
ORIGINAL ARTICLES
Understanding of technical education level professionals regarding sickle cell disease: a descriptive study
Ludmila Mourão Xavier Gomes1, Magda Mendes Vieira2, Tatiana Carvalho Reis2, Thiago Luis de Andrade-Brabosa2, Antônio Prates Caldeira2
1Minas Gerais Federal University
2Montes Claros State University
ABSTRACT
Aim: To assess the understanding of technical education level professionals who work in Primary Health Care units regarding sickle cell disease in children.
Method: This is a descriptive and transversal study, involving 357 health community agents and nursing technicians who responded to a structured questionnaire. The performance was tested in terms of the average score for every stage of the questionnaire.
Results: The average score was below 65% in all stages, with critical results in the stages “clinical manifestations” and “management of children with sickle cell disease”. There was a statistical association between the best performance and the following variables: role in the team (OR=5.92; IC95%=1.90-20.49) and the level of interaction with the sickness (OR=1.71; IC95%=1.09-2.69).
Discussion: The professionals must be able to assist children with sickle cell disease.
Conclusion: The lack of information on the part of the professionals that care for and handle children with sickle cell disease, indicates the need to develop these professionals in such a way as to improve the quality of the service provided.
Descriptors: Sickle Cell Anemia; Children; Knowledge; Quality in Health Care; Primary Health Care.
INTRODUCTION
Sickle cell disease is a hemoglobinopathy that represents an important public health issue in Brazil and around the world due to its elevated morbimortality(1). In Brazil, there is an estimated falciform trace on the general population of between 2% and 8%, and between 25,000 to 30,000 cases sickle cell anemia have been found(2).
Historically, a patient with sickle cell disease makes use of hemotherapy services(3,4). However, it is preferable if such a patient makes use of both hemocenters and primary health care (APS, in Portuguese) services. The development of a bond between the patient and relatives with the health team is fundamental, in order to help to understand the disease, to anticipate risky situations and to avoid complications that may lead to hospitalization.
Nowadays, the reorganization of the assisting model in Brazil focuses on two basic objectives: the emphasis on primary care as the entrance to health services in general, and the emphasis in the promotion of health. The Family Health Strategy (ESF, in Portuguese) integrates multi-professional health teams which have a fundamental role in this strategy. These teams must work mainly to promote health and to prevent the worsening of illnesses. They can also provide good support to the patient with sickle cell disease and to his relatives(5). Some authors report that the introduction of the ESF to this group of patients is a valid strategy in order to improve the health services provided, as these patients have to endure environmental and other intrinsic factors related to this chronic disease(3,6). ESF can have a prominent role in monitoring nutritional conditions, as well as in the improvement with regard to adherence to prophylactic antibiotic therapy as directed to these patients(5,6).
Besides doctors, nurses and dentists, the ESF teams also include important professionals with a technical educational level. Nursing technicians are responsible for developing preventive actions and for promoting health in addition to the supervision of healing tasks. This professional must be the individual who builds the link between the community, patients and their families with the health services, and must act as the go-between in terms of the knowledge (biomedical practices) and the culture of the place in which this professional works(7). From this perspective, the community health agents (ACS, in Portuguese) must act as a facilitator, being able to build bridges between the health services and the community, promptly identifying any problems, working to prevent diseases, and promoting health.
Although literature in this topic is very limited, it is observed that there is a growing interest in the role and in the tasks allocated to technical education level professionals in Brazil, especially to ACS.
On the follow-up of children with sickle cell disease, it is basically expected that these professionals are able to perform home visits tailored to the peculiarities of the patient with sickle cell disease, guiding the family regarding the use of folic acid, the prophylactic use of penicillin, the prevention of infections, the caring about the environment and physical activities, and the scheduling of evaluation consultations with regard to growth and development, among other tasks.
Considering the relevance of the tasks undertaken by technical education level professionals (nursing technicians and ACS) in the family health teams, and the fact that sickle cell disease is a public health issue that disrupts family dynamics, the present study aims to evaluate the understanding of these professionals with regard to sickle cell disease in children.
