ORIGINAL ARTICLES
Social representations of women in pregnancy, postpartum, and educational actions
Dafne Paiva Rodrigues1, Eryjosy Marculino Guerreiro1, Márcia de Assunção Ferreira2, Ana Beatriz Azevedo Queiroz2, Delano Franco da Costa Barbosa3, Ana Virginia de Melo Fialho1
1State University of Ceará
2Federal University of Rio de Janeiro
3Municipal Government of Caucaia
ABSTRACT
Aim: To understand the social representations of postpartum in terms of health education in pregnancy and childbirth.
Method: This is a descriptive study guided by the Theory of Social Representations, developed in nine Family Health Centers in Fortaleza, Ceará. The study subjects were users enrolled in one of these centers, in the postpartum period, older than 18 years, with at least six prenatal visits and a postpartum consultation. We used the Test of Free Association of Words.
Results: The primiparous women combine educational activities with family education. The multiparous women have in their evocations representations of health actions provided by the physician, courses and lectures.
Discussion: The multiparous women undergo a process of reframing of their experience after the consultations. Thus, scientific knowledge is emphasized and popular knowledge devalued.
Conclusion: We need to reframe educational actions that may be understood as a vehicle for knowledge construction, breaking the traditional design of transmission and reproduction.
Descriptors: Health Education, Nursing, Women, Pregnancy, Postpartum Period.
INTRODUCTION
Policies toward women's health have, over the years, emphasized the need to educate throughout the pregnancy and puerperium period as they are periods that are new, unique, and full of changes in women's and their family's lives.
In 1984, the Ministry of Health elaborated the Program for Integral Assistance to Women's Health (PAISM), which incorporated as principles and guidelines the proposals for decentralization, hierarchization, and regionalization of services, as well as the importance of comprehensive care and equity(1). However, one of the greatest criticisms of the program is that it was not actually regionalized, despite having been a landmark in the politics of women's health, mainly due to the feminist movement.
In 2000, the Ministry of Health established the Program for Humanization of Prenatal and Birth Care (PHPN), following the principles that were firstly presented in PAISM to ensure better care for women during pregnancy and childbirth, but adopting the concept of broader health. The PHPN brings with it the perspective of women as individuals responsible for their own health and the assurance of their reproductive rights, in which case the humanization of care is its main strategy(2).
Some years later, in 2004, another victory was achieved in the context of women's health by means of the National Policy for Integral Attention to Women's Health (PNAISM), which had as its guiding principles: health promotion, gender, and completeness. One of its goals was to promote the improvement of the living conditions and health of Brazilian women by ensuring legally established rights and expanded access to media and services for the promotion, prevention, care, and restoration of health in the whole territory(1).
This access has been expanded through the National Primary Care Policy in 2006, which proposed the creation of the Family Health Strategy (FHS), allowing the reorientation of the biomedical model, and through the National Policy for Health Promotion, which sets the operationalization of health promotion, taking as its object the problems and needs of health, and its determinants and constraints(3).
It is also worth highlighting the Stork Network, implemented through Ordinance No. 1459, which provides women with the right to humanized care during pregnancy and childbirth, as well as in all levels of care. This model of care during labor and birth was inspired by the classification of hospitals and the Carioca Stork Program, which seeks to reduce maternal and infant mortality and encourages prenatal consultations at the FHS, visits to maternity hospital, prenatal care, and the provision of transportation transport(4).
The FHS presents as its central idea an educational practice that aims to promote health through a set of activities focused on improving well-being conditions and access to goods and social services activities. It takes advantage of being allocated within the community where the service is provided, as well as being administered by a multidisciplinary team. In addition, the FHS also promotes health contextuality, comprehensiveness, and education in all the activities developed(5).
Thus, health education can be seen as an important tool to promote the emancipation of the subject, in the case that the individuals involved in the process understand it as the possibility of transformation and develop educational actions that foster the strengthening of autonomy.
