REVIEW ARTICLES
Nursing diagnoses of patients with heart failure: an integrative review
Ana Carla Dantas Cavalcanti1, Juliana de Melo Vellozo Pereira1
1Fluminense Federal University
ABSTRACT
Aim: To identify the information produced and published in the Brazilian and international literature regarding the diagnoses of nurses in the case of hospitalized patients with heart failure.
Method: This is an integrative review without a defined time frame, performed with regard to the consultation of the following databanks: CINAHL, MEDLINE, SCOPUS, LILACS, Web of Science, CAPES Thesis Bank, USP Thesis Bank and BIREME.
Results: 24 studies were selected and analyzed. Decreased cardiac output, excessive fluid volume, activity intolerance, impaired skin integrity, impaired gas exchange, efficient knowledge, risk of falls and impaired physical mobility were the most frequently mentioned diagnoses in the studies that were analyzed.
Discussion: The results match the progression of heart failure, which limits the tolerance of the individual to physical exercise and causes water retention.
Conclusion: This evidence will contribute to guiding nursing care and to the development of caring protocols.
Descriptors: Nursing Diagnose, Heart Failure, Hospitalized Patients.
INTRODUCTION
In the Brazilian Unified Health System in Brazil, cardiovascular diseases (CVD) represent one of the main causes of hospitalization, with heart failure (HF) being the most frequent pathology(1). HF is a syndrome defined as the final common track to the majority of cardiac diseases, and one of the most important clinical challenges in healthcare today(2).
Nurses who take care of patients with HF experience difficulty in terms of the interpretation of signals and symptoms that present themselves as a consequence of the pathophysiological process, and have to deal constantly with other aspects inherent in human beings, who lose their equilibrium when facing the disease and its treatment.
The evaluation of the hospitalized HF patient includes verifying which aspects of his therapeutic regime have been affected. Each individual needs to breath, eat, defecate, sleep, move, have a sense of well-being, be able to take care of himself, and express feelings. These are basic human needs with regard to which nursing staff aims to assist when a disease and/or treatment interferes with the roles that a person plays in his daily life(3).
Today, there is a standard in terms of these human responses, referred to as nursing diagnoses. These standards are being used in Brazil in order to assist nursing practice in health public and private institutions, with scientific and legal support, and with an effective impact in the quality of nursing care(4,5).
Nursing diagnosis is defined as the clinical analysis of the answers given by the individual, his relatives or by the community, regarding vital processes, or actual or potential health issues. These support the process of the selection of nursing interventions on the part of the nurse, so that particular goals can be achieved, as this professional is responsible for such results(4).
There are research publications that identify diagnoses in many areas of nursing, permitting the researcher to accumulate results that, once identified, can support the decision about the clinical focus in different areas. Within this context, this study aims to identify the information produced and published in the Brazilian and international literature about nursing diagnoses in the case of HF hospitalized patients.
METHOD
This is an integrative review performed using several online databanks: CINAHL, MEDLINE, SCOPUS, LILACS, Web of Science, CAPES Thesis Bank, USP Thesis Bank and BIREME.
To guide this study, the following guiding question was used: What nursing diagnoses identified in the case of hospitalized HF patients are seen in the literature?
As an initial descriptor, the expression “nursing diagnosis”, combined with “heart failure”, in both Portuguese and English were adopted. Due to the specific characteristics of each database, the search strategies were adapted according to the aim and the inclusion criteria used in this study.
The definition of controlled descriptors was referenced on the Descriptors in Health Sciences (DeCS, in Portuguese), MESH (Medical Subject Headings) terminologies and CINAHL headings. Hence, for the databases LILACS, BIREME, CAPES Thesis Bank, USP Thesis Bank, SCOPUS and Web of Science (on the last two, there was the use of descriptors in English only), the other following controlled descriptors were used: nursing diagnoses (in Portuguese only; in both Portuguese and English; in English only) and heart failure (in both Portuguese and English). For the MEDLINE database, the following MESH terminologies were used:heart failure, congestive heart failure, chronic heart failure, acute heart failure, diastolic heart failure, systolic heart failure, heart failure preserved systolic function, heart failure with normal ejection fraction, nursing diagnosis, nursing diagnoses, nursing process. The search on the CINAHL database had the following controlled descriptors: heart failure, congestive heart failure, nursing diagnosis. The logic operators “and” and “or” were used according to the need for such.
