ORIGINAL ARTICLES
Complications related to the type of epicutaneous catheter in a cohort of neonates
Eny Dórea Paiva1, Amélia Fumiko Kimura2, Priscila Costa2, Talita Elci de Castro Magalhães3, Edi Toma2, Angelina Maria Aparecida Alves4
1Fluminense Federal University
2University of São Paulo
3Hospital and Maternity São Luiz
4Federal University of the State of Rio de Janeiro
ABSTRACT
Aims: To analyze the relationship between the type of epicutaneous catheter installed and the time until the occurrence of complications that motivate early removal of the device.
Method: Prospective cohort study conducted in a neonatal intensive care unit of a private hospital in the city of São Paulo, in the period July 1st 2010 to June 30th 2011. The cohort consisted of neonates undergoing the installation of polyurethane double-lumen or silicone single-lumen epicutaneous catheter.
Results and discussion: We analyzed 270 catheters. There was no association between the type of epicutaneous catheter and time until the occurrence of complications (p=0,45). The polyurethane double-lumen catheter presented higher average time of catheter permanence (p≤0,01).
Conclusion: Both types of epicutaneous catheters have enabled intravenous infusion over 10 days and showed no major complications.
Descriptors: Newborn, Central Venous Catheterization, Neonatal Nursing.
INTRODUCTION
In recent decades, technological advances in intravenous therapy in neonatology have been intensified, benefiting newborns (NB) at high risk that demand prolonged drug treatments intravenously infused, requiring a secure central venous access for it(1).
In this context, the peripherally inserted central catheter (PICC) or epicutaneous catheter was created to meet the therapeutic demands of critically ill neonates(1). This device provides a route for central venous access by means of the puncture of a peripheral vein of the upper or lower limb(1).
Since it is an invasive procedure, the use of PICC is not free of risk. Mechanical complications, including occlusion, extravasation, migration and thrombosis, occur in 15% to 48% of PICCs inserted(2).
For the population of newborns, catheters made of biocompatible materials such as silicone and polyurethane are available on the market. The catheters manufactured with silicone are those of a single lumen, with a diameter of 1.9 Fr and 3F. The polyurethane catheters may be single lumen with calibers of one or two French (Fr) and dual lumen with 2Fr(3).
The choice of the device should be based on the newborn’s clinical condition evaluation and also the infusion therapy. It is ideal that there should be no need for the nurse to an exchange the type of catheter during the patient's treatment time. In this context, the polyurethane double lumen PICC allows to infuse, simultaneously, incompatible drugs, avoiding multiple venous accesses and reducing the frequency of venipuncture infusions of these solutions. On the other hand, the single lumen catheter is indicated for the infusion of only one type of intravenous solution(4).
The literature suggests that the number of catheter lumens may be related to increased rates of catheter-related complications(5). Once the polyurethane catheter displays a greater number of lumens, there is a chance that complications, particularly those related to the manipulation of the catheter such as bloodstream infection and accidental traction, occur at a higher incidence when compared to silicone epicutaneous catheter of a unique lumen.
The nurse plays a central role in the insertion, maintenance, detection and treatment of epicutaneous-catheter-related complications. Whereas the double-lumen polyurethane catheter is a recent technology in neonatal units, the need to analyze the advantages and disadvantages of this type of catheter compared to the single-lumen silicone catheter is justified. Therefore, this study aims to examine the relationship between the type of epicutaneous catheter installed and the time until the occurrence of complications that motivate early removal of the device.
METHOD
This is a cohort study with prospective data collection. The cohort consisted of neonates who received silicone single-lumen PICC devices or polyurethane double lumen for prolonged intravenous therapy. The study was conducted in a NICU of a large hospital in the private network of the city of São Paulo, in the period from July 1st 2010 to June 30th 2011. All catheters that were introduced during that period were evaluated to be inserted into the study.
The NICU has 60 beds and the professional staff of the nursing team consists of 24 nurses and 124 nursing assistants and technicians. Of the total number of nurses, 22 are certified by a PICC installation qualification course. The monthly number of births in this institution is approximately 800 and approximately 30 PICCs are installed per month in the neonatal unit.
