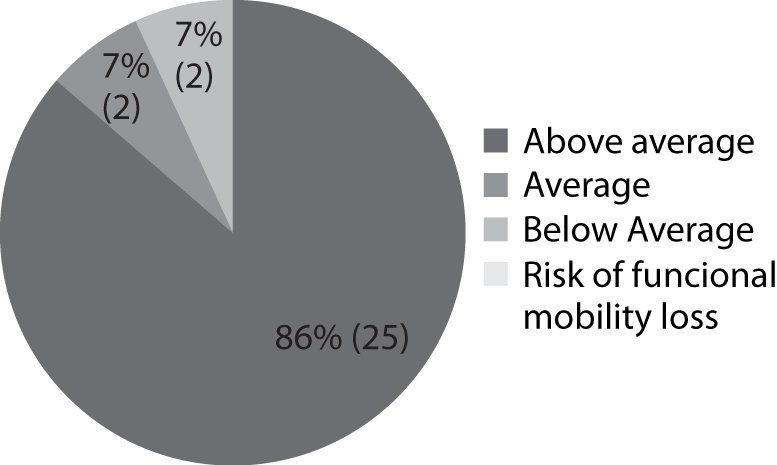
The results of the tests of standing up and walking, standing up from a chair over a 30 second period, and sitting and reaching the feet, are presented according to the classification developed by Rikli and Jones (2008) in Charts 1, 2 and 3, respectively.
| Chart 1: Result of the test of standing up and walking on the part of the residents of the slum communities of Souza Soares and Beltrão, Brazil, according to the relative classification based on the age of each individual, 2012. |
|
| Chart 2: Result of the test of standing up from a chair within a 30 second period on the part of the residents of the slum communities of Souza Soares and Beltrão, Brazil, according to the relative classification based on the age of each individual, 2012. |
 |
Chart 3: Result of the test of sitting and reaching the feet on the part of the residents of the slum communities of Souza Soares and Beltrão, Brazil, according to the relative classification based on the age of each individual, 2012. |
 |
The WOOQOL-Bref scores in each domain can vary from 0 to 100. The higher the score, the better will be the quality of life of the subject, as presented in Table 2. This table demonstrates the scores in terms of the domains. With these results, it is clear that the psychological and social domains presented both the highest and the lowest scores.
| Table 2: Distribution of the results of the sample related to each domain presented by the instrument WOOQOL-Bref, of the residents of the slum communities of Souza Soares and Beltrão, Brazil, 2012. | ||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
Source: the authors
Table 3 presents the information related to the association between the results of each motor test and each WOOQOL-Bref domain, as well as the relationship between each test and the general score of the estimated quality of life. It can be seen that there was no significant relationship between the motor tests and the self-reported quality of life.
| Table 3: Association between the motor tests, domains and quality of life estimated by the WOOQOL-Bref instrument of the residents of the slum communities of Souza Soares and Beltrão, Brazil, 2012 . | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This study aimed to evaluate the association between the quality of life and the performance of the physical fitness test in slum communities in the city of Niterói, Brazil. The results found show that the profile of the elderly that did not demonstrate any motor fragility. In the classifications generated, these subjects are on the average level, in terms of the test results with regard to standing up and walking. The average quality of life score was 60.2 points out of 100 points. Therefore, despite the good performance, the quality of life is near to what can be classified as normal. No correlation was found between the domains of the quality of life and the motor tests.
Some authors agree with the results of this present study, indicating that physical fitness is nor necessarily a determining factor with regard to the self-perception of the quality of life on the part of the elderly(12,13,14). One study evaluated the relationship between life, functional independence, and physical performance of the lower limbs in 125 elderly subjects. The researchers found that, despite a higher functional impairment, the elderly individuals presented a higher satisfaction with their lives(12). In another study, researchers have investigated the physical capacity and the self-perception of the quality of life of 340 elderly subjects between 65 and 80 years of age(14) and were able to see that, in people older than 70, the relationship between the mentioned variables was proportionally inverse, and in elderly subjects of up to 70 years, there was no correlation.
Together with the results found here, some other recent studies show that the reduction in physical capacity compromises the quality of life of the elders, as it directly influences the performance of routine tasks, besides the reduction of the speed of walking and autonomy(15,16,17). When studying the effect of functional training related to postural balance, functional autonomy and quality of life in 70 elderly subjects, researchers found that the improvement in body balance reflected in the quality of life of the subjects(18). As a confirmation to these findings, another study was able to point out in 42 people, there was a relationship between physical fitness and the quality of life indicators(15).
The definition of quality of life is complex, multidimensional and subjective, representing the views of the subject regarding what one considers as elements of a healthy life, or based on their views of the world, society, and the individual(17). Therefore, each person has a definition for leisure, health, well-being, and habits and lifestyle, varying according to social, economic, political, and cultural contexts(12,14). Another important factor is the correlation between the practicing of physical activity as a possible indicator of the quality of life(19). These elements are inherent to the data found in the definitions of self-perception of quality of life, as the studied population lives in a poor community filled with socioeconomic and cultural peculiarities, with limited access to leisure and health services.
In one piece of research, aimed at analyzing the possible associations between functional capacity and the level of quality of life of the elderly, some of whom had a regular routine of physical activities while some others did not share the same habit, the authors used a socio-demographic profile questionnaire, the WHOQOL-BREF, and a scale of self-evaluation of the functional capacity in 121 volunteers(19). These researchers observed that, with regard to the quality of life domain, the elderly who had a routine of physical exercise also presented better average results when compared to sedentary individuals, except for social networks. Only the variable described as the level of functional capacity achieved a favorable significant difference in terms of the group that had the habit of engaging in regular physical activity.