The search in the databases took place in March 2014, organized by the following inclusion criteria: productions (article, dissertation and/or thesis) that dealt with the topic “nursing diagnoses” in adult patients (at least 18 years or older), hospitalized, with diagnosed HF, indexed in databases published in English, Portuguese or Spanish, and without a time restriction in terms of publication. Studies excluded when they did not have a clear methodology and/or were impossible to be accessed in printed or online formats.
An instrument of data collection previously validated was used in terms of the selected publications. It considers the following items: identification, methodological characteristics, methodological precision, precision over the measured interventions and over the results found(6).
All the titles and abstracts listed as a result of the search of the databases were read by two reviewers, who adopted a consensus in terms of selecting the productions that presented results that matched the question of this study, for a full, detailed reading. After the complete understanding of the texts, the items that needed to be evaluated were extracted. The data was typed into an electronic spreadsheet, of the Microsoft Excel 2007 type, for a deeper statistical descriptive analysis. After that, the information was summarized in tables to simplify the data gathered from the journals, such as number of publications per journal, their CAPES Qualis rank, levels of evidence, and description of the methodological aspects and of the nursing diagnoses.
The classification of journals using the CAPES ranking was done based on categories of evaluation, and involves an updated annual process. These evaluations are ranked based on qualitative indicators, such as - A1 (the highest level); A2; B1; B2; B3; B4; B5; C (equivalent to zero)(7).
The Practice Based on Evidences supports the idea that a qualification system of evidence that is characterized hierarchically, depending on the methodological approach used, which is supported by the study’s delimitations(8). Level 1 would be applied to evidence resulting from a meta-analysis of multiple controlled and random clinical trials; level 2 is for evidence acquired in individual studies involving an experimental design; level 3 relates to evidence from quasi-experimental studies; level 4 works for evidence from descriptive studies (non-experimental ones) or with a qualitative approach; level 5 is for evidence generated from case studies or experience studies, and level 6 is for evidence based on the opinions of specialists, according to the categorization established by the Agency for Healthcare Research and Quality (AHRQ)(8).
RESULTS
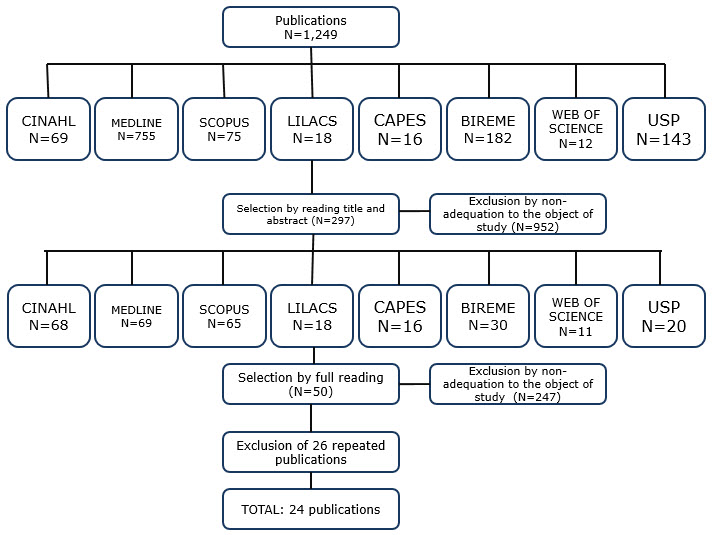
The sample was composed of 24 studies. Image 1 depicts a flowchart of the procedure to select the publications.
Image 1. Explanatory flowchart of the procedure with regard to the selection of articles. Niterói (2014).
Source: Designed by the authors.
The evaluation of the 24 articles analyzed their origin. 12 came from international journals, while 12 were Brazilian. Most of the international articles were written in English (n=10), and two were written in Spanish. The publications produced in Brazil came from the state of São Paulo (n=6), Rio de Janeiro (n=3) and Rio Grande do Sul (n=4). With regard to the type of publication, 18 were scientific articles, four were Master’s dissertations, and there were two summaries published in journals.