METHOD
This is a descriptive and transversal study, developed in the municipality of Montes Claros, located on the north of the Brazilian state of Minas Gerais. The municipality is the main urban center of the region, with an estimated population of 360,000 inhabitants. The city is a focal point in terms of health services for the whole region and features a concentration of the second largest number of patients with sickle cell disease in the state. With regard to the Family Health network, the city has 52 complete ESF teams in the urban area, and seven in the surrounding rural area. For this study, all nursing technicians and community health agents from the family health teams within the urban zone were considered eligible. The criterion for exclusion was if a professional was away on vacation or missed a shift during the collection of the data. Data collection was undertaken during the second semester of 2010. In order to collect the data, we used a questionnaire built from the guidelines drawn up by Secretary of State for Health of Minas Gerais and the Brazilian Ministry of Health(7-8). In order to validate the content, the instrument was reviewed by five professionals - two specialists (one hematologist doctor and one nurse specializing in hematology), two pediatricians, and one nurse who works in Primary Care. The review considered the presence or lack of criteria in terms of coverage, objectivity and relevance. To check the adequacy and viability of the questionnaire, a pilot study was performed with professionals from family health teams from the rural zone.
To characterize the participants, the following variables were used: gender (male/female); age (years); marital status (married or in stable relationship/single or separated/widow); function in ESF (community health agent/nursing technician or auxiliary); time working in Primary Care (years) and; the level of interaction with sickle cell disease. This last variable represents the existence of a closer contact/previous interaction with the studied illness, and it was measured by questions to the professionals prior to the moment they answered the question about how much they knew about sickle cell disease. The level of interaction was classified as: none/zero (never heard about sickle cell disease), light (has heard about sickle cell disease), moderate (knows someone with sickle cell disease), b (has relatives diagnosed with sickle cell disease).
The level of understanding with regard to sickle cell disease was observed from the evaluation of true or false statements regarding the key aspects of the guidelines regarding primary care. Each statement marked correctly added one point to the total score with regard to 37 questions. The questionnaire was divided in three domains: epidemiology (8 questions), clinical manifestations (9 questions), and management of children with sickle cell disease (20 questions). The performance in the test was checked through a total of correct answers to the questions. To better ascertain the level of professional knowledge, the total scores were categorized according to results above and below average. Pearson’s chi-square test, with Yates’ correction or Fisher’s exact test, were used to check the association of the dependent variable (performance above/below average) against the other variables. The level of significance adopted was 5%. To analyze the data, we used Statistical Package of Social Science (SPSS®) software, version 16.0 (license code 550c48f4c442018490b8) and Epi Info® software, version 3.15, which helped the statistical analysis of this study.
Ethical considerations were respected. The participation in the research was voluntary after signing a free and clear consent agreement. This present study was submitted for consideration by the Committee of Ethics in Research of Montes Claros State University (Unimontes, in Portuguese), and approved under Consubstantial Notion #1517/2008.
RESULTS
In the municipality, there were 392 professionals (nursing technicians and ACS) placed in Family Health teams in the urban area. In this research, 357 professionals (91%) participated, which included 30 nursing technicians, 319 ACS and eight who did not include their role. 28 professionals were excluded from this research because they were absent during the period of data collection, and seven did not agree to participate in this study (Diagram 1). The number of professionals who participated was, on average, 6.8 (SD=1.8) for each ESF team.
Among the selected professionals, there was a predominance of females (298; 83.5%). The average age was 31.4 years. The marital situation of the majority was married/in stable relationship status (189; 52.9%) and the many had children (217; 60.8%). The median of service time in the APS was 3 years (1.00-5.00). The profile of the professionals is presented in Chart 1.
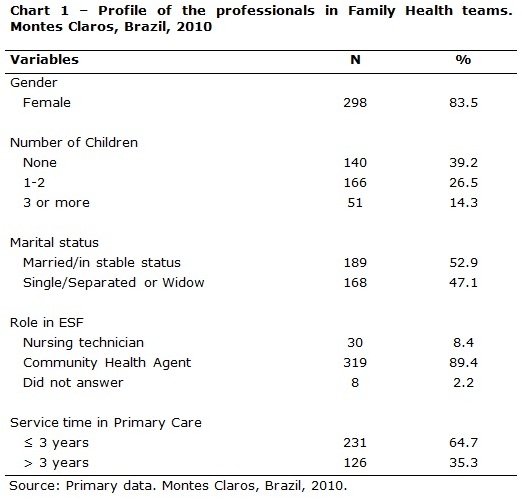
The level of the previous interaction of the respondents with the studied pathology was evaluated as: none, for 19 professionals (5.3%), light, for 185 professionals (51.8%), moderate, for 134 professionals (37.5%), and b, for 19 professionals (5.3%).