The geographical specificity of the slum communities of Souza Soares and Beltrão is an important issue that should be highlighted in order to understand the results achieved in this study. The homes of the researched individuals are built on steep hills, which demand strength and relative good fitness to move around. For this reason, the data obtained is based on good result in terms of motor tests, and it is possible that the elderly subjects were already in good physical shape on the day of the evaluation. Therefore, in the first instance, this study has not found any significant association between quality of life and functional capacity.
CONCLUSION
The results of this study show a lack of correlation between the quality of life and physical fitness with regard to the studied population. The evaluation is very complex and demands attention; however it is extremely important to understand the profile of this particular population. At the same time, it is necessary to highlight that this is the first study performed on this population. Therefore, it is suggested that the performance of new evaluations be undertaken based on these guidelines, in order to support the construction of specific actions to improve the health and well-being of the increasingly aging population of Brazil.
It is important to mention that the study was done using a small sample, one which does not represent the population in general. Consequently, this is a limiting factor. Another limiting issue is the bias present in terms of the intra-evaluator and the inter-evaluator, which can be worked on as much there are training sections to minimize them as much as possible. However, as this is a pioneer piece of research in terms of the specific population, it is important to better understand the factors that influence the quality of life and the functional capacity, and also to redirect the interventions already performed.
REFERENCES
1. Census Bureau (Unites States). International Programs 2013 [ Internet ]. [ Cited 2013 Jul 23 ]. Available from: http://www.census.gov/population/international/data/idb/region.php
2. Instituto Brasileiro de Geografia e Estatística (Brasil). Sinopse censo demográfico 2010. IBGE: [ s.l. ] 2011. [ Cited 2013 Jul 20 ]. Available from: http://www.ibge.gov.br/home/mapa_site/mapa_site.php#download
3. Almeida VFSM, Leite LS. Avaliação do Programa de Preparação para a Reserva e Aposentadoria do Comando da Aeronáutica. Meta: Avaliação. 2012; 4(12):232-249.
4. Marinho LM, Vieira MA, Costa SM, Andrade JMO. Grau de dependência de idosos residentes em instituições de longa permanência. Rev Gaúcha Enferm. 2013;34(1):104-110.
5. Gottlieb MGV, Schwanke CHA, Gomes I, Cruz IBM Envelhecimento e Longevidade no Rio Grande do Sul: um perfil histórico, étnico e de morbi-mortalidade dos idosos. Revista Brasileira de Geriatria e Gerontologia. 2011; 14(2):365-380.
6. Nascimento CMC et al. Exercícios físicos generalizados capacidade funcional e sintomas depressivos em idosos brasileiros. Revista Brasileira de Cineantropometria e Desempenho humano. 2013; 15(4):486-497.
7. Santana MS, Chaves EMM. Atividade Física e Bem-Estar na Velhice. Revista Salud Pública. 2009;11:225-36.
8. Livramento GA, Fagundes PPAN, Winter GR, Bernardes VP, Krause MP Estudo longitudinal do nível de atividade física de mulheres idosas. Revista Brasileira de Atividade Física e Saúde. 2012; 17(6):552-561.
9. Pucci GCMF; Rech CR; Fermino RC; REIS RS. Association between physical activity and quality of life in adults.Revista de Saude Publica. 2012; 46(1):166-179.
10. M. G. Maciel, Atividade física e funcionalidade do idoso. Motriz. Oct/Dec 2010; 16 (4): 1024-1032, Oct/Dec 2010.
11. Sposito G, D`Elboux MJ, Neri AL, Guariento ME. Satisfaction with life and functionality among elderly patients in a geriatric outpatient clinic. Revista de Ciencia e saude coletiva. 2013; 18(12): 3475-3482
12. Enkvist A, Ekstron H, Elmstahl S. What factors affect life satisfaction (LS) among the oldest-old? Arch Gerontol Geriatr 2012; 54(1):140-145.
13. Hernadez R, Fernádez L, Alonso O. Satisfaction with life to functionality in active elderly people. Acts Esp Psiquiatr 2009; 37(2):61-67.
14. Menêses A L; Lima AHRA; Farah BQ; et al Relação entre Aptidão Física e os Indicadores de Qualidade de Vida de Indivíduos com Claudicação Intermitente Rev Bras Med Esporte, 17(3), May/Jun 2011.
15. Prado RA; Egydio PRM; Teixeira ALC; Izzo P; Langa CJSO. A influência dos exercícios resistidos no equilíbrio, mobilidade funcional e na qualidade de vida de idosas. O Mundo da Saúde. 2010; 34(2):183-191.
16. Torres GV; Reis LA; Reis LA, Fernandes MH. Qualidade de vida e fatores associados em idosos dependentes em uma cidade do interior do Nordeste. J Bras Psiquiatr. 2009; 58(1):39-44.
17. Leal SMO; Borges EGS; FonsecA MA; Alves Junior ED; Cader S; Dantas EHM. Efeitos do treinamento funcional na autonomia funcional, equilíbrio e qualidade de vida de idosas. R. bras. Ci. e Mov 2009;17(3):61-69.
18. Carvalho ED; Valadares ALR; Costa-Paiva LH; Pedro AO; Morais SS; Pinto-Neto AM. Atividade física e qualidade de vida em mulheres com 60 anos ou mais: fatores associados. Rev Bras Ginecol Obstet. 2010; 32(9):433-40.
19. Sampaio PRC; Costa CLA. Capacidade funcional e qualidade de vida de idosos da cidade de Brejo Santo - Ceará. Rev Interfaces. 2013; 1(3):1-8.
All authors participated in the phases of this publication in one or more of the following steps, in According to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the versión submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 01/20/2014
Revised: 09/29/2014
Approved: 09/30/2014