
ORIGINAL ARTICLES
Reproductive risks and comprehensive care of pregnant women with hypertensive syndromes: a transversal study
Rozânia Bicego Xavier1, Claudia Bonan1, Aline Carvalho Martins1, Kátia Silveira da Silva1
1Fundação Oswaldo Cruz
ABSTRACT
Aims: To analyze the socio-demographic and reproductive risk profiles of pregnant women with a history of hypertensive syndromes, as well as their clinical and obstetric conditions and the characteristics of the care given during prenatal, labor and post-labor care in maternity hospitals caring for women at high risk.
Method: transversal and quantitative study using the medical records of 164 pregnant women.
Results: The predominance of adult and black women, with low education levels, low income, multiple pregnancies and multiple reproductive risk factors. Insufficient prenatal clinical and nutritional care, the presence of hypertension at the moment of the labor and little attention given to reproductive planning during post-labor period have been were also observed.
Discussion: The care given at the maternity hospital is insufficient to meet the health needs of the women, which indicates fragmentation and discontinuity. Most of the women’s situations were characterized by a combination of individual, social and programmatic vulnerability factors.
Conclusion: Meeting the reproductive health needs of these women demands comprehensiveness, coordination and continuity of health care; professional capacity to handle the risks; transformation of vulnerability situations.
Descriptors: Comprehensive Health Care; Hypertension; Pregnancy, High-Risk.
During the last two decades, a number of transformations occurred in our country has given a favorable impact on the reproductive health indicators. However, the rates of maternal morbidity and maternal and child mortality are still high, reflecting not only the problems with access to and quality of care but also the persistence of social and regional inequalities, situations that generate vulnerability and compromise the exercise of reproductive rights(1). Maternal morbidity and maternal and child mortality are sentinel events; visible manifestations of a series of events and circumstances indicating risks to health determined not only by biological or environmental factors, but also by socio-cultural and institutional ones.
Many pregnant women come to the health service with problems that could be avoided, detected, treated or controlled before the pregnancy or during its early stages(2). The health care and reproductive planning of non-pregnant women with a history of morbidities such as hypertension, diabetes, AIDS, alloimmunization, or records of fetal or newborn death, are neglected. This lack of care exposes them to repeated pregnancies in unfavorable conditions, recurrent risks and negative results in many gestations(3). Many morbidities or risk conditions pre-existent to the pregnancy could be controlled, providing better maternal and neonatal results in future gestations(4). This is the case in pregnant women with chronic hypertension history and/or a history of hypertensive disorders in pregnancy (DHEG, in Portuguese). Hypertensive syndromes in pregnancy constitute one of the main causes of maternal mortality and morbidity in our country(5). They appear in different ways, such as part of a previous chronic hypertensive episode or as hypertension developed during pregnancy with or without pre-eclampsia or eclampsia. These two conditions can also arise without a history of previous hypertension, but indicate risks for the next gestation(6).
In our country, the prevalence of hypertension in women of reproductive age is significant. Official data show that 9.7% of women between 18-24; 15.4% between 25-34; and 21% between 35-44 have had a previous clinical diagnosis of hypertension(7). These data present the necessity of comprehensive attention and care of their reproductive health during or after the gestation in women with chronic hypertension and/or a history of hypertensive syndromes developed during previous gestations. The Ministry of Health has developed policies and programmatic actions regarding approaches to women with high-risk pregnancy diagnoses, and has also invested in the installation of a specific service network(6). The implementation of these actions is incomplete, however, lacking the development of lines of comprehensive care for women of reproductive age, specifically, for those with a history of hypertensive syndromes.
In this article, the results of a study are presented, based on the review of the clinical records of pregnant women with a history of hypertensive syndrome, attended at maternity hospitals caring for women at high risk. The aims of this study were to analyze the social-demographic and reproductive risk profiles; the characteristics of the care; and the clinical and obstetric conditions of pregnant women with a history of hypertensive syndrome in a maternity hospital caring for women at high risk during the prenatal, labor and post-labor periods. The results may be relevant for the discussion of lines of reproductive health care for women with a history of hypertensive syndromes in a comprehensive perspective.
