REVIEW AND COMMENT
Home visits in cases of heart failure: reflection in the light of Leininger’s theory
Karen Brasil Ruschel1, Karina Azzolin1, Eneida Rejane Rabelo1
1Federal University of Rio Grande do Sul
INTRODUCTION
In view of the somber epidemiological panorama of heart failure (HF), especially in terms of high hospital readmission rates, new patient care strategies need to be tested and implemented by nurses(1-3).
HF is a worrying and problematic disorder for health teams, the most important objective in treatment being to attain and maintain the clinical stability of the patient(4-6). Educating patients in their homes can be an alternative that brings the healthcare team closer to the patients’ reality, sometimes supporting the continuity of the educational process initiated during hospital confinement, or even the strategies planned on an outpatient clinic level(7).Home visits are gaining in importance, because guiding patients and caregivers in their routine environment and identifying difficulties in their ability to implement self-care, makes this approach more effective and humanized. Home nursing is characterized by the care, treatment, recovery and rehabilitation of patients, taking into consideration the family and community organization of which the patient is part(8).
Home caring of HF patients by nurses includes providing guidance about the disease and self-care, about dietary restrictions regarding salt and liquids, monitoring adherence to prescribed drugs, weight control, and the early verification of signals and symptoms of decompensation(9-10). Studies have demonstrated that failure by patients to recognize the signals and symptoms of HF as well as a low adherence to treatment, are precipitating factors that may be involved in decompensation(11).
In home care, the emphasis of attention shifts from the focus on the recovery of the individual’s health, to the focus on the prevention of risks and injuries, and to promoting health. Preference for home care over hospitalization is a global trend, a strategy that could ensure humanized assistance, apart from reducing hospital costs arising from the hospitalization process(12).
However, the success of this approach requires continuing and frequent efforts with the objective of bringing the healthcare team closer to the patient and their caregivers. In practice, we are faced with different ways of life, cultural heritages, and especially, visions of the disease process peculiar to each individual. Such aspects mean that the health professional has a need to understand and have knowledge of various cultural dimensions. It is necessary to transform the care prescribed at, and attached to, hospital environments into culturally congruent care envisioning that the quantity and quality of the information and guidance dispensed by the nurse is, in fact, implemented in the family and in the social context of each patient(13-14).
According to this perspective, we can seek support from Leininger’s cultural care diversity and universality theory on which to base the practice of home nursing care for HF patients, transforming fiction into reality.
OBJECTIVE
To exercise the theoretical-reflexive thinking based on Leininger’s cultural care diversity and universality theory in the context of home visits for HF patients.
THEORETICAL FRAMEWORK- LEININGER’S CULTURAL CARE DIVERSITY AND UNIVERSALITY THEORY
While working on her doctoral thesis at the end of the 1950s, Madeleine Leininger described transcultural nursing as being a specific area of nursing practice. The transcultural health model was presented in the 1970s, but it was only in 1984 that the globally disseminated Sunrise model was published(15). In Brazil, Leininger’s theory became a reference which was used with increasing frequency by the end of the 1980s. Its objective is to provide culturally congruent nursing care for individuals of various cultures. For Leininger, cultural care is concerned with the values, beliefs and expressions that help, support or qualify the individual or group to maintain their well-being and to improve their quality of life(16).
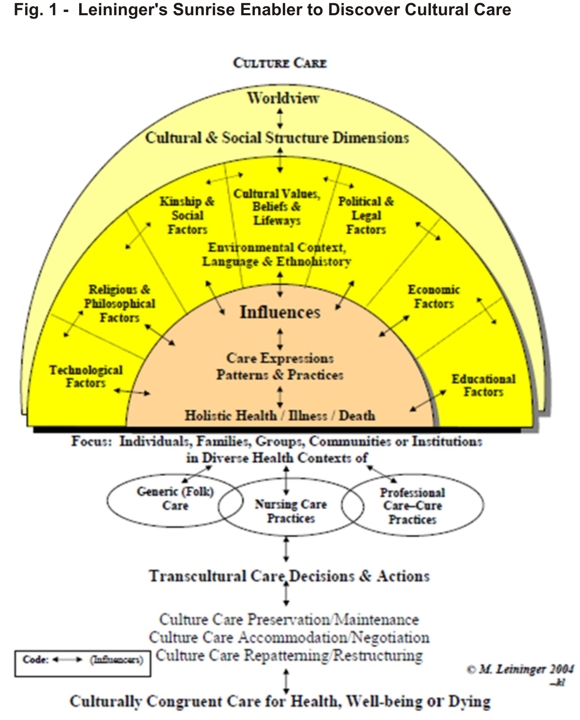
The focus is on recognizing and understanding cultural similarities and differences as part of the process of constructing nursing care. The Sunrise model (Fig. 1- Leininger’s Sunrise Enabler to Discover Cultural Care) was developed by Leininger in order to arrange the essential components of her theory into a scheme. The rising sun symbolizes care (the appearing of the sun), which is concerned with phenomena related to assistance, the conduct of support and capacity building directed at the individual, with a real or potential need to attenuate or improve their quality of live(15).The upper half of the circle represents the components of the social structure and factors related to a vision of the world that influences care giving and health through language and encounter. Such factors influence the popular system, the professional system and the nurse, represented by the lower half of the circle. Both halves together represent the entire sun, that is, the scenario that nurses must consider in order to provide care and improve health. The nurse works as a link between the professional and the popular health system by means of three types of caring actions: preservation, accommodation and the re-patterning of cultural care(15).The model considers human beings as inseparable from their culture and social structure. These aspects are considered to be pillars of Leininger’s theory.
