ARTIGO ORIGINAL
The need to become family caregivers: Grounded Theory
Raquel Silva de Paiva1; Glaucia Valente Valadares1; Juliana Silva Pontes1
1Federal University of Rio de Janeiro
ABSTRACT
Aim: To discuss the relationship between the family and hospital discharge regarding manifestations, attitudes, feelings and practices. Method: The Theory Based on Data Approach, with semi-structured interviews and unsystematic participant observation was used as an approach. The research was undertaken in a public hospital in the city of Rio de Janeiro. Nine family members who are caregivers for a relative subsequent to a stroke, participated. Results: The categories "Facing the unexpected," "Recognizing the need for care after discharge" and "Realizing one’s importance in the recovery of the relative" emerged. Discussion: The data showed an understanding on the part of the family with regard to the need to care for relative affected by stroke, highlighting the duality evident in this experience. Conclusion: The impact caused by the stroke and the need to take care of the relative at home highlights the importance of subjectivity and exchange of knowledge, being necessary to comply with the expectations and meanings of each family caregiver.
Keywords: Family Nursing; Patient Discharge; Stroke; Nursing Care.
INTRODUCTION
Cerebrovascular diseases, especially stroke (AVC), are the second leading cause of death worldwide, and the leading cause of disability among adults. Five million people die each year due to cardiovascular events and, of the individuals who survive such an event, 33% to 50% remain with severe sequelae, and rehabilitation can last for months or years. Of these survivors, 10% are at risk of developing a recurrent stroke during the first year after the event(1).
Considering the increased incidence of risk factors in the lives of the population at the beginning of the XXI century, cardiovascular diseases account for 32.2% of deaths in Brazil, and stroke is the leading type cardiovascular disease(2). The incidence of stroke is higher after the age of 65 and, considering the fast aging population, it is estimated that this event is, increasingly, an important public health problem.
Because it is a disease which has an acute onset and a chronic course, stroke has intermediate consequences which require adjustment on the part of the client, the family and the health professional services that serve this clientele. Thus, it is important that everyone is protected in these times of crisis, doubts and uncertainties. It is necessary that we think about the needs and desires of clients and families in order to prepare them for home care.
Considering the functional and cognitive deficits, as well as the personality change and the behavior and communication difficulties presented by the stroke victim, the degrees of disability tend to undermine family and society, determine the levels of dependence on assistance and, consequently, make it a challenge to care.
The individuals affected by the stroke usually follow an intervention and treatment routine ranging from surgery to clinical treatment and, finally, to rehabilitation.
Thus, it is important that from the first day of hospitalization, client and family have access to information that will contribute to the development of their skills and capabilities in the post-discharge period. This requires that the nursing professional promotes education and health throughout the period of hospitalization, based on the certainty that the family is an important source of support and welfare for the sick client.
Preparation of the client and the family for discharge throughout the period of hospitalization reduces expectations in terms of home care. On this subject, the professional nurse is responsible for establishing the link with other professionals, in order to provide the welfare and resources necessary for ensuring the safety of care after discharge.
Hospital discharge should be planned based on the reality and the needs of each individual, using the discharge plan (PAH), which consists, in an organized way, of the activities determined by the specific condition of each client(3).
However, the discharge policy, increasingly adopted at an early stage by hospitals, poses a constant challenge to nurses who need to prepare clients and families in the reorganization of life in their homes, over a short period of time as a means of identifying potential problems, and preventing and controlling situations that may occur(4).
Regarding teaching and learning, the client should, with professional help, constantly evaluate the client’s progress. If the person has additional attacks that might limit his/her activities, a very common occurrence in clients suffering a stroke, the family should be counseled about these limitations. It will be necessary for the nursing professional to observe the evolution of the family throughout the time in hospital in order to be able to continue providing assistance at home.
When thinking about home treatment, there is the need to understand what value the family can offer with regard to this new experience - caring for a relative and considering all possible difficulties that may arise. It is worth remembering that a lack of preparedness can cause serious harm to the client, resulting, even, in recurrent hospitalizations.