The following table presents the identification characteristics of the publications according to their year of publication, the journal involved, and the CAPES Qualis rank:
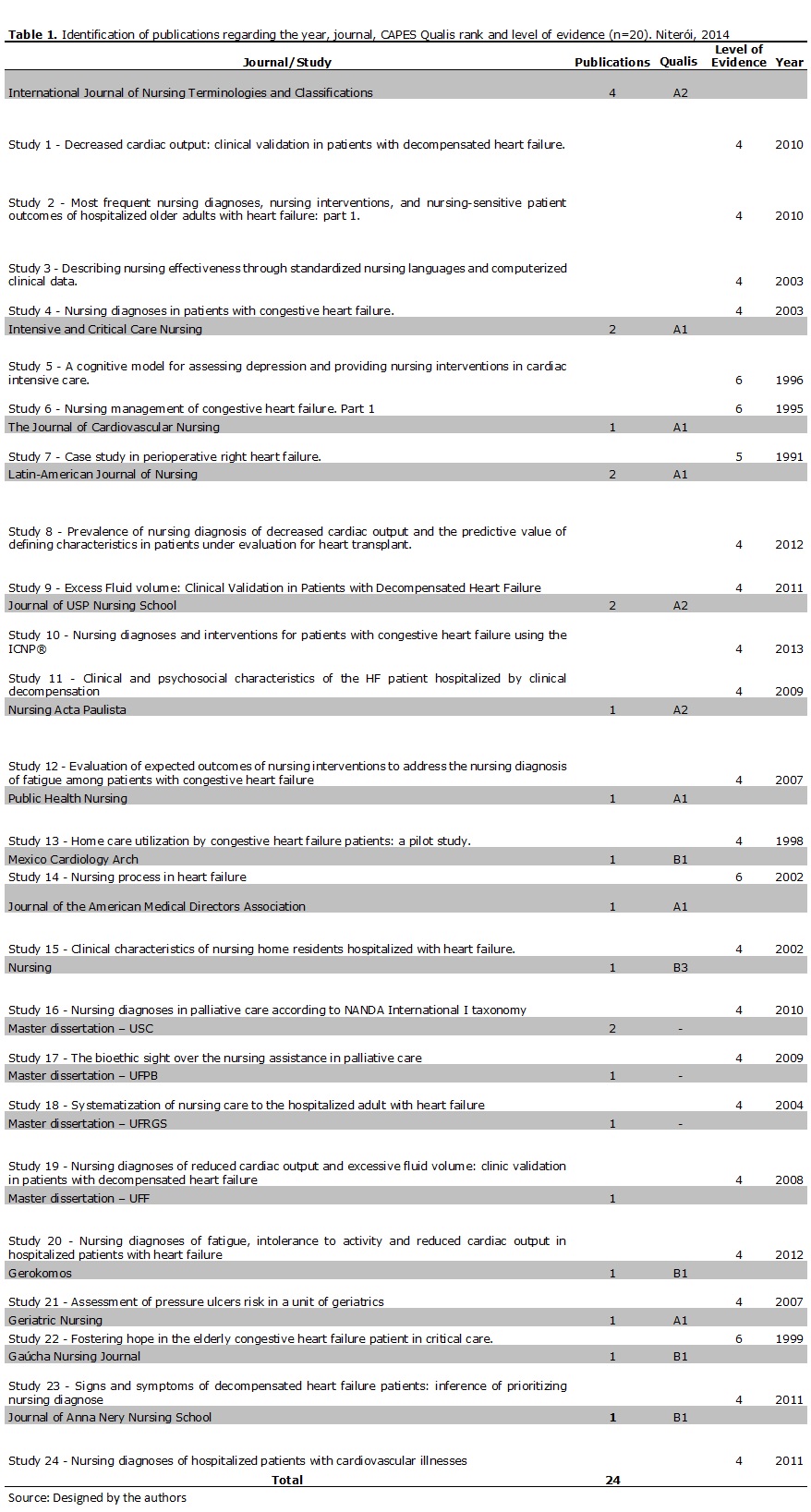
The majority of the studies were published between 2000 and 2013 (n=19). Fourteen articles came from journals that were ranked by CAPES Qualis as “A”, which is considered the best possible ranking of a journal in the area of nursing. From the 24 studies, 17 came from nursing journals and three were from medical publications, which CAPES Qualis evaluated according to their specialty. For the sample in this review, 19 studies were given a level of evidence ranking of #4, four were #6 and one was given a level of evidence of #5.
For the Master’s dissertations, the grade established by CAPES for the graduation programs was considered as an evaluation criteria(7). Study 17 came from the Graduation Program in Bioethics of São Camilo University, which has a CAPES evaluation grade of four, while for studies 18 and 20 they were produced by students of the Graduation Program in Nursing of the Federal University of Paraíba, and by the Graduation Program in Cardio-Vascular Sciences of Fluminense Federal University, respectively. The Graduation Program in Nursing of the Federal University of Rio Grande do Sul, where this study is from, was graded five by CAPES.