Health education in pregnancy and childbirth involves the patients who have a key role, for being the center of the educational process, allowing the deduction of the existence of representations in this group. It is understood, therefore, that the form of expression of puerperal women in the educational process provides directions regarding health education during pregnancy and the postpartum period.
In this sense, the object of research is health education under the social perspective of the meanings, considering individuals as bearers of a knowledge that is socially constructed and shared by interaction(6).
The Social Representations Theory was adopted as a theoretical possibility capable of guiding the manner in which individuals act regarding reality—specifically the users of health education in pregnancy and childbirth—based on a system of values defined under the social influence.
To generate social representations, the object must have enough social or cultural relevance. It should be a phenomenon which represents the chosen social group. It should also be consistently involved in a group practice, detected in behaviors and communications that actually occur systematically(7). Therfore, understanding health education as a social phenomenon, the objective of this study is to understand social representations of postpartum women regarding health education in pregnancy and childbirth.
METHOD
This is an excerpt of the dissertation entitled "Social representations of postpartum women regarding health education in pregnancy and childbirth." The descriptive research is guided by a procedural approach of the Theory of Social Representations(6.8).
The study was conducted in nine Family Health Centers (FHC) of the Regional Executive Secretary (RES) IV of Fortaleza, Ceará. The study subjects were a group of women who met the inclusion criteria: subjects were enrolled in one of the centers; were in the postpartum period; Had had at least years of age; had at least six prenatal visits, and; Had had a postpartum consultation. The exclusion criteria were: women who left the area covered by the FHC, or who had had a change of address during the period of data collection.
The women were chosen in the postpartum period so that they could report their experiences throughout the cycle. These women should have at least six prenatal consultations, as is recommended by the Ministry of Health(9), and one puerperal visit by the small number of women who undergo puerperal consultations(10). One hundred and fifteen mothers, divided into two groups, participated in this research: 54 primiparous women and 61 multiparous women.
The entry in the places to be investigated was carried out after obtaining the approval of the Ethics Committee in Research of the State University of Ceará, under number 26905 on May 14, 2012, and authorization from the Municipal System of School and Health and from the District of Primary Healthcare of RES IV, according to Resolution 196/96, which regulates research involving human beings(11). Upon release of the study, data collection occurred between the months of May to July, 2012.
There was an initial contact between researchers and the research patients in their homes and in the FHC by means of the community health agents. The goal of this contact was to supply the research subjects information about the study, which included the presentation by the researchers and the explanation of what was intended to happen and why, the need for ensuring anonymity of the participants’ responses, as well as highlighting the importance of their contributions, and, finally, offering participants the free choice whether to participate in the study or not. The acceptance resulted in signing the consent form. An instrument of data production was used to draw a socio-familial, demographic, and obstetric profile of the participants, and, subsequently, the Test of Free Association of Words (TALP).
TALP is characterized as a projective technique that encourages individuals to reveal the latent content of their memory in relation to a particular object, often implicit in their testimonies. The procedure for its application is rather simple: all you have to do is to announce one or more words to the subject. These words are called inducers. In response, the subject must verbalize the first words that come to mind as quickly as possible. One should be careful not to allow time for the preparation of statements; the words should be spoken as soon as possible(12).
There were four inductor words chosen for this study: educational actions; pregnancy; the post-natal recovery period, and; educational activities during the pregnancy and post-natal recovery period. The words were chosen with a view to getting closer to plain language and so they could be easily understood by users.
After the application of the test, for each inducing stimulus, a dictionary in which we inserted the entire repertoire of responses that were evoked throughout the sample, concerning their inducing stimulus, was created. Afterwards, the responses were organized in alphabetical order for verification of the most frequent answers and grouping of those with the highest frequency regarding the words that had the same semantic similarity, but which had appeared isolatedly or had statistically irrelevant frequency. Once the dictionaries were organized, the database was built(12-13).