It is necessary to realize that a chronic disease tends to completely change the daily lives of families. Become a family caregiver may be stressful, which may be reflected in the loss of physical and mental health on the part of the caregiver alongside the process of the rehabilitation of the dependent relative. Given this, it is imperative that nursing staff understand how the family defines the situation of caring for the subject affected by a stroke.
Thus, the study is justified, mainly, by the social relevance of considering the peculiarities and complexities of the phenomenon under consideration. The increase in population over the age of 65 in Brazil, the increased incidence of cerebrovascular diseases in this age group, the premature discharge policy adopted by healthcare institutions among other factors, are issues that require urgent action to better prepare clients and those of his/her family that will be responsible for home care.
Considering the significance of hospital discharge to the stroke client's family as an object of study and the concerns originating from the reflections above, the research aims to discuss the relationship between the family and the hospital discharge process regarding the manifestations, attitudes, feelings and practices of those affected.
Taking care for an ill family member is a complex and unique job in the life of every person so affected. Realizing that this singularity generates distinct ways to understand and take care, for the purpose of undertaking this study, Symbolic Interactionism (IS)(5) was adopted as a theoretical approach. This was because it facilitates an understanding of the phenomenon, and allows the researcher to appreciate the significance that human beings attribute to their experiences.
Human being plans and direct their actions with regard to others in terms of granting of meaning to the objects it uses to run it plans(5). We live in a symbolic world where individual constructs, symbols and meanings are designated with values we acquire throughout life. The experience of having a relative affected by a stroke and the reality of taking care of such a person are experiences that are supported by our perceptions of the world. Thus, actions are directed according to the meaning that the situation has for each stakeholder (individual, family and institution).
METHOD
Symbolic Interactionism is the best choice in terms of qualitative methodological approaches in that it enables the production of knowledge based on practical reality. Therefore, we opted for a qualitative approach, and the Theory Based on Data (TFD) approach as a method(6). This allows us to understand, through systematic analysis, the processes by which the phenomena are unfolding.
The Theory Based on Data approach is characterized by being a field method whose purpose is to generate theoretical constructs that explain socially contextualized action. Thus, the theory originated from the adoption of elements of TFD and is derived from data gathered, analyzed and compared through a complex process of analysis and interpretation(6).
Considering that the associations between categories can be subtle and implicit, and with the intention of deepening theory, experts consider it useful to adopt a paradigmatic model. This is an organizational scheme used to classify and organize theoretical connections, incorporating the following basic components: causal conditions, context, intervening conditions, action-interaction strategies, and consequences(6).
In this research we will consider the discussion of the causal conditions associated with the phenomena, i.e., events or incidents that lead to the occurrence or development of a phenomenon.
With regard to data collection, the procedures followed the precepts of Resolution No. 196/96 of the Ministry of Health, which addresses research involving humans. Therefore, we requested permission from the Ethics Committee in Research of the Municipal Health and Civil Defense of the Municipality of Rio de Janeiro, which approved the study in accordance with Opinion No. 90A/2011.
The data collection occurred through semi-structured interviews and unsystematic participant observation. Individual interviews were conducted according to the availability of family members. Thus, there were days and times scheduled after the hospital visit, in a reserved place outside the ward, allowing respondents to express their perceptions.
The participant observation was done during the hospital visit because this is an opportune time to observe the relationship of the healthcare team with the relatives, and the relatives with the hospitalized patient. The observation lasted two days before and after the semi-structured interviews, with the purpose of complementing the data obtained and to verify the need for new questions after observation.
The participants were the relatives of the hospitalized patients, who in turn were victims of a first stroke event with moderate or severe disability in a neurological health institution. The choice of these patients was based on families experiencing this situation for the first time.
Relatives over eighteen years of age, of both genders, who identified themselves as family caregivers who were to assume primary responsibility and provide unpaid care for a relative with stroke sequelae after hospital discharge, participated in the study. Patients receiving psychiatric treatment or exhibiting other neurological disorders that, in addition to care facing the consequences of stroke, needed other forms of care, were excluded from the study. Data collection was conducted between the months of May and July 2011.