We considered eligible the neonates who were born in the maternity department and received one of two types of catheters studied, without a diagnosis of coagulopathies and congenital anomalies with loss of skin integrity.
The exposure variable was the type of epicutaneous catheter installed, silicone single-lumen or polyurethane double lumen. The silicone single lumen catheter had a caliber of 1.9 Fr (BD First PICC 26G / 1.9 Fr, 50cm - Beckton Dickinson, Utah, USA) and the two-way polyurethane catheter had a caliber of 2Fr, 1FR on each track and a single distal opening (Nutriline TwinFlo 24G/2Fr, 30cm - Vygon, Aachen, Germany). The choice of the type of catheter was in accordance with the assessment of the health team, respecting the clinical status and drug treatment of the newborn. The NB received a single lumen catheter when the drug therapy was composed of only one intravenous solution; and was given the double lumen catheter when intravenous therapy was composed of more than one type of intravenous solution, for example, parenteral nutrition and antibiotics.
The outcome variable was the need for removal of the device due to the occurrence of a complication that motivated the unplanned removal of the catheter. It was considered as unplanned removal when it was caused by complications such as obstruction, rupture, suspicion of catheter-related infection, thrombosis, traction or accidental drop, migration of the tip, edema, infiltration or hypoperfusion.
An obstruction was considered as the impossibility of permeabilizing the catheter with one ml of saline solution using a 10 ml syringe and absence of blood reflux through its lumen. Catheter rupture is the occurrence of a breach or hole in it. Tip migration is the displacement of the tip of the PICC confirmed by radiological images. Accidental traction is the total or partial inadvertent removal of the catheter.
The presence of bacteremia or fungal infection in a patient with a vascular device, and one or more positive results for peripheral blood culture or clinical manifestations of infection (fever, chills or hypotension), with no other apparent focus of bloodstream infection, was considered suspicious for infection of catheter-related bloodstream(4).
Edema of the extremities is the identification of mild to intense swelling around the site of the catheter insertion or the ends of the catheterized member during the stay of the device. Infiltration is the invasion of non-vesicant solution or drug in the extravascular space. Phlebitis is vein inflammation of a mechanical, chemical or bacterial source(4).
In compliance with Resolution No. 466/2012 of the National Health Council (NHC), which regulates the realization of research with human beings(6), the research project was approved by the Research Ethics Committee of the hospital, studied field (Protocol 219/10).
To record the data we used a specific form containing the variables of interest in the study: clinical diagnosis, weight and gestational age at the time of catheter insertion, classification of weight in relation to gestational age at birth, gender, postnatal age, type of the catheter installed, date of insertion, removal date and reason for removal. The newborns with a catheter were followed from insertion to removal of the device.
The collected data were stored in a Microsoft Office Excel 2007 spreadsheet and analyzed by means of the R software, version 3.0.1. The continuous variables were analyzed with descriptive statistics and categorical variables, by means of absolute and relative frequency. For the categorical variables, the existence of differences between groups and silicone single-lumen and polyurethane double lumen was determined by the chi-square test or Fisher's exact test. For continuous variables Student t test was used. The level of statistical significance was p<0.05 with 95% confidence interval. We calculated the number needed to cause harm (NNH), which case is an epidemiological measure that indicates how many people need to be exposed to a risk factor over a specified period of time to cause damage to a patient who would not otherwise have had damage. We estimated the survival functions by the product-limit method of Kaplan-Meier for the comparison of the time until the occurrence of catheter removal due to complications between the two groups. To compare the cumulative survival curves between the groups we used the log-rank test. Survival analysis is used in cohort studies and refers to the study of data related to the time until the occurrence of a particular event of interest, from a start time to an end time of a pre-defined study(7).