With regard to the object of the research, 21 of the articles studied the identification of nursing diagnoses, while three studies clinically validated the diagnoses ”decreased cardiac output” and “excessive fluid volume”. The main aspects of each study are as follows:
Study 1 clinically validated the defining characteristics of the nursing diagnosis “decreased cardiac output” from NANDA-International. The most important characteristics were fatigue, dyspnea, edema, orthopnea, nocturne paroxysmal dyspnea and elevated central venous pressure.
Study 2 identified the most frequent nursing diagnoses in the electronic medical records of 302 elderly patients hospitalized with heart failure: “intolerance to activity”, “decreased cardiac output”, “lack of knowledge” and “risk of falling”.
Study 3 offered a survey of nursing interventions based on NANDA-I, NIC and NOC in the electronic records of 566 patients hospitalized with HF and pneumonia. Most frequent were “deficient understanding”, “ineffective airway clearance”, “decreased cardiac output” and “pain”.
Study 4 identified the prevalence of nursing diagnoses in 26 patients. “Intolerance to activity” was present in 100% of patients, followed by “excessive fluid volume” (92%).
Study 5 was the reported case of a patient with HF and the nursing diagnosis of “depression”. In this paper, there was the discussion of intervention proposals according to the defining characteristics explored in the article.
Study 6 was a piece of bibliographical research that brought nursing interventions and results directed to the following diagnoses that were considered to be of the highest priority: “decreased cardiac output”, “impaired tissue perfusion”, “impaired gas exchange”, “excessive fluid volume”, “ineffective breathing pattern”, “intolerance to activity”, “despair” and “deficient knowledge”.
Study 7 was a case study of a patient with HF in a perioperative period, during which time nursing diagnoses were “decreased cardiac output”, “impaired gas exchange” and “high risk of inefficient family coping”.
Study 8 identified the prevalence of the defining characteristics of the nursing diagnosis “decreased cardiac output” in patients with HF who were under evaluation for a heart transplant. The characteristics of increased peripheral vascular resistance, third heart sound, and decreased ejection fraction were considered predictive for the studied diagnosis.
Study 9 clinically validated the diagnosis “excessive fluid volume”. The defining characteristics considered important were dyspnea, orthopnea, edema, hepatojugular positive reflection, nocturne paroxysmal dyspnea, lung congestion and elevated central venous pressure.
Study 10 considered affirmatives of nursing diagnoses and interventions for patients with congestive HF based on the International Classification of Nursing Practice (ICNP®). These resulted in 66 affirmatives with regard to nursing diagnoses, divided according to the following dimensions: tachycardia, dyspnea, edema and congestion.
Study 11 evaluated the clinical and psychosocial characteristics of 61 patients with decompensated HF, particularly: dyspnea, coughing, chest pain, fatigue, dizziness, palpitation, headache and edema.
Study 12 identified the main defining characteristics in 30 patients, with a nursing diagnosis of “fatigue” relatd to need for additional energy, inability to keep up with the routine, verbalization of lack of energy, increase in the number of physical complaints.
Study 13 identified the nursing diagnoses of 40 elderly patients with chronic HF. These were: “intolerance to activity”, “decreased cardiac output”, deficient knowledge”, “risk of falling” and “impaired skin integrity”.
Study 14 was a bibliographical piece of research that considered the process of nursing based on priority nursing diagnoses such as: “decreased cardiac output”, “impaired gas exchanges”, “excessive fluid volume”, “intolerance to activity” and “deterioration of quality of life”.
Study 15 identified the clinical characteristics of 95 patients with HF in homecare: dyspnea at rest and during exercises, orthopnea, nocturnal paroxysmal dyspnea, fatigue and edema of the lower limbs.
Study 16 identified the nursing diagnoses of 20 medical records of patients with HF under palliative care, such as: “impaired physical mobility”, “altered risk of nutrition” and “impaired skin integrity”.
Study 17 performed a nursing process in 20 elderly hospitalized patients under palliative care, and presented “risk of falling”, “impaired physical mobility”, “risk of altered nutrition”, “impaired skin integrity”, “chronic pain”, “inefficient breathing standard”, “risk of infection” and “decreased cardiac output”.