METHOD
It is a transversal, quantitative study conducted at a maternity hospital which is a reference unit for gestational risk in Rio de Janeiro city. A data bank created for a previous study(8) was used, with socio-demographic, reproductive, clinical and obstetric information relating to 3,440 pregnant women, registered to this maternity hospital, between January 2006 and December 2008. In the present study, all the 164 pregnant women with records of hypertension during the present or previous pregnancy, and/or chronic hypertension, were included.
The women`s medical records were reviewed for the confirmation of hypertensive syndrome diagnosis, definition of the type of hypertensive disease (previous history of hypertensive disorders in pregnancy, pre-eclampsia and/or eclampsia; a present obstetric history of hypertensive disorders in pregnancy, pre-eclampsia and/or eclampsia; or chronic hypertension) and information on socio-demographic features, reproductive risk, clinical and obstetric conditions and characteristics of the care at the reference unity during prenatal, labor and post-labor periods.
For the systematization and treatment of this material, a data bank was created specifically with the EPI INFO program, version 3.5.3. The variants of the study were described by percentages. Regarding the description of the reproductive risk profile, the clinical and obstetric information gathered was regrouped according to the classification suggested by the Ministry of Health, as follows: a) individual characteristics and unfavorable socio-demographic conditions; b) previous reproductive history; c) previous clinical conditions and intercurrences; d) obstetric disease in the present pregnancy(6).
The study observed the ethical rules of Resolution 466/12 of Ethics in Research National Commission and was approved by the Ethics in Research Committee at the maternity hospital caring for women at high risk on 02/09/2009 (under nr 0066/09). Confidentiality was assured to conceal the identity of the women.
RESULTS
The age of the population studied varied from 15 to 46 years. Most women (61.0%), were aged between 20 and 35; followed by women of advanced maternal age (32.3%); and adolescents (6.7%). Black and mulatto women correspond to 62.8% of the population studied and 56.1% lived with husbands or partners. Most of the women lived in Rio de Janeiro city (59.1%) and the rest lived in other cities or states (Table 1).
Half the women presented with a low education level with at least the elementary school completed; 50.6% declared their family income to be less than or equal to 3 minimum salaries, including 8.5% whose families lived with less than one salary. On the whole, the women were housewives (39.6%) or had elementary occupations such as maids, nannies or general service assistants (25.6%) (Table 1).
A total of 84.8% women were multigestational (two or more pregnancies, including the present). Related to labor, 20.7% had never given birth, 58.5% had given birth one or more times and 20.7% had had at least three deliveries (data not presented on a table).
In relation to the reproductive risk profile, a history of miscarriage was relatively frequent among this population. About 31.7% reported one miscarriage; 3.7% had had this experience at least two or more times (habitual miscarriage); and miscarriages in hazardous situations were registered in 10.4% of the cases. Previous fetal and/or newborn death was verified in 23.2% of the cases. The presence of twins in the current pregnancy occurred in 3.0 % of the cases and 3.7% in previous pregnancies.
Among the clinical and obstetric conditions in the present pregnancy, gynecopathies existed in 5.5%, rhesus isoimmunization in 6.1% and nuchal translucency altered in 3.0% of the pregnant women. Other pathologies were registered in less than 2.0%. Fetal malformation in the present or previous pregnancy was registered in 20% of the cases (Table 2).

Besides the reproductive risks described above, a history of hypertensive syndromes was present in all the population studied. Previous hypertensive disorders in pregnancy, pre-eclampsia or eclampsia were observed in 37.2% of the pregnant women; in the present pregnancy, the same pathologies were found in 10.4% and chronic hypertension in 61.0% (Table 2).
A total number of 31.3% of women with previous history of hypertensive disorders in pregnancy, pre-eclampsia and eclampsia was registered at the reference unity at less than 14 weeks gestation; 27.9% between 14 and 19 weeks; 37.7% between 20 and 30 weeks; and 3.3% initiating prenatal care at more than 30 weeks. Among the pregnant women with a history of chronic hypertension (61% of the population), 39% were registered at less than 14 weeks gestation; 23% between 14 and 19 weeks; 25% between 20 and 30 weeks; and 13% initiating their prenatal care at the maternity hospitals caring for women at high risk after 30 weeks. These results show that the most of the women with reproductive risks which could be identified in the first three months came to the specialized service in the second or third trimester.