RESULTS
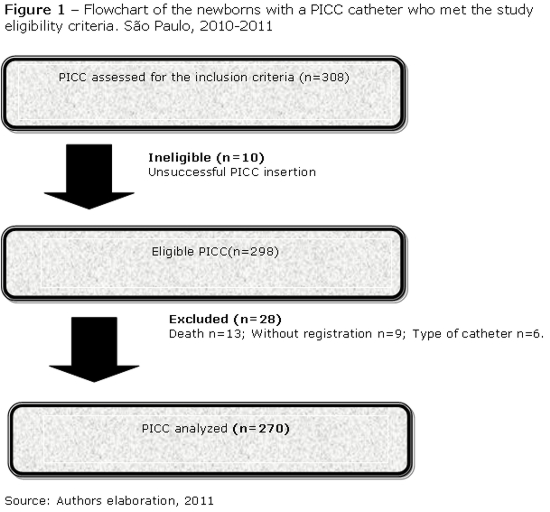
In the period studied, 308 PICC insertion procedures were evaluated, of which 10 procedures (3.2%) resulted in an unsuccessful installation. Among the 298 catheters successfully installed, we excluded 28 (9.4%) for the following reasons: silicone single lumen catheter 3.0 Fr and polyurethane single lumen 1.0 Fr, 6 (2.0%); absence of records in the institutional print-out for PICC catheter monitoring, 9 (3.0%); and death during catheter use, 13 (4.7%). Next the follow-up flowchart(8) of the installed PICC is presented (Figure 1).
The 270 PICC devices that met the eligibility criteria of the study were included in 213 neonates, 189 (70%) silicone single lumen catheters and 81 (30%) polyurethane double lumen catheters.
The neonates who composed the two groups of catheters were compared as to their characteristics in order to verify whether the populations had homogeneous clinical features. The variables characterizing the two groups of neonates are shown in Table 1.
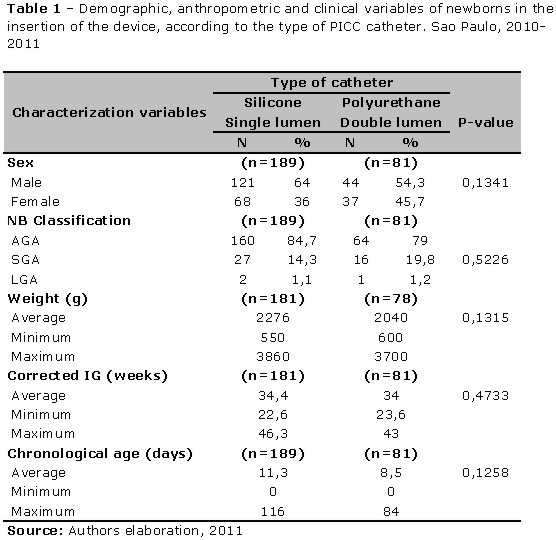
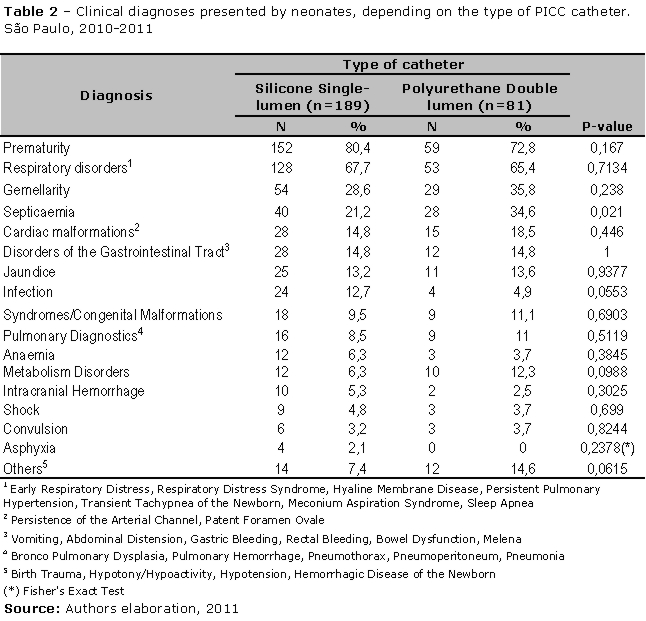
Table 2 shows neonates’ diagnoses. Prematurity and respiratory diseases were the most common diagnoses in both groups of catheters. There was a statistically significant difference between the newborns only regarding the diagnosis for septicemia.
