ORIGINAL ARTICLES
Sexual health of pregnant women in a basic healthcare unit: a descriptive study
Ana Clara Patriota Chaves1, Maria Albertina Rocha Diógenes2
1State University of Ceará
2University of Fortaleza
ABSTRACT
Aim: To assess the sexual health of pregnant women, and identify possible risk factors.
Method: Exploratory and descriptive study with 40 pregnant women at a Health Center in Quixadá – CE, from December, 2011 to February, 2012.
Results: Findings show an average sexual initiation age of 16; 55% had sexual relations with more than one partner. Contraceptive methods used prior to pregnancy were condoms (60%) and oral contraceptives (57.5%). During pregnancy, 75% did not use condoms during sexual relations. Main gynecological complaints were pelvic pain (77.5%), dysuria (70%) and vaginal discharge (65%); 70% had not done a cytopathological test during the pregnancy.
Discussion: Women are initiating their sex lives and becoming pregnant prematurely without proper information and awareness of STD prevention and the importance of the cytopathological testing.
Conclusion: The study showed that pregnant women were significantly vulnerable to STDs, and discussed how this issue must be addressed and treated during prenatal care.
Descriptors: Women’s Health; Pregnant Women; Sexually Transmitted Diseases; Prenatal Care; Primary Health Care.
INTRODUCTION
The gestational period is a phase marked by physiological and psychological changes in a woman’s life. There are feelings of joy and satisfaction, but also of fear, insecurity and despair, which all affect the sexuality and sexual behavior of women, making them vulnerable to certain risks. Other gestational changes, such as low immunity and anatomic and hormonal changes, may lead to sexually transmitted diseases (STDs).
In turn, such diseases impact on maternal and fetal health, and transmission may take place during pregnancy, or during and after childbirth(1).
For both sexes, STDs increase an individual’s vulnerability to HIV and Aids, and may lead to higher maternal and infant mortality. STDs may result in cervical pain, inflammatory pelvic disease, infertility, cervical cancer, miscarriage, premature birth, congenital and prenatal infections, puerperal infection, all of which are risks that emerge during pregnancy and puerperium. Additionally, they may seriously affect the fetus, or even result in fetal or neonatal death, and childbirth sequelae. Nevertheless, if these diseases are treated at an early stage, the consequences can be minimized(2).
Furthermore, the number of women infected by HIV has risen in the last few years, confirmed by the ratio between the number of men with HIV for every woman with HIV, which has decreased. In 1989, the ratio was 6 to 1. Alarmingly, in 2009, that ratio dropped to 1.6 men for every woman infected(3).
However, what frequently happens during the prenatal period is that more attention is paid to the more common gestational period diseases, at the expense of STD treatment. Healthcare services rarely provide gynecological testing during the prenatal period, and usually a gynecological test is only done after a patient complains of vaginal disturbances(4).
It is also important to bear in mind that integral assistance must be provided to pregnant women, which means addressing their sexual health during the prenatal period by sharing ideas and information on how they can experience their sexuality in a healthy way.
Therefore, it is important for healthcare staff to understand the sexual behavior of these women by continual monitoring in monthly prenatal consults, in order to prevent STDs and resulting complications during pregnancy, as well as encouraging healthy habits in their sex lives.
In this context, there is a need for specific research to assess the sexual health of pregnant women and to identify risky behavior or vulnerability that may negatively affect the health of pregnant women and their children. Thus, a key question of this study arises: What are the risk aspects related to the sexual health of pregnant women?
With this in mind, the research aims to identify risky sexual behavior among pregnant women, identify the main gynecological complaints, and verify the achievement prenatal cytopathological testing.
These characteristics will provide the basis for new approaches regarding this issue, and propose intervention by means of a multidisciplinary team that can effectively promote healthiness, prevent disease, and offer the means by which each woman can care for her own health.
METHOD
This is a descriptive and exploratory study in a Basic Health Unit (UBS) in the rural area of the Quixadá-CE municipality, Brazil, between December, 2011 and February, 2012.