At the moment of their admission to prenatal care, almost 30% of the pregnant women presented with high blood-pressure levels, and considering the total of the population studied, 6.1% presented accentuated forms of hypertension, with levels higher or equal to 160x110 mmHg. The use of anti-hypertension medication at the moment of the admission was informed by 37.2%, a percentage quite inferior to the percentage of women who declared themselves to be chronically hypertensive (61%). Many women (87.8%) referred to familiar antecedents of hypertension syndromes (Table 3).
The use of alcohol during pregnancy was informed by 10.4% of the women and smoking by 11.6%. In relation to the nutritional situation, 58.5% of the women were overweight or obese. Two thirds of the women declared the pregnancy was not planned (Table 3).

During the prenatal care at the maternity hospital caring for women at high risk, more than two thirds of the women had had six or more obstetric appointments and had gone through educational activities; in only 40.9% of the medical records there was notation of physician appointment and 14% with a nutritionist. During the present pregnancy, 25.6% needed admission because of hypertensive episodes.
It could be observed that 14% of the women did not continue the prenatal care at the reference unit, and it is not known if they were sent to or opted for prenatal care or labor in another institution (Table 3). Among the population studied, 123 pregnant women (75%) delivered their babies at the unit. At the moment of admission for the delivery, 52% of those women were hypertensive and 13.8% presented with accentuated hypertension, their blood pressure being equal to or higher than 160 x 110 mmHg (Table 4). Most deliveries (58.5%) were conducted without occurrences; and 35.8% of occurrences were related to hypertension. C-sections were performed for 71.5% of the women. The puerperium occurred without problems in 75.6% of the cases and the occurrences registered were related, mainly, to hypertension (Table 4).
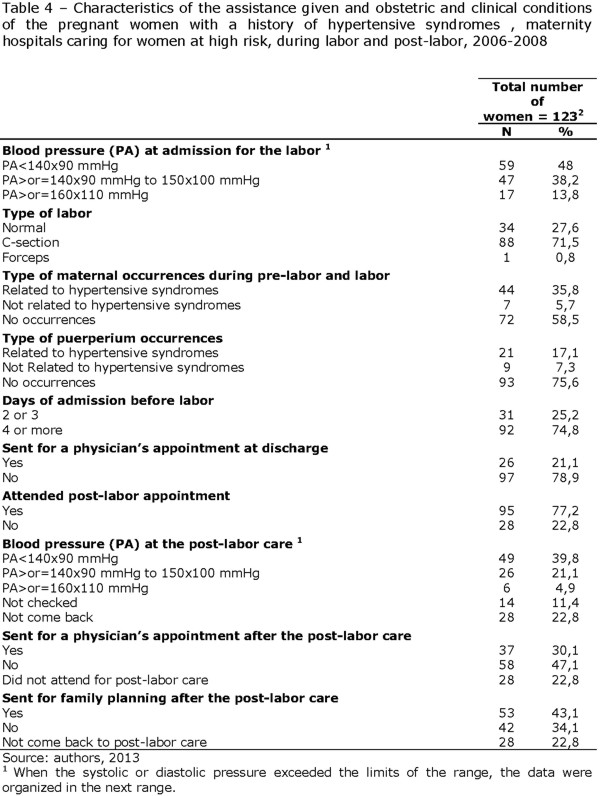
More than half the newborns (51.2%) presented good general state; 13.8% were premature, associated or not with low birth weight; 6.5% were malformed; 4.9% presented with low birth weight; and 4.1% fetal suffering. After at least a four-day stay (underwent by 74.8% of the cases), 60.2% of the women were discharged with their babies. The hospital discharge records indicate that the patient was not sent to a physician in 78.9% of the cases (Table 4).
Among the 123 pregnant women who had the baby at the unit, 28 (22.8%) did not return after the labor (Table 4). Among the 95 who came back for the post-labor care, 33.7% were hypertensive, with blood pressure levels equal or higher than 140x90 mmHg to 150x110 mmHg’ 6.3% presented with blood pressures equal or higher than 160x110 mmHg. Two situations have drawn the attention: 14.7% of the women who came back for the post-labor care did not have their blood pressure checked; and in 61% of the cases there was no record of the patient being sent to the physician (data not presented on the table). In the post-labor period, only 55.8% of the women who attended their appointment were sent to the family planning clinic (data not presented on the table).