Study 18 performed the systematization of nursing care in hospitalized adults with HF in the light of the Horta’s Theory of Basic Human Needs. The main diagnoses found in this paper were: “reduced cardiac output”, “disturbed sleep standard”, “constipation”, “ineffective airway clearance”, “intolerance to activity”, “acute pain”, “anxiety”, “impaired skin integrity”, “impaired physical mobility”, “hyperthermia” and “diarrhea”.
Study 19 was a Master’s dissertation that clinically validated the nursing diagnoses “decreased cardiac output” and “excessive fluid volume” in patients with decompensated HF, and originated the publications of studies 1 and 9.
Study 20 evaluated the nursing diagnoses “fatigue”, “intolerance to activity” and “reduced cardiac output” in patients hospitalized with decompensated HF which this one was considered the most significant, associated with patients with acute myocardial infarction, functional class III (NYHA), and altered values of plasma creatinine clearance.
Study 21 analyzed the risk of developing pressure ulcers in a geriatric hospitalization unit, where HF was one of the main causes of hospitalization. The nursing diagnoses found were: “reduction of physical activity”, “deficit in self-care”, “impaired skin integrity” and “intolerance to activity”.
Study 22 considered the implementation of the process of nursing in a hospitalized patient with HF, and with the nursing diagnosis “depression”. The main defining characteristics were loss of weight, loss of appetite, reduced anxiety, reduced verbalization, lack of initiative, reduced response to stimuli, reduced affection, passivity and lack of commitment to the treatment.
Study 23 identified the signs and symptoms of 303 hospitalized patients with decompensated HF admitted in an emergency unit, and prioritized the nursing diagnoses implied.
Study 24 verified the nursing diagnoses in the case of hospitalized patients with cardiovascular diseases, HF being the most frequent reason for such hospitalization. The most prevailing diagnoses were “anxiety”, “acute pain” and “reduced cardiac output”.
Table 2 presents the most significant methodological aspects of the studies analyzed:
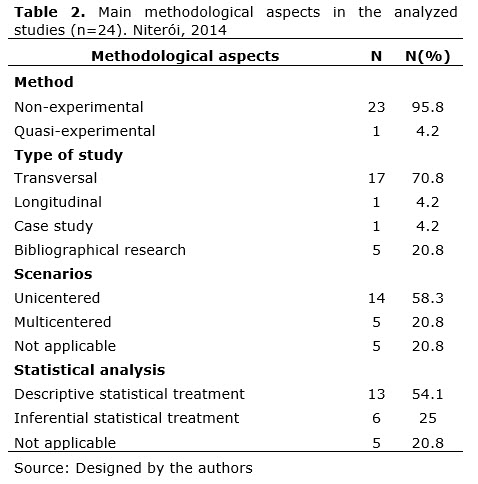
These studies are mostly methodologically non-experimental, prospective transversal, single-centered and with a descriptive statistical analysis.
It is important to mention that the studies involving inferential analysis attempted to create connections between the presence of a certain nursing diagnosis and the clinical and socio-demographic characteristics in a sample of HF patients. In order to do so, the statistics were performed as follows: chi-square test calculations (or Fisher’s exact test), the T-Student test (or Mann Whitney’s Test), the Kruskal-Wallis test and analysis of simple variations (studies 3, 13, 20 and 24). When the objective was to verify the predictive value of defining characteristics for a certain diagnosis, the calculation of odds ratio was used (studies 8 and 15).
Throughout these studies, 35 titles for nursing diagnoses were mentioned in the case of hospitalized HF patients. Table 3 presents the most frequently mentioned nursing diagnoses per study.
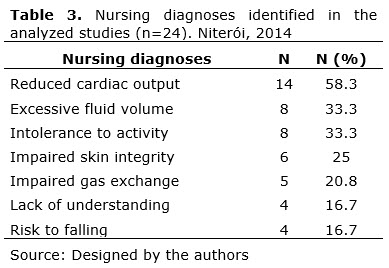
There were 8 types of nursing diagnoses identified among the 24 studies. From these, 14 mentioned “reduced cardiac output”, “excessive fluid volume” (n=8) and “intolerance to activity”, “impaired skin integrity” (n=6), “impaired gas exchange” (n=5) and four studies cited “deficient knowledge”, “risk of falling” and “impaired physical mobility”. It is important to say that, from the 24 publications, 13 used the diagnosis standard NANDA-I, 10 studies worked with a free diagnosis pattern, and one used ICNP®.