In this unit, the Programa de Saúde da Família (Family Health Program) offers health services with a team that includes a doctor, a nurse, a nursing technician, 3 general services staff, and 9 community health agents. Both doctor and nurse give prenatal consults.
The eligible population included 50 registered pregnant women who were monitored at the Basic Unit for Family Health in Várzea da Onça, a rural area in the Quixadá Municipality. The participants were selected by means of random sampling based on convenience, which takes samples based on the accessibility of the participants.
All the women in the sample were pregnant, registered and monitored at the unit, agreed to participate in the study, and had received at least one prenatal consult. The study excluded any pregnant women who had changed residency, even if they were registered and were already receiving prenatal consults. After all the inclusion and exclusion criteria were applied, the accessible population was 40 pregnant women.
For data gathering, the study used a form containing questions regarding social-demographic variables, sexual behavior variables and any gynecological complaints. This form was handed out to participants during prenatal consults, and a cytopathological test was also used to gather data.
The data analysis involved the use of the statistics software program Statistical Package for Social Sciences (SPSS), version 19.0. The analysis used descriptive statistics (simple, average, median frequency and pattern deviation), variable intersection, and the Odds Ratio calculation. The data was put on charts to facilitate visualization and comprehension, and later analyzed using the relevant literature.
The research was compliant with all ethical and legal principles of Resolution 196/96(5), and was approved by the Committee for Ethics in Research at the State University of Ceará, under the protocol number 11582654-8. Before signing up for the study, all the women were briefed on the research project, and then signed an Informed Consent Form.
RESULTS
Socio-demographic data
The average age of the women was 25.8 years (DP =6.4) and the average level of education was only 7.7 years (DP=3.1). For family data, there was an average of 4 persons per family and an average of 5 rooms per home. 31 of the families (77.5%) had a single breadwinner, and most of these individuals (n=35; 87.5%) received less than the minimum salary (R$545) and 25 (62.5%) received benefits from government programs.
Sexual health aspects
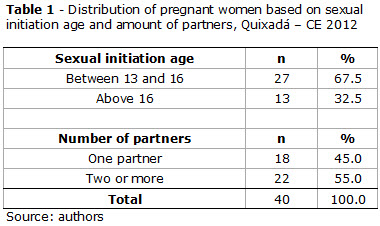
Table 1 shows the sexual initiation age and number of sexual partners of the research participants.
As for the sexual activity of these women, one notices that most initiated their sexual life between the ages of 13 and 16, with an average age of 16 in terms of their first sexual experience, and a median age of 15. One can also notice that 22 (55%) had two or more sexual partners.
Table 2 shows the intersection of data on schooling and the sexual initiation age.
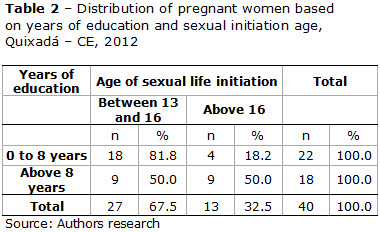
It can seen that the majority (n=18; 81.8%) of those with up to 8 years of education, which corresponds to elementary schooling, had a more premature sexual initiation when compared to the others. Upon calculating the Odds Ratio (OR=18*9/9*4; OR=4.5), the participants with a lower level of education had a 4 times greater chance of beginning their sexual life prematurely than did the participants with more than 8 years of education.
As for contraceptive methods, Table 3 shows the participants’ data regarding the use of condoms and oral contraceptives.
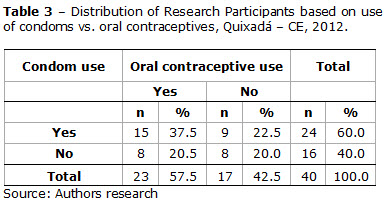
The survey found that 24 (60%) and 23 (57.5%) of the participants, had previously used condoms or oral contraceptives at some point during sexual relationships. 15 (37.5%) reported using double protection before becoming pregnant. Nevertheless, the survey shows that a significant percentage of participants did not use condoms.
As for intercourse during pregnancy, the majority (n=32; 80%) maintained sexual relations, but 30 (75%) did not use condoms.
Table 4 shows the main gynecological complaints of the participants.