Three fixed variables were chosen: parity, education, and age. Data processing was performed using the Trideux 5.1 software, which allows factorial correspondence analysis of the data. By means of use of this program, we observed correlations between groups, as well as visualizing the relations of attraction and spacing between the elements of the representational field concerning the object(12,14). The Trideux organizes the fixed variables in columns and the opinion modalities or variables in lines, which face each other and present themselves graphically in the representation of the factorial plan(13).
RESULTS
Demographic and obstetric socio-familial profile of the study participants
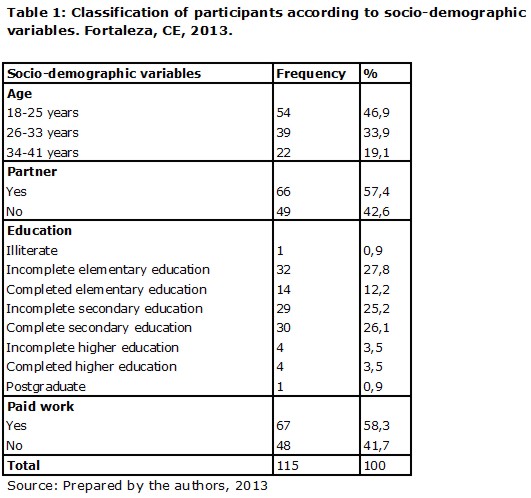
The data derived from the capture of the profile of 115 women who underwent TALP was submitted to statistical analysis by simple frequency and percentage, and was organized in tables that are capable of providing full viewing and understanding (Tables 1 and 2).
With regard to sociodemographic profile, Table 1 demonstrates that there was a variation of ages from 18 to 41 years, especially the age group between 18 and 25 years (46.9%), with a lower frequency of postpartum women aged above 33 years (19.1%). With respect to whether the participants lived with a partner or not, the majority lived with a partner (57.4%); 35 were married; 31 were in a stable union, and 42.6% had no partner.
With regard to education, 27.8% had an incomplete elementary education, 26.1% completed high school, and 25.2% had an incomplete high school education. Only one (0.9%) postpartum woman was a graduate. As for paid work, more than half (58.3%) had some paid work, while 41.7% of the women did not have any paid work.
Professions practiced in order of representation of the women were: household activities (42); maid (19); student (9); seamstress (5); sellers (4); housekeeper (3); babysitters (3); cook (2); manicurist (2); trader (2); sales promoter (2); artisan (2); waitress (2); public servant (2); production assistant (1); nutritionist (1); farmer (1); clerk (1); call center operator (1); receptionist (1); store manager (1); administrative assistant (1); street vendor (1); scullery maid (1); educator (1); cashier (1); general service provider (1); distributor (1); kitchen assistant (1); office assistant (1); embroiderer (1); janitor (1), and; sewing auxiliary (1).
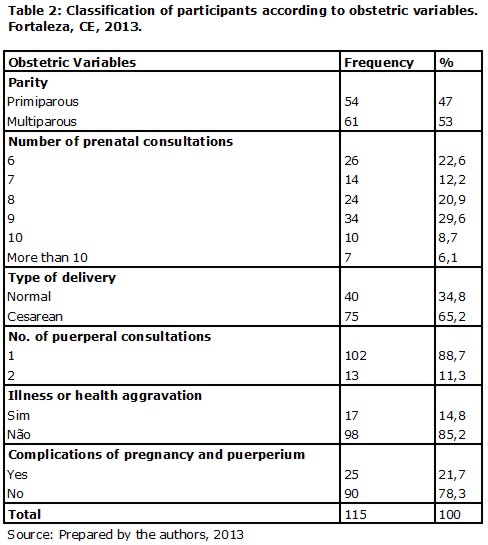
Table 2 shows the obstetric profile of the mothers in the study, and it demonstrates that the majority of the women were multiparous women (53.0%), that they had attended nine prenatal visits (29.6%), had had a cesarean delivery (65.2%), had attended a postpartum consultation (88.7%), did not have any illness or health problems (85.2%), and had had no complications during this pregnancy and childbirth (78.3%).