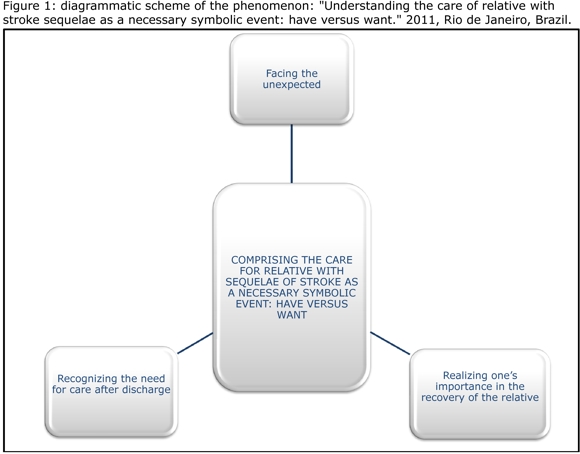
To better understand the data, see Figure 1. The aim is to allow the reader to visualize and better understand the phenomenon and its relationship to the categories and subcategories that compose it.
RESULTS
Following the precepts of TFD, it was adopted as the theoretical sampling procedure for obtaining data. This is an ongoing feature whereby data begin to repeat themselves until they reach a situation of theoretical saturation, i.e., when the data collection procedure no longer results in new information(6).
In this sense, the study sample was composed of nine willing family caregivers. It is worth mentioning that the number of families interviewed was configured based on the analysis of interviews and observations. The production of data indicated the need for new collections in order to clearly delineate the categories(6).
The profile of interviewees included six females and three males. In order to ensure the anonymity of the participants the letter "E" was used, and a numeral corresponds to each speech as identified in the study - [ E1 ], [ E2 ], and so on.
With regard to the relationship to the hospitalized individual, six were sons/daughters, two were spouses and one was a sister, with ages ranging from 29 to 61 years. Regarding the length of hospitalization, this ranged between one month and five months. It should be noted that data collection took place near the time of hospital discharge.
During the review process related to causal conditions, there emerged the phenomenon "Comprising the care for relatives with sequelae of stroke as a necessary symbolic event: have versus want," anchored by categories: "Facing the unexpected", "Recognizing the need for care after discharge" and "Realizing one`s importance in the recovery of the relative.”
Facing the unexpected – This highlights the unexpected character of the event. In the reports you can see that even when the individual presented some risk factors, the family did not think of the possibility of a stroke.
You never think it will happen. She took care of her health, taking medicines for hypertension and being treated for diabetes. However, she just could not stop smoking.[ E3 ]
Given the unpredictability of such a situation, the families found that receiving the news of the stroke was scary.
On the day that I knew that he had an AVC, I was in shock. I did not know what to think or what to do. I was wondering about his life and ours too. I knew that a lot would change. [ E5 ]
Upon receiving the news, the person thought that s/he had all the knowledge needed about the disease (symbols rescue). They thought about the seriousness of the situation (related to the symbols) and had bad or negative thoughts. The following individual demonstrated in his comments, a concern about the presence of the current sequelae.
Receiving the news was very bad. Many things crossed my mind. A lot of bad things. [ E2 ]
Considering that strokes are common in the Brazilian population and that their sequels are easily understood in terms of common sense, to receive the news that a relative was affected, the person tends to think of the limitations resulting from AVC. It should be noted that even before obtaining a confirmed diagnosis, they understood the gravity of the situation and, in most cases, had feelings of distress.
Recognizing the need for care after discharge - After the initial shock of the confirmation of the diagnosis, the relatives realized the wide variety of constraints and this was replaced by the notion of the magnitude of the event.
After discharge we'll continue caring for him at home, helping him to stay as it was before, or doing things in the best possible way. From what I know, we'll have to even care for these sequelae. [ E5 ]
The continuity of care after discharge is a key element in the recovery of a stroke victim, and can be quite prolonged. When the diagnosis is confirmed and is sequelae are presented, the family recognizes that, after discharge, it must dedicate itself to care in the home environment.