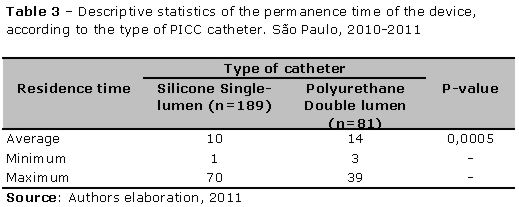
Regarding the average length of use of catheter, the data show that there were statistically significant differences between the groups. The neonates with polyurethane double lumen PICC had a higher average of catheter permanence.
The incidence of complications between the polyurethane PICC was 45.6%, and between the silicon catheters was 35.4%, with no statistical significance between the groups (p=.11). The relative risk found was 1.28 [CI, 0.95 to 1.75].
Table 4 presents data on the incidence rates of complications that occurred in the two groups of catheters studied.
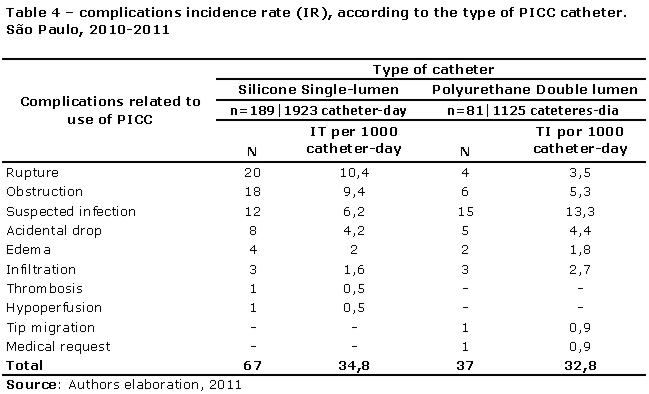
Once the incidence rate of complications in the silicone catheter group was 34.8/1000 catheter-day and 32.8/1000 catheter-day for the group of polyurethane catheter, the value of the attributable risk was 0,00196. Consequently, NNH was 51.02 in this study. This means that if 51 infants are exposed to the silicone catheter, only one will develop complications.
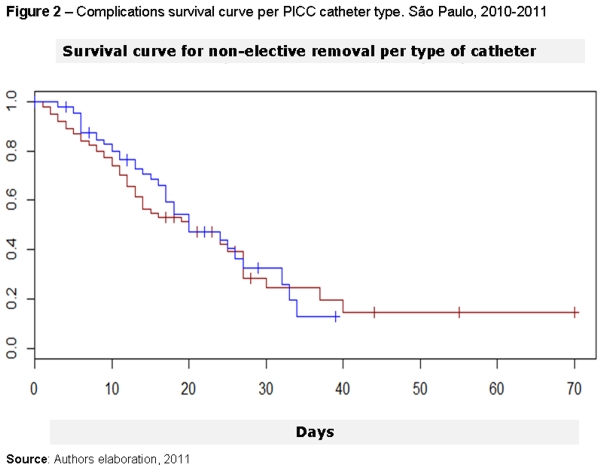
Despite the fact of the IT complications, the survival curve, was higher in the group of double lumen catheters for complications between the two types of catheters, it did not present a statistically significant difference (p=0.45). However, it is observed that up to approximately 20 days of catheter permanence, the group with double lumen PICC seems to provide a slightly higher cumulative survival rate when compared with the silicone single-lumen PICC.
DISCUSSION
The incidence of complications among the polyurethane PICC was 45.6%, and among the silicon catheters was 35.4%, with no statistical significance between the groups (p=0.11). The relative risk found was 1.28 [CI, 0.95 to 1.75]. However, as the confidence interval crosses the line of the no effect, the results suggests that there is no significant difference between the groups regarding the risk of complications regarding the use of the epicutaneous catheter in newborns.
It is essential for nurses to know the characteristics of vascular devices and learn how to adapt them to the needs of the patients, especially when it comes to premature neonates.
The ideal catheter should be one of small caliber and length, with the largest possible internal diameter (lumen), besides being flexible and biocompatible. Currently there is no material with ideal insertion and permanence properties, and therefore it is necessary to evaluate the advantages and disadvantages of each type of catheter before choosing which one to use.