As for the 14.8% who reported any illness or health problems, six had some type of allergy (rhinitis, sinusitis, asthma), four were hypertensive, two had had cholecystectomy, two suffered from anemia, two had epilepsy/seizures, one suffered from celiac disease, one was diabetic, and one had depression.
In relation to complications in pregnancy and childbirth, which affected 21.7% of the mothers, we can mention: hypertension (9); threatened abortion (4); gestational diabetes (3); urinary tract infection (3); pre-eclampsia/eclampsia (3); seizures (1); case of abruption placentae (1); myoma (1); fetal distress (1); twin pregnancy (1); kidney infection (1), and; conjunctivitis (1).
It is worth mentioning the amount of cesarean deliveries (75), despite the small number of women who suffered complications during the last pregnancy, childbirth, and postpartum period (25).
Factorial correspondence analysis: evocations issued by the women
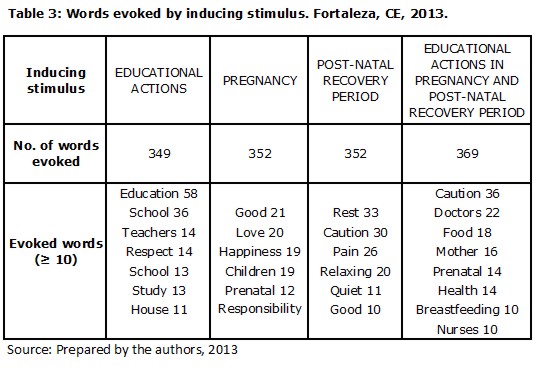
For this analysis, 1,422 words utilised in TALP aided the quest for understanding social representations of postpartum health education in pregnancy and childbirth. The stimulus or opinion variables used were: educational activities; pregnancy; post-natal recovery period, and; educational activities during pregnancy and the post-natal recovery period (Table 3).
Graph 1 represents two axes: Factor 1 (F1) on the horizontal axis and Factor 2 (F2) on the vertical axis. Factor 1 is represented prominently in bold, while Factor 2 is highlighted in italics. The fixed variables (parity, education, and age) are shown in uppercase.
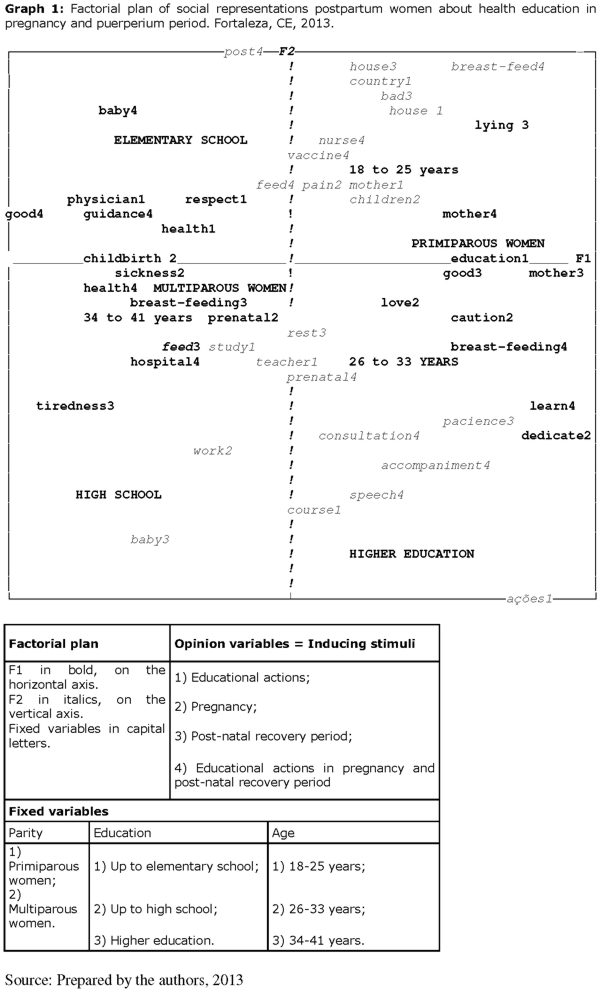
In F1, on the horizontal line, on the right side of the plane, it is possible to observe the most representative word and its correspondent factor (CF), constructed by the primiparous women (CF: 281) in relation to the educational activities stimulus, namely: education (CF: 41). In turn, on the left side, the multiparous group becomes evident (CF: 245) in the age group between 34 and 41 years (CF: 297), exhibiting the following evocations on the same stimulus: respect (CF: 33), medical (CF: 25), and health (CF: 12).