DISCUSSION
The information produced and published was observed from around the world, with a significant Brazilian representation. It is significant to add the fact that two of the pieces of research found in international journals were produced in Brazil, which demonstrates that the country is actively participating in the search for a greater level of understanding in this area. Studies published mainly in journals ranked “A” in the area of nursing may indicate a concern for improving the intellectual qualifications of the researchers.
In this review, 53% of the studies presented evidence at level four according to the method of evaluation used by the Agency for Healthcare Research and Quality (AHRQ)(8). Therefore, besides this methodology involving evaluation of the level of evidence, there is also a proposal done by the Joanna Briggs Institute, which analyzes the publications using their own instrument, based on qualitative and quantitative approaches, the synthesis of the opinions of specialists, budgetary analysis, consideration of technology and review of instruments as a means of observing the levels of evidence which categorize these studies. In terms of the reviews of important authorities, based on clinical and experience criteria, in descriptive studies and in reports written by committees of specialists, the level of evidence found is IV(9).
With regard to the most frequently mentioned nursing diagnoses, “reduced cardiac output” was highlighted. This is defined by NANDA-I as an insufficient amount of blood sent out from the heart to support the body’s metabolic demands(4). This diagnosis shows aspects of the decompensating HF and its follow-up throughout the process of hospitalization, permitting the monitoring of care offered to the patient during the course of his illness.
The “excessive fluid volume” in HF is caused by the excessive ingestion of fluids and of sodium, almost always resulting from an inadequate diet, which leads to an overcharge of the renal functions and hydric retention(1,10-11).
The “intolerance to activity” in HF is related to breathing discomfort, fatigue and palpitations, which the patients experience when developing their own daily routines, limiting the quality of life and causing early retirement and an increased indirect cost to the public national health system(1,12).
“Impaired skin integrity” means altered epidermis and/or dermis, being explained by the invasion of structures in the body of the hospitalized cardiac patient that needs a more invasive approach on the part of the health team, in order to monitor the hydric balance and the hemodynamic values, and to guarantee nutritional and effectiveness support for the pharmacologic treatment, with the use of urinary catheters, nasogastric tubes and peripheral venous access, respectively(4).
“Impaired gas exchange” is related to the secondary hypoxemia to the ventilation-perfusion imbalance and lung edema. A transversal study that evaluated indicators of gas exchange in hospitalized HF patients indicated the following characteristics: breathing depth and frequency, orthopnea, chest pain, sleepiness and urea(13).
The “lack of understanding” can affect adherence to the treatment, which is one of the main causes of HF decompensation. With regard to this, the non-pharmacological approach uses strategies of education, monitoring, changes in life style and palliative care(1-2).
The “risk of falling” was the only diagnosis of risk evidenced in this review. This is associated with the symptoms of HF, such as dizziness, tiredness, dyspnea, all of which are significantly important that the nurse identifies the need for protective measures with regard to the hospitalized patient.
CONCLUSION
The contribution of this study implies the need for the prioritizing of nursing interventions in terms of the hospitalized HF patient, thereby avoiding and/or reducing mistakes in the development of nursing processes, and proposes the construction of assisting protocols based on the evidence here presented.
REFERENCES
1. Bocchi EA, Marcondes-Braga FG, Bacal F, Ferraz AS, Albuquerque D, Rodrigues D, et al. Sociedade Brasileira de Cardiologia. Atualização da Diretriz Brasileira de Insuficiência Cardíaca Crônica - 2012. Arq Bras Cardiol 2012: 98(1 supl. 1): 1-33.
2. Bertuzzi D, Souza EN, Moraes MA, Mussi C, Rabelo ER. The knowledge of patients with heart failure in the homecare context: an experimental study. Online braz j nurs [ periodic online ]. 2012 Dec [ cited 2014 03 march ] 11 (3): 572-82. Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/3736.
3. Thoroddsen A, Ehnfors M, Nurs D, Nurs A. Nursing Specialty Knowledge as Expressed by Standardized Nursing Languages. International Journal of Nursing Terminologies and Classifications. 2010 April; 21(Issue 2): 69-79.