DISCUSSION
The results present a concerning reality in which multiple situations of health vulnerability(7) overlap and potentiate each other, in a general way. Considering individual situations, besides a history of previous hypertension in a previous or present pregnancy, most women presented with other morbidities (overweight, obesity, smoking, alcohol, gynecopathies and/or other chronic diseases), and with other conditions also considered as gestational risk factors (history of miscarriage, fetal or newborn death and/or malformation). Other studies demonstrated the association of these risk factors with hypertensive disease in pregnancy(10).
Hypertensive syndromes are considered one of the main primary determinants for serious maternal morbidity and mortality and, besides that, the conjunction of hypertension with other morbidities and risk conditions increases the chances of misfortune for the women and/or their babies(11, 5). The multiple risk factors accumulated by the women in this study compose a scenario of moderate maternal morbidity, a kind of “vestibule” leading towards serious maternal morbidities and many times fatal. Considering the health care policies, it is necessary a specific approach to this population regarding the specialized, comprehensive and qualified care needed, during, before and after the pregnancy, in order to reduce these avoidable events, in their major part.
Situations of social vulnerability, indicated by low income and low education levels, are associated with individual health conditions, potentiating the women’s reproductive risks. Studies show the association between precarious social-economic conditions and bad reproductive health indicators(12, 13); some have specifically concluded that lower levels of maternal education are associated with serious maternal morbidity and maternal mortality(13,14,15). Situations of health vulnerability – individual, social and programmatic – caused by ethnic-racial inequalities have already been clearly demonstrated in the literature (16); what helps to understand the overrepresentation of black women in the studied population.
Despite the limitations of the study, these results indicate the need to consider another dimension in the context of vulnerabilities experienced by the women, and that come partially over the social and individual conditions: the questions that are related to the access and quality of health care – what has been called programmatic vulnerability(9). Many women admitted to the reference unit were from other cities or states; what leads to questions about the difficulties they found in being admitted to the health care services nearest to their homes. Amaral et al.,(11) in their study of serious maternal morbidity in Campinas, verified that 48% of the patients were sent to other cities, revealing the fragile organization of the regional perinatal care.
According to the Ministry of Health’s criteria(6), the identification of any reproductive risk factor during prenatal care at the basic health care service should result in sending the patient immediately to the reference unity. However, problems with the health care network with the reference and contra-reference systems and with the professionals handling the risk conditions are obstacles to adequate attention being paid to the high-risk pregnancy. More than one third of the women studied started prenatal care in the second or third trimester. Considering the prevalence of chronic hypertension, other diseases and previous reproductive risks in the group of pregnant women studied, questions arise about the reasons they did not come earlier to the maternity hospitals caring for women at high risk: Did they delay their prenatal care? Did the basic health care unit identify the risks? What problems could have arisen between the visit to the basic health care unit and the prenatal care appointment? In Rio de Janeiro city, despite the increase of prenatal care network, there are problems in relation to the quality of the care given(17).
Comprehensive and qualified prenatal care, in all levels of complexity, is fundamental to minimize the occurrences caused by hypertension to the mother and/or the fetus(18). In the reference unity studied, care given to the pregnant women with hypertensive syndromes histories were centered in the obstetric appointment, and was fragmented and discontinuous. Many records showed there was no registration of a physician appointment during prenatal care, or even being sent for physician assistance at admission. During post-labor care, an impressive number of women were hypertensive and even so they were not sent for a physician appointment. Besides that, almost 15% of the women did not have their blood pressure checked at the moment of the research. The importance of the quality of clinical care, with adhesion to protocols, was emphasized in a study of serious maternal morbidity, especially when there are hypertensive occurrences (11).
Other findings of the research show the deficiencies in the care provided to the women. Despite the high prevalence of overweight and obesity – conditions that predispose and aggravate hypertension during pregnancy(10) - there was no indication in the women’s records they were sent for a nutritionist appointment. One third did not participate in educational activities during the prenatal period and there is no mention of the approach taken in cases of smoking and alcohol use, which are notoriously harmful to the fetus and mother’s health(19). Educational actions and multiprofessional assistance are important aspects of comprehensive care, as they favor the consideration of health and sickness, comprehension of risks and discussion about life and nutritional habits, physical activities and other factors.