Still in F1, on the right side, lies the semantic field produced by the primiparous women in relation to pregnancy stimulus, represented as follows: dedication (CF: 38), care (CF: 28), and love (CF: 17). On the opposite side, the women in the age group between 34 and 41 years in the multiparous group evoke the words: sick (CF: 35), delivery (CF: 28), and prenatal (CF: 19).
As for the third stimulus, the post-natal recovery period in F1, on the right side, the words evoked by the group of primiparous women were: good (CF: 25), mother (CF: 22), and lying (CF: 18). On the left side, represented by the group of multiparous women, in the age group between 34 and 41 years, the following words stood out: fatigue (CF: 49), breastfeeding (CF: 16), and food (CF: 12).
Finally, in the fourth stimulus, educational activities during pregnancy and the post-natal recovery period, the primiparous women quoted the following words on the F1, right side: breastfeeding (CF: 49), learn (CF: 44), and mother (CF: 36). On the left side, the multiparous women, in the age group between 34 and 41 years, produced the words: health (CF: 55); good (CF: 46); orientation (CF: 39); baby (CF: 31), and; hospital (CF: 12).
In F2, the upper pole, regarding the educational actions stimulus, the words expressed by the group of primiparous women who had completed an elementary education (CF: 311) in the age group from 18 to 25 years (CF: 183) were: house (CF: 47), fathers (CF: 29), and mother (CF: 14). In the lower pole, represented by the group of multiparous women in the age group from 26 to 33 years (CF: 152), who had completed a high school education (CF: 97) or had advanced up to higher education (CF: 217) were: actions (CF: 68); courses (CF: 56); study (CF: 14), and; teacher (CF: 13).
Regarding the pregnancy stimulus in F2, we can observe the representative words in the upper pole: pain (CF: 12) and children (CF: 13), characterized by the group of primiparous women who had completed an elementary education, aged between 18 and 25 years. In the lower pole, the word ‘work’ (CF: 42) represents the group of multiparous women in the age group from between 26 and 33 years who had completed high school or had advanced to higher education.
Still in F2, the evocations issued for the stimulus post-natal recovery period in the upper pole were: home (CF: 26) and bad (CF: 25), representing the group of primiparous women who had completed an elementary education and were aged between 18 and 25 years. In the lower pole: baby (CF: 46), resting (CF: 26), and patience (CF: 15), representing the group of multiparous women in the age group from 26 to 33 years who had completed high school or had advanced up to higher education.
In the upper pole of F2, for the stimulus educational activities during pregnancy and the post-natal recovery period, the evoked words were: rank (CF: 35); breastfeeding (CF: 30); nurse (CF: 22); food (CF: 21), and; vaccine (CF: 15). In the lower pole: lecture (CF: 68); monitoring (CF: 39); consultation (CF: 31), and; prenatal (CF: 26), representing the group of multiparous women in the age group from 26 to 33 years who had completed high school or had advanced up to higher education.