Since the 2.0Fr polyurethane double lumen PICC is an intravenous device introduced in the Brazilian market in recent years, reports in the literature are scarce regarding the use of this catheter in the neonatal population. Since it has a less invasive character when compared to phlebotomy and has two independent pathways for the administration of intravenous therapy, we suggest that its use may benefit the neonatal population.
The epicutaneous catheter material can contribute to the intravenous therapy with some advantages and disadvantages. The polyurethane catheters have higher stiffness, increased chemical resistance, moldability, biostability and also low thrombogenicity(9). By presenting thinner walls and greater luminal diameter, the catheter provides greater speed in infusion solutions and increased length of stay in the patient(10).
In this study, the removal of the catheter for suspected infection is the most frequent complication between the double lumen catheters (13.3/1000 catheter-day). Slightly higher incidence rates were observed in a prospective study with 226 neonates who underwent insertion of 302 PICCs for venous access and infusion of parenteral nutrition in a tertiary NICU in London (England). The results of the study point out that the infection incidence rate of catheter-related bloodstream was 17 per 1,000 catheter-days(11).
Although there was no difference between the two types of epicutaneous catheter as to the time until the occurrence of non-elective removal, there was a higher incidence rate of this complication among double lumen catheters. One of the explanatory hypotheses would be the greater number of lumens, which may represent an additional input port for infection. However, the double lumen catheters also had a higher average dwell time compared to the single lumen ones. This is a retrospective cohort study, conducted with 683 infants with PICC, aiming to verify whether the risk of bloodstream infection related to the catheter stays constant over time, and therefore we suggest that the time of catheter permanence is an important risk factor for infection in the NICU. There was a significant increase in risk after 35 days of PICC insertion(12).
The bloodstream infection related to the use of PICC is a risk inherent in the use of a vascular access device(4). Many infections related to PICC are not diagnosed or become recognizable only when the patient presents severe sepsis. The manifestations can be both local and systemic. The signs of local infection include redness at the site of insertion, pain and exudation, and the systemic signs include fever and clinical deterioration(10).
The prevention of infections related to PICC includes practices such as hand hygiene, maximal barrier precautions during insertion, antisepsis with chlorhexidine, proper selection of the catheter insertion site, daily review of the need of catheter permanence with removal, weekly changing of the PICC sterile occlusive dressing or when it loses its adhesion(4).
There is controversy over the form of treating catheter-related bloodstream infection among neonates who require vascular access for their survival. However, literature recommends some alternatives to be analyzed case by case. One option is to treat infections with antimicrobial agents by means of a catheter and to repeat the blood culture after 48 hours. If there is persistent infection, considering the removal of the catheter is one of the indications. There are cases in which the use of the catheter without a treatment attempt is discontinued, especially fungal infections. A new catheter may be introduced 24 to 48 hours after the onset of systemic treatment. Treatment with antibiotic lock showed decreased infection, but still needs more scientific evidence for its recommendation(4).
Another study evaluating epicutaneous double lumen catheters, but with 3.0Fr, aimed to report the experience of inserting the PICC in 61 neonates and to analyze the technical characteristics of the procedure and its complications. The results showed that elective removal occurred in 45.9% of the catheters. The reasons for non-elective removal were: phlebitis and edema in 21.3% of catheters inserted, suspected infection in 3.2%, accidental traction in 3.2% of the catheters and distal end rupture of 3.2% of the epicutaneous catheters(13).
Regarding complications, in the group of silicone single-lumen catheters, the most frequent ones were rupture and obstruction. These findings corroborate with the results of a prospective cohort study conducted in the NICU of the state of São Paulo, which evaluated 237 epicutaneous polyurethane and silicone catheters, demonstrating an incidence rate of 6.2/1000 catheter-day(14). Another survey conducted in Taiwan evaluated 412 silicone PICC in 267 neonates weighing ≤1500g and found an incidence rate of obstruction of 4.0/1,000 catheter-day(15).