Comprehensive care involves professionals and health care institutions taking responsibility for the patient. About 15% of the pregnant women with hypertensive syndromes discontinued their treatment at the reference maternity hospital without being sent to, or opting for, another service unit. Nevertheless, in the medical records, there is no registration of contact with the absent women.
The material studied does not permit a better evaluation of the access conditions and quality of care regarding the reproductive health of the women before the present pregnancy. Nonetheless, it calls attention to the fact that two thirds of the women said they had not planned the pregnancy, which indicates contraception needs not met. More than a decade after the regulation, the difficulty has been documented of implementing reproductive planning assistance policies(20). At the reference unity, the approach to reproductive planning has been deficient. Even though family planning service is part of the care given to women after labor and an important component of women’s social rights that has already been won(6), almost half of the women who came back to the post-labor care were not sent for family planning advice.
The present study has limitations due to the fact that the medical records – the main document about the patient’s health conditions and the care given - were the only source of information and contained many mistakes. We believe, however, that the results contribute to a better knowledge of the reproductive health needs of women with a history of hypertensive syndromes offering information that may lead to better care given to this population.
CONCLUSION
The results of this study show that the health care given to pregnant women with a history of hypertensive syndromes at the reference unity was insufficient to contemplate in a comprehensive way their health needs. However, they also suggest that their unmet health needs are previous to the admission to the high-complexity service (and may contribute to this result) and, furthermore, the fragmentation and discontinuity of health care can be perpetuated after their discharge from the reference service.
The issue that puts together “reproduction” and “hypertension” – because of the frequency of hypertension in women of reproductive age or because of its role in the maternal morbidity/mortality scenario – offers us clues to think about the construction of lines of comprehensive care in reproductive health. It puts in evidence the need for programmatic actions of health promotion, risk prevention and care for women throughout their reproductive life (before, during and after pregnancy). This leads to the question of continuity of care in a longitudinal sense and the coordination of health care workers (professionals, programs, services) in a transversal sense.
It points out the necessity of a greater integration among the several levels of a complex health care system, in a way to precociously receive the pregnant women, promptly identify the reproductive risks, and guide and facilitate their access to reference services. In an opposite way, these services must be responsible for the contra-reference and follow the return process of these women to lower levels of complexity, to the continuity of health care.
The questions raised by the results of this research call the attention to the fact that, even in highly specialized environments and with advanced technological resources available – such as the maternity hospital caring for women at high risk – the perspective of comprehensiveness cannot be in a secondary place. There must be attributes of the high-complexity assistance such as: to develop a comprehensive assessment of the individual’s health needs; the offering of education activities; and the promotion of multiprofessional work and an interdisciplinary approach in which the processes of reproductive health or sickness can be understood, not only in biological terms, but also in their social, economic and cultural determinants.
At last, developing and implementing lines of comprehensive care for women of reproductive age with a history of hypertensive syndromes can have an important impact upon maternal and neonatal health indicators. The organization of work processes between professionals and services in a way to guarantee the comprehensiveness, coordination and continuity of care; a higher technical capacity of professionals to enhance their ability to recognize risks and appropriate handling of prenatal care and the development of the abilities of professionals and institutions to provide comprehensive approach to the health necessities are vital tasks, but still challenging, for the construction of what can be called comprehensive care.
REFERENCES
1. Victora CG, Aquino EML, Leal MC, Monteiro CA, Barros FC, Szwarcwald CL. Maternal and child health in Brazil: progress and challenges. Lancet. 2011; 377(9780): 1863-76.
2. Gondim ANC, Oliveira AS, Chagas ACMA, Lessa PRAL, Barbosa BN, Damasceno AKC. Fast HIV screening test for parturients: a quantitative study. Online braz j nurs [ Internet ]. 2010 [ cited 2011 sep 11 ] 9(2). Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/2997. doi: http://dx.doi.org/10.5935/1676-4285.20102997
3. Vettore MV, Dias M, Domingues RMSM, Vettore MV, Leal MC. Cuidados pré-natais e avaliação do manejo da hipertensão arterial em gestantes do SUS no Município do Rio de Janeiro, Brasil. Cad saúde pública. 2011; 27(5): 1021-34.