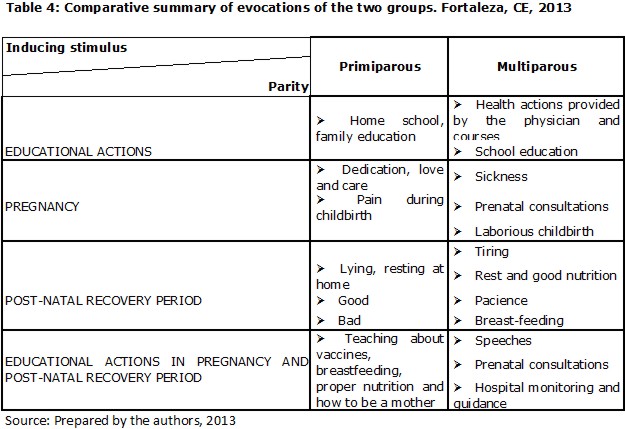
In Table 4, the evocations of the two groups were briefly introduced: primiparous and multiparous women.
DISCUSSION
Regarding the obstetric profile of the participants, it is worth mentioning the worrying number of cesarean deliveries in public health facilities (75), considering that most women did not suffer any complications during the pregnancy and childbirth cycle (25). This data confirms the growth and fast rise of cesarean sections in Brazil. In 2009, the proportion of caesarean deliveries in the public sector was 36.2%, well short of what is recommended by the World Health Organization (WHO)(15).
In the factorial analysis of correspondence we worked with different groups of postpartum women—primiparous and multiparous women—to verify the correlation between the groups. The words evoked by educational activities, pregnancy, the post-natal recovery period, and educational activities during pregnancy and the post-natal recovery period allowed the researchers to approach the multiple universes of meanings constructed in social relations and interaction among women, in response to the need to meet and recognize these women in order to understand and consequently intervene in reality(8,16).
Compared to the first stimulus—educational activities—the representative content for primiparous women is associated with home schooling, passed on from fathers/mothers to the child. The word ‘teaching’ expresses a vertical education and different word learning, in which women are inserted in the educational process. This evocation refers to the power of traditional pedagogy.
Furthermore, we can perceive family education in the evocations of the group. We observe the process of anchoring the object to the knowledge previously learned by women in known fields(6.8). There is nothing more natural than anchoring educational actions in one’s family experience, in one’s experiences with parents, children, in education, and formation in life.
As for the multiparous women, their evocations are marked by the institutionalization of knowledge; that is, the actions in health provided by the physician and courses, and also in school education, provided by the teacher.
The primiparous women perceive the family to be inserted in the educational process, but the consultations bly characterized by the biomedical referential induce in the multiparous women the replacement of the family by the physician as the main evocation in the educational process. The power of the biomedical discourse is capable of disqualifying the knowledge of users, to the point of pushing them not to value what they know and to go through a process of reframing the experience. After the consultations, they devalue the knowledge they have and value only scientific knowledge, even with the experience of a previous pregnancy.
In this sense, scientific knowledge is imposed by means of the authorized discourse of health professionals and popular knowledge is devalued. Thus, verticalized power relations are reproduced, with specific and generalized passages from the perspective of information and reference of health(17). However, subjects are not mere carriers of ideologies, but process information, form opinions, and build knowledge, and act according to the meanings they attach to the experiences of their daily lives(6,8).
The representations of pregnancy for the primiparous group are related to feelings and sensations: dedication, love, and care for the child, and the pain experienced during childbirth.
For these women, pregnancy is full of meanings; an experience beyond the organic and physical feelings. The experience of pregnancy brings bring more emotional aspects with the affective bond. On the other hand, the multiparous women refer to the frequent sickness during the period, as well as referring to the pre-natal consultations and characterizing childbirth as laborious. Their conception of pregnancy is more concrete and objective.