The doctor said that the treatment for a stroke is very long and that my husband will need to do physical therapy and other activities to recover his movements [ ... ] when he is discharged, some of the things that happen here will have to happen at home. [ E4 ]
Often, before the impact of the news and the diagnosis, the family does not accept the restrictions imposed by a cerebrovascular event. Also, it is quite a complex process for the family to fully accept the need for specific care. They may even have idealized unrealistic aims. In this situation, the nurse can work with the family in order to establish a partnership, providing information about the disease, the limits and the possibilities of recovery, helping individual caregivers to face this new life situation.
Realizing one`s importance in the recovery of the relative - when the family caregiver understands that the care provided after discharge should be based on the possibilities of a relative having sequels, its understands that their part in the recovery process is extremely important. In this sense, the nurse must consider the family as having a fundamental role to play during rehabilitation, clarifying whatever it is they need, and becoming a care agent.
Family participation in the treatment of the relatives is very important, since the client is left with physical disabilities and cognitive deficits (deficits for self-care) that complicate or prevent them from following the treatment by themselves. Furthermore, family support is fundamental to the recovery of self-esteem which helps the individual to seek recovery.
[ ... ] despite shock, now I'm relieved and I know I need to stay here to look after him well and also at home. I know it will be good for him if I'm quiet and if I’m prepared for the changes. There are the sequels he'll have to struggle with to treat, to reduce dependence or even to go back to what he was. And I'll go along with him, encouraging him, so it'll be easier for him. [ E4 ]
Realizing that the relative presents disabling sequelae by the desire to see the client restored, that person appreciates the relatives’ participation in treatment and recovery.
Her stroke was very violent, very serious. From what I see, and also with the information I have received, I imagine that the recovery will be very slow and difficult. But my father and I are working together to care and help in any way possible. [ E6 ]
In this sense, nurses need to encourage the active and responsible participation of the family in care, encouraging those involved and supporting them in the reorganization of their lives. This attitude strengthens and empowers families to meet the needs of care for their members, decreasing the distress and suffering in terms of the common situation experienced.
DISCUSSION
The advent of a stroke, due to its characteristics and consequences, constitutes a source of tension within the family. This is because it requires the redefinition of roles on the part of family members. After all, the management of the disabilities arising from the disease occur in the home context.
The sequelae generate the need for someone to assist in performing daily activities and, in most cases, it becomes the responsibility of members of the client’s family. However, the need to become a family caregiver causes great uneasiness, which is associated with pre-assigned concepts of the relative, as well as the physical and emotional exhaustion caused by the new job.
Given the unpredictability of the situation and based on their prior knowledge about the consequences and complications of a stroke, the family engages with a series of doubts and dilemmas. It is common for families to face dilemmas such as the need to choose a single caregiver, needing to think about the changes that occur in the physical environment of the home, and the routine of the family after discharge.
The lack of awareness on the part of the caregivers with regard to the disease or illness in general, the progression of the disease, possible complications, the proper way to care at home and the physical and social demands that may arise, can cause a great deal of anxiety on the part of family caregivers who initially do not think that they are qualified to care.
The actions of family caregivers are mediated by meanings. After facing the world around them, the individual is called to act, i.e., to deal with the situations with which they are faced. To achieve this, it is necessary for them to reflect, interpret and determine their actions in the light of these reflections(7).
Caring for a dependent family member is related to actions imposed by society, which in turn are based on social norms, beliefs and cultural values. We should consider that each family is unique and, in a situation of illness, organizes its own way of taking care of its members. The quality of care provided depends on how the family is prepared, organized and oriented to provide care in the home(8).
Understanding the process of care at home can allow us to identify deficiencies and weaknesses to which nurses can turn their attention. It can help them to choose priorities and focus in their work. Informal care is, and will continue to be, provided by family members in most cases, and in situations that involve chronic conditions, short, medium and long term dependence, with or without the use of technical equipment(4).
The context experienced by relatives can be translated into feelings and behaviors that are sometimes difficult to understand. Thus, the support for the family needs to be placed in the professionals’ working context, involving dialogue, listening, and hosting aspects relevant to the processes of humanization(9).