The understanding of the professionals was demonstrated by the average performance on the tests applied, which was below 65% for the three domains observed. The professionals obtained an average performance in the domains “clinical manifestations of sickle cell disease” (53.3%) and “management of children with sickle cell disease” (50.0%), which was a cause for concern. The averages and percentages of the correct answers are seen in Chart 2.
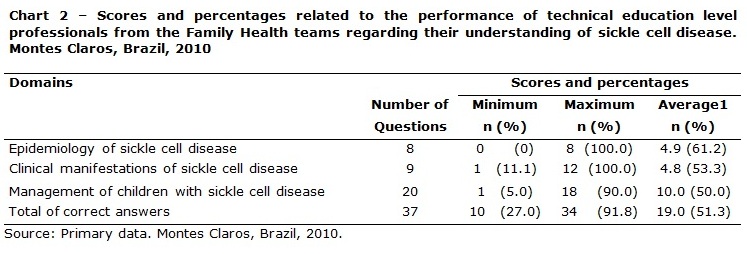
Chart 3 shows the relationship between the professional characteristics of the respondents and their test results.
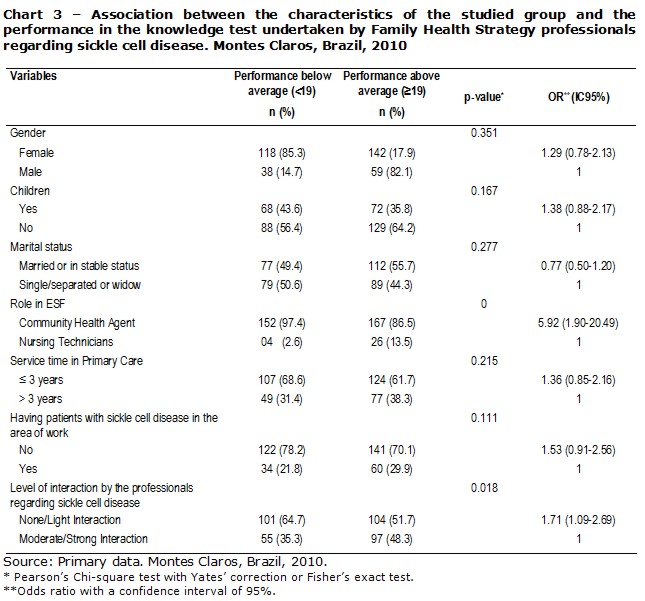
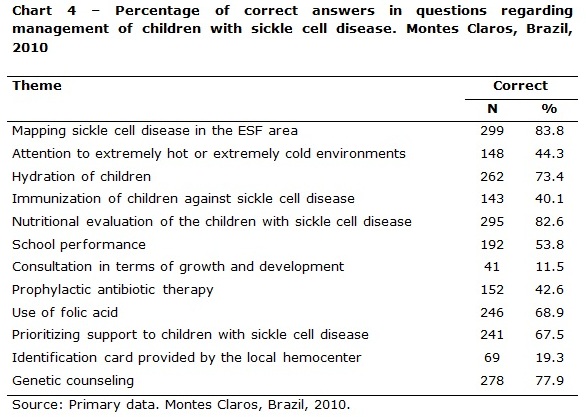
There is a meaningful statistical association for the variables “role in ESF” (p=0.000) and “level of interaction by the professionals regarding sickle cell disease” (p=0.018). Chart 4 refers to the proportion of correct answers to key questions regarding the understanding of caring for children with sickle cell disease. Among the items mentioned, we highlight those with a lower proportion of correct answers on the part of the technical education level professionals: follow up from consultation of growth and development, immunization, attention to the environment, school development, use of folic acid, prophylactic antibiotic therapy, prioritization in caring, and the use of identification cards.