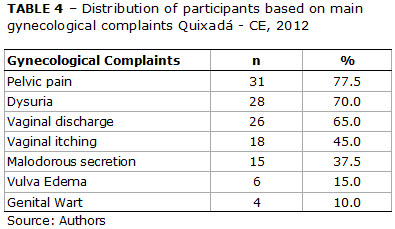
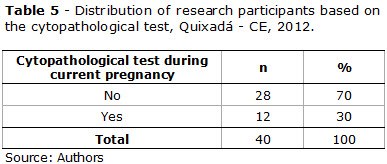
The most frequent gynecological complaints the participants mentioned were pelvic pain (n=31; 77.5%), dysuria (n=28; 70%) and vaginal discharge (n=26; 65%). In addition, four women (10%) had genital warts. In addition, most of the women (n=28; 70%) did not undergo a cyptopathological test during the prenatal exam, as shown in Table 5.
DISCUSSION
Some of the aspects related to the sexual health of the pregnant women may point to a greater risk or vulnerability of this group to STDs/AIDS.
The women had a low educational level, averaging 7.7 years of study, and low family income, since most of them (87.5%) received less than the minimum monthly salary (R$545). These factors are linked to the number of pregnancies, which frequently cause school absenteeism, and consequently, lower educational levels and income, as another piece of research has shown(6).
The research findings show that the average sexual initiation age was 16, as confirmed by the research of Custódio et al(7). Other studies (8-9) show an even lower age of 15 for sexual initiation, which is close to the age reported in the current study. It is clear that many teenagers begin their sexual lives at a premature age, without having enough knowledge of STDs, unplanned pregnancy and prevention methods.
Premature sexual initiation combined with a multiplicity of sexual partners as shown in the study, are both risk factors for women, and leave them exposed to STDs and AIDS. These findings corroborate the results of another piece of research(10) that included 1,543 women aged 15-49, whose main risky behaviors were unprotected sex (72%), sexual initiation at ages younger than 18 (47%), their sexual partner´s use of alcohol and drugs (14%), and finally, having two or more sexual partners (7%).
Much like this research, which shows how women with a relatively low level of education have a higher chance of beginning their sex lives prematurely, other studies(11-12)show the significant connection between low educational levels and family income, and the early onset of sexual life. Furthermore, in another piece of research(13) with 73 pregnant women in the municipality of Quixadá, 82.2% of the women had never participated in educational activities, which made sexual counseling and education difficult. This is unfortunate, considering how important knowledge and information about sexuality is to ensure safe sex practices during this period in a woman’s life.
As for condom use, this research found that most of the pregnant women had previously used condoms or oral contraceptives. Research by Duarte et al(8) involving 487 women, found that the most frequently used contraceptive methods prior to pregnancy were oral contraceptives (61.8%) and condoms (38.2%). In another piece of research(14), this time with 339 women, oral contraceptives were found to be the most frequently used method (59%), followed by condoms (57%) prior to pregnancy. Even though the use of contraceptive methods has risen among couples, the percentage that uses double protection is still low when compared to the percentage that uses a single contraceptive method, whether condoms or oral contraceptives.
The research also found most of the women who maintained sexual relations during pregnancy did not use condoms. These findings corroborate those of another study done with 11 pregnant women, in which none of the women admitted to using condoms during their pregnancy. Many pregnant women feel a condom is unnecessary during intercourse since there is obviously no possibility of becoming pregnant. In other cases, condoms are not used because husbands reject the idea altogether, and this attitude may be related to STDs/AIDS(15) exposure.
The most frequent gynecological complaints made by the research participants were pelvic pain, dysuria and vaginal discharge. A similar study with 339 pregnant women pointed to a 51.6% occurrence rate of vaginal discharge, confirming it as one of the most common gynecological complaints(14).
The main factors associated with pathological vaginal discharge during pregancy are STDs, being aged below 20, unstable conjugal unions, multiple sex partners, and habitual sexual relations without condoms(14).