The primiparous women view the post-natal recovery period as a time when they need to spend more time lying down, resting at home, and that can be good or bad, similar to the conception of the multiparous women, who understand the post-natal recovery period as tiring, a period in which one needs to rest and emphasize good nutrition and patience regarding the care toward the baby, such as breastfeeding.
The conception of postpartum women regarding the educational actions during pregnancy and in the post-natal recovery period differs between the groups: the primiparous women understand these actions as the educational process at the health center with nurses, centering on vaccines, breastfeeding, proper nutrition, and how to be a mother. Multiparous women refer to lectures, prenatal consultations, monitoring, and hospital guidance on their health and their baby.
Such evocations reveal that health education is hegemonically mechanical since it has as a practical approach the lectures and individual guidance, both focusing on the baby and breastfeeding. The lecture represents a specific teaching activity, with a distant relationship between the action promoter and the other listeners, allowing for the expression of users in a limited way, since it does not deal with the various subjectifications addressed in the questioning method(5).
One may also realize, by means of the evoked words, that women fall behind, ceasing to be a woman or to be a mother. The focus of care is the baby and not the woman. What can also be seen in other studies is where women end up directing themselves to the attention and care of the children, husband, and home, showing that preoccupation with themselves is not a priority(18,19).
CONCLUSION
In the present study, the contents of the representations of women announce that education in health is the focus of lectures and activities aimed at the education of the child in social-familial spaces such as the home and school. The users did not restrict the meanings of education in health to the formal field of professional care because, in the production of meanings about the object, they have recognized the family as a legitimate area of educational action, conveyed from parents to children, with a discourse influenced by the family education.
Through the evocations verbalized by the women, it can be stated that the traditional model of information transmission predominates. The lessons are focused primarily on the care of the baby and breastfeeding. The woman is on the side of this care, this learning, as if, after the birth of her child, she ceases to exist and ceases to be a woman; to be only a mother.
The persistence of professionals is necessary in order to implement activities aimed at the improvement of educational activities in the area of women's health, through the sharing of knowledge and interaction among users, generating efforts for the realization of educational practices as a way to improve the impact of this action in the physical, mental, and emotional health of women during pregnancy and childbirth.
We need to reframe the educational actions to ensure they are understood as a vehicle for knowledge construction, not transmission. To provoke changes in these social representations of educational action, further studies involving the introduction of other elements that may reconfigure the field of representation are needed.
Health education as a right should dismantle the assistentialist, mechanistic vision of the body and point to a dialogue, knowledge socialization, and practices between professionals and users. The relationships that are established between professionals and users in these organizational and care conditions presented offer limited possibilities for establishing an effective communication that may contribute to the understanding of woman regarding their health condition, potentialities, and capabilities of personal and family changes.
As limitations of this study, we may highlight the quantity of participants and the restrictions to the CFs of a given RES (IV), from the capital of Ceará state, in which case the research should be expanded to other RES and other municipalities.
REFERENCES
1. Ministério da Saúde. Política Nacional de Atenção Integral à Saúde da Mulher: princípios e diretrizes. Brasília: MS; 2011.
2. Ministério da Saúde. Parto, aborto e puerpério: assistência humanizada à mulher. Brasília: MS; 2001.
3. Figueira TR, Ferreira EF, Schall VT, Modena CM. Percepções e ações de mulheres em relação à prevenção e promoção da saúde na atenção básica. Rev saúde pública. 2009; 43(6): 937-43.
4. Ministério da Saúde (Brasil). Portaria nº 1.459, de 24 de junho de 2011. Institui, no âmbito do Sistema Único de Saúde: a Rede Cegonha. Diário Oficial da União 27 jul 2011; Seção 1.
5. Bittencourt IS. Educação em saúde: conhecimento socialmente elaborado por enfermeiras e usuários. Jequié. Dissertação [ Mestrado em Enfermagem ]- Universidade Estadual do Sudoeste da Bahia; 2010.