4. Herdman TH. NANDA International Nursing Diagnoses: Definitions & Classification 2012-2014: Wiley-Blackwell Ames, IA; 2012
5. Bittencourt GKGD, Crossetti MGO. Theoretical model of critical thinking in diagnostic processes in nursing. Online braz j nurs [ periodic online ].2012 Oct [ cited 2014 03 march Suppl 1: 563-7.Available from:http://www.objnursing.uff.br/index.php/nursing/article/view/3919
6. Ursi ES. Prevenção de lesões de pele no perioperatório: revisão integrativa da literatura. [ dissertação ]. Ribeirão Preto: Universidade de São Paulo, Escola de Enfermagem de Ribeirão Preto; 2005.
7. Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. Qualis periódicos. 2014. Disponível em: http://www.capes.gov.br/avaliacao/qualis.
8. Stetler CB, Morsi D, Rucki S, Broughton S, Corrigan B, Fitzgerald J, et al. Utilization-focused integrative reviews in a nursing service. Appl Nurs Res. 1998; 11(4):195-206.
9. The Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual: 2014 edition [ Internet ]. South Australia (Australia): The University of Adelaide; 2014[ citado em 2014 Mar 1 ]. Disponível em: http://www.joannabriggs.org
10. Jessup M, Abraham W, Casey D, Feldman A, Francis G, Ganiats T, et al. 2009 Focused Update: ACCF/AHA Guidelines for the Practice Guideline: Focused Update Diagnosis and Management of Heart Failure in Adults. Circulation, 2009; 119:1977–2016.
11. Brandão SMG, Altino DM, Silva RCG, Lopes JL. Defining Characteristics of Decreased Cardiac Output: A Literature Review. International Journal of Nursing Terminologies and Classifications. 2011 April/June; 22(Issue 2): 92-102.
12. Zipes DP, Libby P, Bonow RO. Braunwald E. Braunwald Tratado de Doenças Cardiovasculares; 2009.p.539-68.
13. Sousa VEC, Montoril MH, Pascoal LM, Lopes MVO. Avaliação da troca gasosa de pacientes com insuficiência cardíaca congestiva. Cogitare Enfermagem. 2010 Outubro/Dezembro; 15(4):681-7.
14. Amorim LC, Santos I, Rocha RM, Rangel B, Albuquerque DC. Quality of life of patients with heart failure: a quantitative study. Online Brazilian Journal of Nursing[ serial on the Internet ]. 2009 [ cited 2013 march 10 ] 8(3): [s.p.]. Available from http://www.objnursing.uff.br/index.php/nursing/article/view/j.1676-285.2009.2518/554.
15. Martins QCS, Aliti G, Rabelo ER. Decreased cardiac output: clinical validation in patients with decompensated heart failure. International Journal of Nursing Terminologies and Classifications. 2010;21(4):156-65 [ incluída na revisão ].
16. Scherb CA, Head BJ, Maas ML, Swanson EA, Moorhead S, Reed D, et al. Most Frequent Nursing Diagnoses, Nursing Interventions, and Nursing‐Sensitive Patient Outcomes of Hospitalized Older Adults With Heart Failure: Part 1. International journal of nursing terminologies and classifications. 2011;22(1):13-22 [ included in the review ].
17. Scherb CA. Describing nursing effectiveness through standardized nursing languages and computerized clinical data. International Journal of Nursing Terminologies and Classifications. 2003;14(4):29-30 [ included in the review ].
18. Calsinski de Assis C, de Barros L, Botura A. Nursing diagnoses in patients with congestive heart failure. International Journal of Nursing Terminologies and Classifications. 2003;14(s4):1-2 [ included in the review ].
19. Johnson LH, Roberts SL. A cognitive model for assessing depression and providing nursing interventions in cardiac intensive care. Intensive and Critical Care Nursing. 1996;12(3):138-46 [ included in the review ].
20. Dahlen R, Roberts SL. Nursing management of congestive heart failure. Part 1. Intensive and Critical Care Nursing. 1995;11(5):272-9 [ included in the review ].
21. Wingate S, Leach SP, Mitchell SM, Dudas GM. Case study in perioperative right heart failure. The Journal of cardiovascular nursing. 1991;6(1):80-6 [ included in the review ].
22. Matos LN, Guimarães TCF, Brandão MAG, Santoro DC. Prevalence of nursing diagnosis of decreased cardiac output and the predictive value of defining characteristics in patients under evaluation for heart transplant. Revista latino-americana de enfermagem. 2012;20(2):307-15 [ included in the review ].