DISCUSSION
In this study, it was possible to evaluate the level of understanding regarding sickle cell disease on the part of technical education level professionals who work in primary healthcare. This fact indirectly translates into the quality of the healthcare service provided to the patients, for whom these professionals are responsible. We highlight the fact that the questions used were created on the basis of official directives(8-9) regarding sickle cell disease, which implies that the evaluated professionals disregard such directives. The level of understanding of the professionals, shown by the average performance on the applied tests, was below 65% on all three domains studied.
The performance of the professionals in each stage of the knowledge test draws special attention to the domains “clinical manifestations” and “management of children with sickle cell disease”, for which the average percentage scores were 53.3% and 50%, respectively. The professionals who are part of Primary Care must be aware of the different manifestations of the illness, the risk to life, and management aspects, in order to reduce the frequency and the severity of the crisis and the resulting complications by being able to undertake an immediate investigation(10). Studies performed with APS professionals show little understanding on the part of the nurses and doctors about the disease(11-14). However, there are no studies that evaluate technical education level professionals such as ACS and nursing technicians regarding sickle cell disease, as was observed in this study.
With the reorganization of the APS network in Brazil, and the organization and standardization of caring guidelines with regard to chronic patients, it is fundamental to stress the importance of nursing technicians and ACS in order to ensure better results. ESF is understood to provide a complete assistance in regions/determined geographic areas and, to perform as such, this service incorporates ACS.
These professionals lack information in the area of health, and it is a responsibility of local SUS (acronym, in Portuguese, for Brazilian Unified Public Health System) public administrators to ensure the permanent formation, qualification and education of these professionals while in service(7,15). ACS, inserted in the context of the transformation of the model of health care, and as a member of the multiprofessional health team, is the mediator between the health system and the family/community. S/he has the potential to establish a link with the users, as they live in the area covered by the Family Health Unit.
With regard to sickle cell disease, within primary care, it is expected that directed home visits are performed, with effective measures to control pain, be aware of signs/symptoms of illness, and various educational roles in addition to genetic counseling and the prevention of infections, follow-up of prophylaxis with antibiotics, vaccination and screening in order to prevent strokes(3,6,14). The ESF social actors are important in this process.
The best performance of the professionals in the knowledge test was related to the variable “level of interaction of the professionals with sickle cell disease”. The absence of interaction and light interaction rates with the disease (OR=1.71; IC95%=1.09-2.69) was related to the low scores in the knowledge test when compared to moderate and b interaction rates. This association indicates that the higher is the association or interaction of the professionals with sickle cell disease in their routine, the better is their performance in the test.
It was verified that ACS (OR=5.92; IC95%=1.90-20.49) achieved a lower than average performance when compared to nursing technicians. The significant statistical difference found in the level of understanding between them was expected, but not desired. This difference regarding the level of understanding, forces us to look to the development of these people as professional ACS. They are part of a multiprofessional health team in ESF, and their role is not based on the disease, but on the sick person or on those with the possibility of falling ill. On the other hand, the nursing technician is trained differently is specialized in the area of health, prepared to assist in healing tasks, and in preventing and promoting health(7,15).
From this perspective, it is suggested that these professionals should be included in the process of permanent learning, educating them in sickle cell disease. These professionals offer a great potential in terms of health promotion and preventive actions(14).
Another reflection done in this study is about the spaces for discussion in thematic areas in the ESF, which are described as permanent education spaces. We question if these spaces are really used for discussing the role of the ESF teams, especially in dealing with clients with sickle cell disease.
With regard to caring for children with sickle cell disease, we mention three prophylactic measures that are widely recommended in the work against sickle cell disease. These are prophylaxis with penicillin, basic immunization and with special immunobiological drugs, and the use of folic acid(16).
The performance of the participants regarding immunization (143; 40.1%) was considered critical. A child with sickle cell disease must be given the vaccines according to the basic vaccination calendar, together with special immunobiological drugs, such as the vaccines against pneumococcus, meningitis and influenza(8,16). The lack of understanding regarding the need for special immunibiological drugs implied by the lack of a follow up in vaccine coverage and, as a consequence, the increased risk of complications associated with some specific illnesses(1,17).