6. Jodelet D. As representações sociais. Rio de Janeiro: EdUERJ; 2001. p.17-44.
7. Sá CP. A construção do objeto de pesquisa em representações sociais. Rio de Janeiro: EdUERJ; 1998. p.45-59.
8. Moscovici S. Representações sociais: investigações em psicologia social. Petrópolis: Vozes; 2009. p.29-109.
9. Ministério da Saúde. Pré-natal e puerpério: atenção qualificada e humanizada. Brasília: MS; 2006.
10. Martins SN, Rodrigues DP. Qualidade da consulta puerperal: percepção dos enfermeiros acerca da consulta puerperal em uma unidade básica de saúde de Fortaleza-CE. In: Anais do 61. Congresso Brasileiro de Enfermagem; 2009 dez 7-10; Fortaleza, Brasil. Fortaleza: Associação Brasileira de Enfermagem; 2009. p. 5409-11.
11. Conselho Nacional de Saúde (Brasil). Resolução nº 196/96, de 10 de outubro de 1996. Diretrizes e Normas Regulamentadoras de Pesquisas Envolvendo Seres Humanos. Diário Oficial da União 10 out 1996;Seção 1.
12. Nóbrega SM, Coutinho MPL. O teste de associação livre de palavras. In: Coutinho MPL, Saraiva ERA. Métodos de pesquisa em psicologia social: perspectivas qualitativas e quantitativas. João Pessoa: UFPB; 2011. p.95-106.
13. Coutinho MPL, Nóbrega SM, Araújo LS. O software Trideux: uma ferramenta metodológica aplicada ao campo de pesquisas em representações sociais. In: Coutinho MPL, Saraiva ERA. Métodos de pesquisa em psicologia social: perspectivas qualitativas e quantitativas. João Pessoa: UFPB ; 2011. p.107-47.
14. Cibois P. Les méthodes d’analyse d’enquêtes. Versailles: Université de Versailles; 2009. p.11-20.
15. Ministério da Saúde. Sistema Nacional de Vigilância em Saúde - Relatório de situação : Ceará. 5.ed. Brasília: MS; 2011.
16. Bittencourt IS, Vilela ABA. Representações sociais: uma abordagem teórica em saúde. RBPS. 2011; 24(1): 80-5.
17. Bonfim PF, Fortuna CM, Gabriel CS, Durante MC. Ações educativas em um Programa de Agentes Comunitários de Saúde. Rev bras enferm.2012; 65(3):420-7.
18. Monteiro LC. Representações sociais de puérperas sobre o cuidado de si e o cuidado de enfermagem no alojamento conjunto. Fortaleza.Dissertação [ Mestrado em Enfermagem ]- Universidade Estadual do Ceará; 2011.
19. Kalinowski LC, Favero L, Carraro TE, Wall ML, Lacerda MR. Postpartum primipara at home and associated nursing care: a data-based theory. Online braz j nurs [ Internet ]. 2012 Dec [ cited 2013 jan 30 ] 11(3). Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/3852. http://dx.doi.org/10.5935%2F1676-4285.20120046
Authors' Participation in the research:
Design: Dafne Paiva Rodrigues, Eryjosy Marculino Guerreiro;
Data collection: Eryjosy Marculino Guerreiro;
Analysis and interpretation: Dafne Paiva Rodrigues, Eryjosy Marculino Guerreiro, Márcia de Assunção Ferreira, Ana Beatriz Azevedo Queiroz;
Writing: Dafne Paiva Rodrigues, Eryjosy Marculino Guerreiro, Delano Franco da Costa Barbosa;
Critical review: Dafne Paiva Rodrigues, Márcia de Assunção Ferreira, Ana Beatriz Azevedo Queiroz, Ana Virginia de Melo Fialho;
Final approval of the article: Dafne Paiva Rodrigues.
Received: 28/02/2013
Revised: 14/11/2013
Approved: 17/11/2013