Nursing staff should reflect on the meaning of the family, as an active member in the recovery process and in the well-being of the ill patient. Staff should reserve moments during which the think about their own situation making that individual an active participant, and facilitating interpersonal relationships, preparing that person for assuming the role of family caregiver after discharge.
Thus, we must recognize that the family is part of the healing process of the relative in that they provide welfare and act as a communicator between the patient and the health team. This therapeutic relationship can be maximized when there is an interest on the part of professionals, valuing the affective relationship between family and patient(10).
CONCLUSION
The data analysis allowed us to understand that the impact of an AVC and the need to take care of the client at home highlights the importance of subjectivity and the exchange of knowledge, being necessary to comply with the expectations and meanings of each caregiver within a family.
Considering the significance of family members when it comes to taking care of a relative with the sequelae of a stroke, the process of taking care after hospital discharge should be thought of as being more than a simple task execution. It must be understood that caring for a dependent relative requires affection and commitment between those who care and the individual who is cared for.
In this sense, as presented, the path taken internally by the caregiver goes through symbolic aspects, ranging from an awareness of the disease and its peculiarities, through understanding that treatment will have to be continued in the family home, reaching an understanding of its importance in the recovery of an ill relative. That is, the individual unconsciously perceives the world around him or her, interprets and reflects on the situation, emphasizing its importance in the treatment of the victims of a stroke.
Thinking about the complexity involved in the care of someone who is ill in this way, and being aware of the limited time available to enable patients and family caregivers to perform home care, we must emphasize the fundamental importance of nursing staff having a broad perspective, encompassing the whole family in its planning and care processes.
REFERENCES
1. Organização Mundial de Saúde (OMS). Media Centre. The top 10 causes of death. Genebra: 2008. [ on-line ] [ citado em março de 2010 ] Disponível em: www.who.int/mediacentre/factsheets/fs310/en/index.html.
2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. A vigilância, o controle e a prevenção das doenças crônicas não-transmissíveis: DCNT no contexto do Sistema Único de Saúde brasileiro. Brasília: Organização Pan-Americana da Saúde; 2005
3. Huber DL, Mcclelland E. Patient preferences and discharge planning transitions. Journal of Professional Nursing. J Prof Nurs. 2003; 19(4):204-10.
4. Perlini NMO, Faro ACM. Cuidar da pessoa incapacitada por acidente vascular cerebral no domicílio: o fazer do cuidador familiar. Rev Esc Enferm USP. 2005; 39(2): 154-63.
5. Blumer H. Symbolic interacionism: perspective and method. Englewood Cliffs (NJ): Prentice-Hall, 1969.
6. Strauss A, Corbin J. Pesquisa qualitativa: técnicas e procedimentos para o desenvolvimento de teoria fundamentada. 2ª ed. Porto Alegre: Artmed; 2008.
7. Machado ALG, Jorge MS, Freitas CHA. A vivência do cuidador familiar de vítima de Acidente Vascular Encefálico: uma abordagem interacionista. Rev Bras Enferm. 2009; 62(2): 246-51.
8. Nardi EFR, Oliveira MLP. Significado de cuidar de idosos dependentes na perspectiva do cuidador familiar. Cienc Cuid Saúde. 2009; 8(3):428-35.
9. Vedootto DO, Silva RM. Humanization with the family in an Intensive Care Unit: a descriptive study. Online Braz J of Nurs [ serial on the Internet ]. 2010 [ cited 2011 Set 11 ]9(3). Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/j.1676-285.2010.3135/html
10. Valadares GV, Paiva RS. Estudos sobre o cuidado à família do cliente hospitalizado: contribuições para enfermagem. Rev Rene. 2010; 11(3): 180-8.
Authors:
Raquel Silva de Paiva: Researcher/Field Researcher, Glaucia Valente Valadares: Orientation of the Research and the Manuscript, Juliana Pontes da Silva: Co-orientation of the Manuscript.
Received: 07/10/2011
Approved: 05/07/2012