The use of prophylactic antibiological therapy by ESF professionals is relevant in terms of preventing the high rates of morbidity and mortality as a result of pneumococcal diseases and other infections(5,16). Some studies report that adherence to this treatment has been a challenge to health professionals(18-19). When observing the index of correct answers (42.6%) with regard to this question, it was seen that the professionals are not ready to motivate clients when it comes to adherence to a prophylactic antibiologic therapy.
With regard to the follow-up in terms of growth and development, it was seen that the majority of the respondents (82.6%) are aware of the importance of this task for children with sickle cell disease. Many authors point to the deficit in growth that a child with sickle cell disease presents at two years of age. This is described as a retardation of somatic growth that affects weight more than height, and is progressively accentuated until the client is 18 years old(5,20).
The lack of knowledge regarding nutritional follow-up can influence the actions needed to promote health. However, in the question linked to the calendar of consultation of children with sickle cell disease, a lack of awareness of this calendar was detected on the part of 316 of the professionals (88.5%). The guidelines in the Brazilian state of Minas Gerais(8) lay down that the follow-up consultations linked to growth and development must be done on a monthly basis for children up to one year of age. Later, these consultations must be every three months until the child reaches five years of age. For children above this age, the state recommends consultations every four months. The lack of awareness of this guideline suggests that the calendar is not doing the job it is supposed to do, and that the correct number of consultations are not being carried out.
When questioned about the attention to extremely hot or extremely cold environments, only 148 professionals (44.3%) answered the question correctly. The low percentage of right answers to this question points to a probable lack of orientation of the family to some important factors that precipitate vase-occlusive crises. Some precipitant factors of these crises that are described in literature and that are of extreme relevance with regard to the families are emotional stress, fatigue, dehydration, exhausting physical exercise, extremely hot or cold temperatures, and high altitude(3,16).
When questioned about prioritization when it comes to caring for a child in the presence of at least one warning sign, it was seen that the proportion of correct answers was above 67.5%. Even with a better performance in this matter, the understanding of technical education level professionals is not yet considered to be adequate.
To perform the recommended actions in healthcare, it is necessary to have full understanding. The low percentage of correct answers on the part of the nursing technicians and ACS in regard to the majority of variables studied here, leads to the fact that these professionals do not have sufficient understanding to assist children with sickle cell disease, which indirectly leads to a bad result in terms of assistance to the risk group studied. From this perspective, we suggest the need for an urgent updating in the knowledge of these professionals.
CONCLUSION
This study evaluated the understanding of ACS and nursing technicians regarding sickle cell disease, and also provides information that can relate to future qualifications and permanent education. The provision of workshops is recommended for these professionals, aiming at providing information and care for children with sickle cell disease and their relatives.
The limitations of this present study are related to the data collection instrument developed by the researchers, as it was seen that there were no validated instruments to observe the topic under consideration. Another limitation is the fact this study was limited to only one municipality.
It is necessary to provide a permanent education of health professionals in primary care through an approach to caring methodology, and guidelines for the patients with sickle cell disease and their relatives. It would also be desirable for new studies to be undertaking that test the level of knowledge before and after the training of professionals, in order to support the discussion regarding this topic.
REFERENCES
1. Fernandes APPC, Januário JN, Cangussu CB, Macedo DL, Viana MB. Mortality of children with sickle cell disease: a population study. J pediatr (Rio J). 2010; 86(4): 279-84.
2. Cançado RD, Jesus JA. A doença falciforme no Brasil. Rev bras hematol hemoter. 2007; 29(3): 204-6.
3. Kikuchi BA. Assistência de enfermagem na doença falciforme nos serviços de atenção básica. Rev bras hematol hemoter. 2007; 29(3): 331-8.
4. Cruz ICF. Saúde da população negra: a construção da equidade no SUS pela implementação da Política Nacional de Saúde Integral da População Negra. Online braz j nurs [ Internet ]. 2010 [ cited 2012 Ago 01 ] 9(3). Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/j.1676-4285.2010.3194/html.