One the most frequent causes of vaginal discharge is a chlamydia infection. Multicentric research(4) with 3,303 pregnant women found that chlamydia infections and gonorrhea and chlamydia co-infections in this group had a prevalence rate of 10% and 9.4% respectively. Likewise, research done by Brandão, Lacerda and Ximenes(16) found a prevalence rate of Chlamydia at 4.4% among 96 pregnant women, and this infection was associated with premature sexual initiation.
The frequency of STD signs and symptoms has risen considerably among pregnant women, from 3.5% in 2006, to 10.1% in 2011(17). Research done(18) with 120 women found that 77.5% had some kind of gynecological infirmity, including candidiasis (40%), bacterial vaginosis (25%), and trichomaniasis (13%). Such symptoms may be associated with pelvic pain, dysuria, and intense vaginal discharge and, if not properly treated, may evolve to serious conditions during puerperium.
Another important issue related to sexual health is the cytopathological test. A large number of pregnant women begin prenatal care with an outdated cytopathological test. Apparently, this test is not common among pregnant women as there are still prejudices, taboos and fear surrounding the issue, especially during pregnancy, which hinders timely STD detection(19).
In a study(20) done with 230 women who had recently given birth, 155 of them were advised to do a cytopathological test during prenatal care, but only 33.6% did so. This data is similar to that of this research, which found that only 30% did this test. Another study(19) done with 445 women who had recently given birth, identified the need for cytopathological testing during prenatal care, as 272 of the women (61.8%) had outdated cytopathological tests.
Some of the factors that interfered with testing were: fear of having samples taken due to being pregnant, fear of pain, difficulty making an appointment and returning to the hospital to take the test. This overview shows that during prenatal consults, health professionals must pay closer attention to the patients’ sexual health, stress the need for gynecological exams and focus on the prevention of STDs and AIDS.
CONCLUSION
Despite the limitations this study faced, especially regarding the sample since the study was done in a rural area, one can conclude that when assessing the sexual health of a group of pregnant women, there are high prevalence factors that imply a higher risk and vulnerability to STDs/AIDS. These factors are mainly a low level of education, low family income, premature sexual initiation, multiplicity of partners, and unprotected sex during pregnancy.
Additionally, this group of women presented exposure behavior and gynecological complaints such as pelvic pain, dysuria, vaginal discharge and warts, all of which can possibly indicate STDs. Thus, all of the above should be investigated during prenatal care, and a cytopathological test should be done if necessary.
This test, which should have been a tool for early diagnosis, was inefficient, most likely because there is still a lack of knowledge on the part of pregnant women, as well as insufficient investigation and awareness on the part of health professionals.
Thus, it is the responsibility of the health professionals, especially nurses, to provide appropriate nursing care to women in every stage of their lives, and to encourage the womens’ participation in activities that promote family planning, proper condom use, STDs/AIDS prevention and healthy sexual habits.
Furthermore, it is important to gauge nursing assistance deficiencies during prenatal care so that these can be corrected, to reinforce health education by building new concepts with these women, and to encourage behavioral changes to protect them from exposure to STDs.
REFERENCES
1. Guarnizo TM, Pardo TMP. El significado de la sexualidad durante la gestación. Av enferm [ Internet ]. 2011[ Cited 2013 Jan 10 ] 29(2):294-306. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0121-45002011000200009&lng=en.
2. Barcelos MRB, Vargas PRM, Baroni C, Miranda AE. Infecções genitais em mulheres atendidas em Unidade Básica de Saúde: prevalência e fatores de risco. Rev bras ginecol obstet. 2008;30(7):349-54.
3. Ministério da Saúde (Brasil) [ homepage on Internet ]. Departamento de DST, Aids e Hepatites virais. Aids no Brasil [ cited 2010 dec 2010 ]. Available from: http://www.aids.gov.br/pagina/aids-no-brasil
4. Jalil EM, Pinto VM, Benzaken AS, Ribeiro D, Oliveira EC, Garcia EG, et al. Prevalência da infecção por clamídia e gonococo em gestantes de seis cidades brasileiras. Rev bras ginecol obstet. 2008;30(12):614-9.