4. Fonseca SC, Coutinho ESF. Fatores de risco para mortalidade fetal em uma maternidade do Sistema Único de Saúde, Rio de Janeiro, Brasil: estudo caso-controle.Cad saúde pública. 2010; 26(2): 240-52.
5. Lotufo FA, Parpinelli MA, Haddad SM, Surita FG, Cecatti JG. Applying the new concept of maternal near-miss in an intensive care unit. Clinics. 2012; 67(3): 225-30.
6. Ministério da Saúde. Gestação de alto risco. 5. ed. Brasília: MS; 2012.
7. Rede Interagencial de Informações para a saúde [ homepage in the internet ]. Informações de saúde, demográficas e socioeconômicas [ cited 2013 feb 13 ]. Available from: http://tabnet.datasus.gov.br/cgi/idb2011/matriz.htm.
8. Xavier RB, Jannotti CB, Silva KS, Martins AC. Risco reprodutivo e renda familiar: análise do perfil de gestantes. Ciênc saúde coletiva. 2013; 18(4): 1161-71.
9. Ayres JRCM. Organização das ações de atenção à saúde: modelos e práticas.Saúde soc. 2009; 18 Suppl 2: 11-23.
10. Dálmaz CA, Santos KG, Botton MR, Roisenberg I. Risk factors for hypertensive disorders of pregnancy in southern Brazil. Rev Assoc Med Bras. 2011; 57(6): 692-6.
11. Amaral E, Souza JP, Surita F, Luz AG, Sousa MH, Cecatti JG, Campbell O. A population-based surveillance study on severe acute maternal morbidity (near-miss) and adverse perinatal outcomes in Campinas, Brazil: the Vigimoma project. BMC pregnancy childbirth. 2011; 11(9):1-8.
12. Leal MC, Pereira APE, Lamarca GA, Vettore MV. The relationship between social capital, social support and the adequate use of prenatal care. Cad saúde pública [ Internet ]. 2011[ cited 2013 Dec 04 ] 27 Suppl 2: 237-53.Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2011001400011&lng=en. http://dx.doi.org/10.1590/S0102-311X2011001400011
13. Villamizar LAR, Ruiz-Rodríguez M, García MLJ. Beneficios de combinar métodos para analizar causas de muertes maternas, Bucaramanga, Colombia. Rev panam salud pública. 2011; 29(4): 213–9.
14. Karlsen S, Say L, Souza JP, Hogue CJ, Calles DL, Gülmezoglu AM, et al . The relationship between maternal education and mortality among women giving birth in health care institutions: analysis of the cross sectional WHO Global Survey on Maternal and Perinatal Health. BMC Public Health. 2011 [ cited 2013 Dec 04 ] 11(606). Available from: https://open.library.emory.edu/publications/emory:f78dd/
15. Souza JP, Cecatti JG, Parpinelli MH, Sousa MH, Lago TG, Pacagnella, Camargo RS. Maternal morbidity and near miss in the community: findings from the 2006 Brazilian demographic health survey. BJOG. 2010; 117(13): 1586-92.
16. Bastos JL, Peres MA, Peres KG, Dumith SC, Gigante DP. Diferenças socioeconômicas entre autoclassificação e heteroclassificação de cor/raça. Rev saúde pública. 2008; 42(2): 324-34.
17. Domingues RMSM, Hartz ZMA, Dias MAB, Leal MC. Avaliação da adequação da assistência pré-natal na rede SUS do Município do Rio de Janeiro, Brasil. Cad saúde pública. 2012; 28(3): 425-37.
18. Assis TR, Viana FP, Rassi S. Estudo dos principais fatores de risco maternos nas síndromes hipertensivas da gestação. Arq bras cardiol. 2008; 91(1): 11-7.
19. Freire K, Padilha PC, Saunders C. Fatores associados ao uso de álcool e cigarro na gestação. Rev bras ginecol obstet. 2009; 31(7): 335-41.
20. Bonan C, Silva KS, Sequeira ALT, Fausto MCR. Avaliação da implementação da assistência ao planejamento reprodutivo em três municípios do Estado do Rio de Janeiro entre 2005 e 2007. Rev bras saúde mater infant. 2010; 10 Suppl1: 107-18.
Received: 27/02/2013