Possibly, the characteristics of flexibility and manageability of the silicone makes it more vulnerable to these types of complications. The resistance of the catheter is directly related to the size and type of device material of the PICC(16).
The catheter made from silicone has higher flexibility compared to polyurethane, offers less irritation to the vascular wall and less drug interaction(9). It is also heat stable, has high resistance to bending, low thrombogenicity and bacterial adherence(9). It features a smaller inner diameter compared to the polyurethane catheter of the same external diameter, a characteristic that complicates and delays the time of infusion of blood components and intralipids due to its higher viscosity. Even saline solutions may present difficulties in the flow(9).
The catheter obstruction can be caused by several factors, including the position of the PICC, thrombus formation, precipitation of drugs, and the presence of colonies of microorganisms on its tip(17, 18).
The care that the professional involved in the maintenance of PICC should dispense to patients with a PICC device is extremely important, in order to prevent complications related to its use. The main obstruction prevention strategy is the meticulous permeabilization of the catheter. The administration of a saline solution before and after the administration of the drug is a routine in the maintenance of the PICC care. This is to prevent drug incompatibility that can generate intraluminal obstruction and rupture of the catheter(4,19).
It is worth noting that obstruction and rupture are preventable complications. Prevention strategies include proper adhesion of the PICC dressing, keeping the site of insertion of the device clean and dry, keeping catheters well connected, avoiding forced pressure on the syringe connected to the catheter, avoiding performing flush maneuver if resistance to the infusion is observed, removing the catheter gently and holding it near the insertion site, but not its cannon(19).
However, the professionals responsible for intravenous therapy need to decide, according to their care practice and the material availability at their institution, what kind of device meets the needs of the service and patients, aiming mainly for increased safety, durability, resistance to pressure and reliability.
It is necessary to point out the limitations of this study: unicentric character and data collection through records of the health care team in medical records, which may allow the occurrence of data loss due to the non-recording of information of interest to the study. Furthermore, there was a greater proportion of polyurethane dual lumen catheters. However, despite the limitations, the findings deserve to be better explored in subsequent studies, given the scarcity of studies related to the safety and efficacy of the use of different types of PICCs in neonates and in other populations.
CONCLUSION
The results of the study indicate that the time until the occurrence of non-elective removal did not differ between the two types of epicutaneous catheters. However, there was statistically significant difference in the average time of permanence between the two types of catheters, indicating that possibly the polyurethane double lumen device contributes for a longer period of time to vascular access for the intravenous infusion of solutions needed by newborns.
There is a variety of catheters available in the market, and a lack of studies that comparatively evaluate their safety and cost-effectiveness, thus preventing the establishment of scientific evidence to support the best choice of the type of device for each patient. However, both types of epicutaneous catheter allowed intravenous infusion for more than 10 days and no serious complications have occurred.
However, the polyurethane epicutaneous double-lumen catheter seems to be a good option for central vascular access for neonates requiring the infusion of multiple concomitant drugs. Since most of the complications are preventable and not serious, such as obstruction, external rupture, suspicion of infection and accidental traction, it is necessary for the nursing staff to prevent and monitor this vascular device as to the early signs of these complications as, for example, increased resistance for infusion, loss of dressing adhesion, connection disinfection, use of gloves, hand washing, use of appropriate caliber syringes (10 mL).
It is extremely important for nurses to know the devices available in the institution where they work, evaluating the patient and the drug treatment prescribed, so that they can choose the most appropriate type of PICC. It is recommended that health services have nurse specialists in intravenous therapy and care of vascular devices, in addition to evidence-based protocols that support the practice of professionals.
Acknowledgment
We thank The National Council for Scientific and Technological Development (CNPq) for funding the Research Project (CNPq Process 480398/2012-7), from which were extracted the data of this study.
REFERENCES
1. Hoang V, Sills J, Chandler M, Busalani E, Clifton-Koeppel R, Modanlou HD. Percutaneously inserted central catheter for total parenteral nutrition in neonates: complications rates related to upper versus lower extremity insertion. Pediatrics.2008;121(5):1152-9.