5. Ministério da Saúde (Brasil). Conselho Nacional de Saúde. Resolução nº 196, de 10 de outubro de 1996. Diretrizes e normas reguladoras de pesquisa envolvendo seres humanos. Diário Oficial da União 16 out 1996.
6. Grandim CVC, Ferreira MBL, Moraes MJ. O perfil das grávidas adolescentes em uma Unidade de Saúde da Família de Minas Gerais. Rev APS. 2010;13(1):55-61.
7. Custódio G, Massuti AM, Shuelter-Trevisol F, Trevisol DJ. Comportamento sexual e de risco para DST e gravidez em adolescentes. DST j bras doenças sex transm. 2009;21(2):60-4.
8. Duarte HHS, Bastos GAN, Duca GFD, Corleta HE. Use of contraceptive methods by female adolescents in Restinga and Extremo Sul communities in Southern Brazil. Rev paul pediatr. 2011;29(4):572-6.
9. Saldanha AAW, Carvalho EAB, Diniz RF, Freitas ES, Félix SMF, Silva EAA. Comportamento sexual e vulnerabilidade à aids: um estudo descritivo com perspectiva de práticas de prevenção. DST j bras doenças sex transm. 2008;20(1):36-44.
10. Silveira MF, Béria JU, Horta BL, Tomasi E. Autopercepção de vulnerabilidade às doenças sexualmente transmissíveis e Aids em mulheres. Rev saúde pública [ Internet ]. 2002 [ cited 2013 Jan 10 ]36(6):670-7. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102002000700003&lng=en. http://dx.doi.org/10.1590/S0034-89102002000700003.
11. Cerqueira-Santos E, Paludo SS, Schirò EDB, Koller SH. Gravidez na adolescência: análise contextual de risco e proteção. Psicol estud. 2010;15(1):73-85.
12. Lima LHM, Viana MC. Prevalência e fatores de risco para a infecção por HIV, sífilis, hepatite B, hepatite C e HTLV-I/II em parturientes e gestantes de baixa renda atendidas na Região Metropolitana de Vitória, Espírito Santo, Brasil. Cad saúde pública. 2009;25(3):668-76.
13. Barros MEO, Lima LHO, Oliveira EKB. Prenatal care in the city of Quixadá: a descriptive study. Online braz j nurs [ Internet ]. 2012 [ cited 2013 Jan 16 ]11(2):319-30. Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/3782
14. Fonseca TMV, Cesar JA, Hackenhaar AA, Ulmi EF, Neumann NA. Corrimento vaginal referido entre gestantes em localidade urbana no Sul do Brasil: prevalência e fatores associados. Cad saúde pública. 2008; 24(3):558-66.
15. Pereira SVM, Bachior MM. Nursing Diagnoses identified in pregnant patients under prenatal care. Rev bras enferm. 2005;58(6):659-64.
16. Brandao VCRAB, Lacerda HR, Ximenes RAA. Frequência de Papilomavírus humano (HPV) e Chlamydia trachomatis em gestantes. Epidemiol serv saúde. 2010;19(1):43-50.
17. Figueiró Filho EA, Freire SSA, Souza BA, Aguena GS, Maedo CM. Sífilis e Gestação: estudo comparativo de dois períodos (2006 e 2011) em população de puérperas. DST j bras doenças sex transm. 2012;24(1):32-7.
18. Hernández BH, Boza AV, Cutié León E, Pineda ABA. Enfermedades de Transmisión Sexual y su relación con el embarazo. Rev cuba obstet ginecol. 1998;24(1):28-33.
19. Gonçalves CV, Duarte G, Costa JSD, Quintana SM, Marcolin AC. Perdas de oportunidades na prevenção do câncer de colo uterino durante o pré-natal. Ciênc saúde coletiva. 2011;16(5):2501-10.
20. Gonçalves CV, Costa JSD, Duarte G, Marcolin AC, Lima LCV, Garlet G, et al. Evaluation of the frequency of accomplishment of the breast examination and of oncotic cervical cytology and the obstetrical ultrasound during the prenatal period: an inversion of values. Rev Assoc Med Bras. 2009; 55(3):290-5.
Received: 06/02/2013
Approved: 01/05/2013