23. Martins QCS, Aliti GB, Linhares JC, Rabelo ER. Excess fluid volume: clinical validation in patients with decompensated heart failure. Revista Latino-Americana de Enfermagem. 2011;19(3):540-7 [ included in the review ].
24. Araújo AAd, Nóbrega MMLd, Garcia TR. Nursing diagnoses and interventions for patients with congestive heart failure using the ICNP®. Revista da Escola de Enfermagem da USP. 2013;47(2):385-92 [ included in the review ].
25. Del Paciente CCYP, Insuficiencia CON. Características clínicas e psicossociais do paciente com insuficiência cardíaca que interna por descompensação clínica. Rev Esc Enferm USP. 2009;43(1):44-53 [ included in the review ].
26. Assis CCd, Barros ALBLd, Ganzarolli MZ. Evaluation of expected outcomes of nursing interventions to address the nursing diagnosis of fatigue among patients with congestive heart failure. Acta Paulista de Enfermagem. 2007;20(3):357-61 [ included in the review ].
27. Anderson MA, Pena RA, Helms LB. Home care utilization by congestive heart failure patients: a pilot study. Public Health Nursing. 1998;15(2):146-62 [ included in the review ].
28. Ortega VC, Cortés GP. Nursing process in heart failure. Arch Cardiol Mex. 2002;72(Suppl1):S262-6 [ included in the review ].
29. Ahmed A. Clinical characteristics of nursing home residents hospitalized with heart failure. Journal of the American Medical Directors Association. 2002;3(5):310-3 [ included in the review ].
30. Mendes AF, Guerra GM, Tsunem M, Palomo JdSH. Diagnósticos de enfermagem em cuidados paliativos segundo a taxonomia NANDA Internacional l. Nursing (São Paulo). 2010;13(148):463-73 [ incluída na revisão ].
31. Mendes AF. O olhar bioético na atenção a assistência de enfermagem em cuidados paliativos [ dissertação ]. São Paulo: Universidade São Camilo, Mestrado em Bioética, 2009;100 [ incluída na revisão ].
32. Negreiros RVd. Sistematização da assistência de enfermagem ao adulto hospitalizado com insuficiência cardíaca [ dissertação ].Paraíba: Universidade Federal da Paraíba. Centro de Ciências da Saúde, 2005;110 [ incluída na revisão ].
33. Barth QCM. Diagnósticos de enfermagem de débito cardíaco diminuído e volume excessivo de líquidos: validação clínica em pacientes com insuficiência cardíaca descompensada [ dissertação ]. Porto Alegre: Unversidade Federal do Rio Grande do Sul.Escola de Enfermagem. Programa de Pós-Graduação em Enfermagem, 2008;109 [ incluída na revisão ].
34. Lago González ML.Assessment of pressure ulcers risk in a unit of geriatrics. Gerokomos. 2007;18(3):135-9 [ included in the review ].
35. Pereira JdMV. Diagnósticos de enfermagem fadiga, intolerância à atividade e débito cardíaco diminuído em pacientes com insuficiência cardíaca hospitalizados [ dissertação ]. Rio de Janeiro: Universidade Federal Fluminense, Programa de Pós-graduação em Ciências Cardiovasculares, Departamento de Medicina Clínica, 2012;121 [ incluída na revisão ].
36. Roberts SL, Johnson LH, Keely B. Fostering hope in the elderly congestive heart failure patient in critical care. Geriatric Nursing. 1999;20(4):195-9 [ included in the review ].
37. Aliti GB, Linhares JCC, Linch GFdC, Ruschel KB, Rabelo ER. Sinais e sintomas de pacientes com insuficiência cardíaca descompensada: inferência dos diagnósticos de enfermagem prioritários. Revista Gaúcha de Enfermagem. 2011;32(3):590 [ incluída na revisão ].
38. Pereira JdMV, Cavalcanti ACD, Santana RF, Cassiano KM, Queluci GC, Guimarães TCF. Diagnósticos de enfermagem de pacientes hospitalizados com doenças cardiovasculares. Escola Anna Nery Revista de Enfermagem. 2011;15(4):737-45 [ incluída na revisão ].
Ana Carla Dantas Cavalcanti – participated in designing the research, collecting data, reviewing, writing and making the final corrections.
Juliana de Melo Vellozo Pereira - participated in designing the research, collecting data, reviewing, writing and making the final corrections.
Recibido: 25/05/2012
Revisado: 14/03/2014
Aprobado: 23/03/2014