2. Shah PS, Shah VS. Continuous heparin infusion to prevent thrombosis and catheter occlusion in neonates with peripherally placed percutaneous central venous catheters. Cochrane database syst rev[ online ]. 2009[ cited 2013 Nov 28 ]16(2):[ about 10.p ].Available from:http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD002772.pub3/abstract
3. Dorea E, Castro TE, Costa P, Kimura AF, Santos FMG. Management practices of peripherally Inserted central Catheter at a neonatal unit. Rev Bras Enferm [ online ] 2011[ cited 2013 Nov 27 ] 64(6)997-1002. Available from: http://www.scielo.br/scielo.php?script=sci_abstract&pid=S0034-71672011000600002&lng=pt&nrm=iso&tlng=en
4. Pettit J, Wyckoff MM. Peripherally inserted central catheters:guideline for practice. 2nd ed. Glenview: National Association of Neonatal Nurses; 2007.
5. Barrier A, Williams DJ, Connelly M, Creech CB. Frequency of peripherally inserted central catheter complications in children. Pediatr infect dis J. 2012;31(5):519-21.
6. Conselho Nacional de Saúde (Brasil). Resolução n. 466, de 12 de dezembro de 2012. Diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Diário Oficial da União 13 jun 2013; Seção 1.
7. Coeli CM, Faerstein E. Estudos de coorte. In: Medronho RA, Boch KV, Luiz RR, Werneck GL. Epidemiologia. São Paulo: Atheneu; 2009. p.237-50.
8. Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)statement: guidelines for reporting observational studies. J clin epidemiol. 2008 Apr; 61(4):344-9.
9. Camargo PP. Procedimento de inserção, manutenção e remoção do cateter central de inserção periférica em neonatos. São Paulo. Dissertação[ Mestrado em Enfermagem Obstétrica e Neonatal ]- Universidade de São Paulo; 2007.
10. Giacomo M. Comparison of three peripherally inserted central catheters: pilot study. Brit j nurs.2009;18(1):8-16.
11. Njere I, Islam S, Parish D, Kuna J, Keshtgar A. Outcome of peripherally inserted central venous catheters in surgical and medical neonates. J ped sur. 2011;46:946-50.
12. Sengupta A, Lehmann C, Diene-West M, Perl TM, Milstone AM. Catheter duration and risk of CLA-BSI in neonates with PICCs. Pediatrics.2010;125(4):648-53.
13. Bueno TM, Cervera PQ, Pérez-Rodríguez J, Quero J. Peripheral insertion of Double-lumen central venous catheter using the Seldinger technique in newborns. J perinatol. 2008;28(4):282-6.
14. Costa P. Análise da relação entre a posição anatômica da ponta do cateter CCIP e o motivo de remoção do dispositivo em uma coorte de neonatos. São Paulo. Dissertação[ Mestrado em Enfermagem ]-Universidade de São Paulo; 2011.
15. Hsu JF, Tsai M, Huang H, Lien R, Chu S, Huang C. Risk factors of catheter-related bloodstream infection with percutaneously inserted central venous catheters in very low birh weight infants: a center´s experience in Taiwan. Pediatr neonatol. 2010;51(6):336-42.
16. Pettit J. Assesment of infants with peripherally inserted central catheters: part 2. Detecting less frequently occurring complications. Adv neonatal care. 2003;3(1):14-26.
17. Paulson PR, Miller KM. Neonatal peripherally inserted central catheters: recommendation for prevention of insertion and post insertion complications. Neonat Netw. 2008;27(4):245-57.
18. Ormond VS, Azevedo RCS, Gaiva MAM, Oliveira DFL. Profile of newborns who used Peripherally Inserted Central Catheter (PICC) in a University Hospital. Online braz j nurs [ Internet ]. 2010 December [ Cited 2013 Sept 17 ] 9 (3): Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/3137. doi: http://dx.doi.org/10.5935/1676-4285.20103137. Infusion Nurses Society.
19. Infusion nursing standarts of practice. J intraven nurs. 2011;34(1): [ about 100.p ]. Avalaible from: http://www.vardhandboken.se/Dokument/INS_2011.pdf
Received: 09/10/2012
Revised: 15/05/2013
Approved: 17/09/2013