5. Souza KCM, Damião JJ, Siqueira KS, Santos LCS, Santos MR. Acompanhamento nutricional de criança portadora de anemia falciforme na Rede de Atenção Básica à Saúde. Rev paul pediatr. 2008; 26(4): 400-4.
6. Xavier-Gomes LM, Reis TC, Vieira MM, Andrade-Barbosa TL, Caldeira AP. Quality of assistance provided to children with sickle cell disease by primary healthcare services. Rev bras hematol hemoter. 2011; 33 (4):277-82.
7. Nascimento EPL, Correa CRS. O agente comunitário de saúde: formação, inserção e práticas. Cad saúde pública. 2008; 24(6): 1304-13.
8. Secretaria de Estado de Saúde de Minas Gerais. Atenção à saúde da criança: doença falciforme. Belo Horizonte: SAS/DNAS; 2005.
9. Ministério da Saúde. Manual de Educação em Saúde. Brasília (DF): Ministério da Saúde; 2008.
10. Khattah AD, Rawlings B, Ali IS. Care of patients with haemogiobin abnormailities: nursing management. Br J Nurs. 2006; 15 (19): 1057-62.
11. Ratanawongsa N, Haywood Jr C, Bediako SM, Lakshmi L, Lanzkron S, Hill MP, et al. Health care provider attitudes toward patients with acute vaso-occlusive crisis due to sickle cell disease: Development of a scale. Patient Educ Couns. 2009; 76 (2):272–8.
12. Dennis-Antwi JA, Dyson S, Ohene-Frempong K. Healthcare provision for sickle cell disease in Ghana: challenges for the African context. Diversity in Health and Social Care. 2008;5 (4):241–54.
13. Weinreich SS, Klerk ESML, Rijmen F, Cornel MC, Kinderen M, Plass AMC. Raising awareness of carrier testing for hereditary haemoglobinopathies in high-risk ethnic groups in the Netherlands: a pilot study among the general public and primary care providers. BMC Public Health [ Internet ]. 2009 [ cited 2012 Nov 10 ] 9(338):1-9. Available from: http://www.biomedcentral.com/content/pdf/1471-2458-9-338.pdf.
14. Xavier-Gomes LM, Vieira MM, Reis TC, Andrade-Barbosa TL, Caldeira AP. Knowledge of family health program practitioners in Brazil about sickle cell disease: a descriptive, cross-sectional study. BMC Fam Pract [ Internet ]. 2011 [ cited 2012 jan 12 ] 12 (89):1-7. Available from: http://www.biomedcentral.com/content/pdf/1471-2296-12-89.pdf.
15. Santos LPGS, Fracolli LA. O agente comunitário de saúde: possibilidades e limites para a promoção da saúde. Rev esc enferm USP. 2010; 44(1): 76-83.
16. Araujo PIC. O autocuidado na doenca falciforme Sickle cell disease and the self care. Rev bras hematol hemoter. 2007; 29(3):239-46.
17. Lucas SB, Mason DG, Mason M, Weyman D. A sickle crisis? a report of the National Confidential Enquiry into Patient Outcome and Death [ Internet ]. London: National Confidential Enquiry into Patient Outcome and Death; 2008 [ cited 2012 Jan 20 ]. Available from:http://www.ncepod.org.uk/2008report1/Downloads/Sickle_report.pdf.
18. Bitarães EL, Oliveira BM, Viana MB. Adesão à antibioticoterapia profilática em crianças com anemia falciforme: um estudo prospectivo. J pediatr (Rio J). 2008; 84(4): 316-22.
19. Strayhorn G, Farley KSMM, Adamkiewicz TV, Silk BJS, Howgate J, Baughman W. Effectiveness of the 7-Valent Pneumococcal Conjugate Vaccine in Children With Sickle Cell Disease in the First Decade of Life. Pediatrics. 2008;121(3):562-9.
20. Dick MC. Standards for the management of sickle cell disease in children. Arch Dis Child Educ Pract Ed. 2008; 93(6):169–76.
Received: 03/09/2012
Revised: 16/03/2013
Approved: 28/05/2013