In this study, the model’s first level will be used for reflection, taking into consideration the concrete individual in the home visit scenario(15-17).
INTERRELATION ANALYSIS
In the context of HVs, practice offers evidence that the health-disease process. is impacted on by social, economic and cultural influences, making it necessary to know the cultural context of both the patient and his/her family, so that health actions lead to the expected result. The behavior and habits of individuals may be part of their culture, and have a direct influence in health and nursing practices. According to Leininger, culture refers to the values, beliefs, rules and ways of life perceived, accepted and transmitted by a certain group within society, and it guides their thoughts, decisions, actions and standards of care(16-17).These aspects are focused on using Leininger’s Theory, which proposes provding care in a transcultural and holistic light.
During the HV, the nurse must take into consideration the individuals, families or groups actively involved in the process of caring, avoiding culturally imposing health practices that are still very deeply-rooted in the biomedical model(17). Imposing practices do not favor autonomy and decision-making, therefore precluding a change of habit and behavior, which are the main objectives of home caring(18). Culture is still recognized as a barrier to adhering to treatment(19). Therefore, culturally congruent care is the opposite of an imposing practice, in which the individual is a participatory being, the subject of care with their own concepts of health and of disease(17). HF is a condition that considerably compromises the daily life of individuals and their families. Even when a patient is stable, physical limitations may be present, requiring that they understand and adapt to this reality. Some patients can no longer perform simple activities unless they are aided, such as bathing without help, shaving or washing the dishes, simply due to tiredness. Adaptations to dietary restrictions (little salt and reduced liquids) are also needed, which brings drastic changes into the family core(7-20). If care is to be considered satisfactory in this scenario, the nurse must consider individuals and their families as participants in the planning of care actions, so that their performance will be directed to preserving, accommodating and re-patterning care. Preservation takes place when the nurse takes into account the care provided by patients and their families on their own way and according to their beliefs and values, while upholding them, taking professional practice into consideration; accommodation refers to the nurse’s ability to negotiate in this home scenario, understanding the cultural dimension within which the individual operates, not only in their home, but in the local community. It is important to guide these patients to take daily walks in order to stimulate physical activity, but what if the individual resides in a risky area or has difficulty accessing it? The potential for negotiation proposed by Leininger can be employed as long as we know and understand this reality. It is possible to propose walks within the house itself, to talk to a family member who can and will take the patient for a walk somewhere else. After all, it is fundamental to negotiate with others and not to be imposing. Finally, remodeling means to restructure cultural care, in the sense that the nurse helps individuals and their families to change health patterns that are important for the improvement in their health, especially for their quality of life, an aspect that is intimately affected when it comes to heart failure patients(21). Home visits allow professionals to create an emotional and friendly relationship with individuals and their families, because the nurse is entering the patient’s home and is therefore getting acquainted with their private home setting. However, confidence must be established between the professional and the family so that the family can feel secure about the actions performed by the nurse. The more effective the professional’s relationship and involvement with the family, the closer will be the link between the professional system and the popular system(21).
CONCLUSION
Understanding health and the promotion of health has made professionals reconsider the concepts and theories guiding their practice so that the care they provide is closer to the needs of the users and to the meaning ascribed by users to the health process associated with their disease.
HVs in a HF scenario enable the nurse to have a wider view of the individual’s real living conditions and that of their family. Based on this view, the nurse can facilitate the family’s adaptation and planning according to their own resources in view of the disease situation. They can also provide greater freedom for the development of self-care, since the time dedicated to the patient and to his or her family is longer than in an institutional context. Leininger’s cultural diversity and universality theory is a comprehensive theory that subsidizes the exercise of critical, reflexive care, contributing to bringing the individual’s universe closer to the professional universe. Nursing care based on Leininger’s theory aims at planning actions with individuals in a participative manner, enabling them to chose the therapeutic itinerary that best suits their reality(21. During HVs, the dialogue and reflection introduced by the nurse allow individuals, their caregivers or their families to equip themselves to offer conditions to think, reflect critically and act, in an attempt to persuade them to participate in providing care.
The application of Leininger’s Theory gives nurses the opportunity to discover care practices that are specific to each individual and to the cultural factors that can influence human care, such as religion, environment, political and economic aspects, vision of the world, and others(22). However, the professional must reflect on the cultural context, and this demands knowledge and an ability to understand and value the preservation, accommodation and re-patterning of care. The relationship involving the nurse, the individual and his or her family in the household context is a fertile ground for the development of transforming educational actions, because care is a major foundation of nursing(23). After this reflection, we can affirm that cultural care theory can be used in the everyday lives of home visits for patients with heart failure, subsidizing nursing care, enabling the implementation of therapeutic interventions centered on the individual, and favoring the improvement of nurse-individual-family interpersonal relations. Therefore, it is up to nurses to assist the individual patient as a unique being, promoting their self-care, the improvement of their quality of life, the recovery of their health, and the integration of their family in terms of cultural care, which is what turns this theoretical practice into reality.
REFERENCES
1. While A, Kiek F. Chronic heart failure: promoting quality of life. Br J Community Nurs. 2009; 14(2):54-9
2. Barretto ACP, Del Carlo CH, Cardoso JN, Morgado PC, Munhoz RT, Eid MO, et al. Re-hospitalizações e morte por insuficiência cardíaca - índices ainda alarmantes. Arq Bras de Cardiol. 2008; 91(5):335-41.
3. Rohde LE, Claussell N, Ribeiro JP, Goldraich L, Netto R, William Dec G, et al. Health outcomes in descompensated congestive heart failure: a comparison of tertiary hospitals in Brazil and United States. Int J Cardiol. 2005; 102(1):71-7.
4. Göhler A, Conrads-Frank A, Worrell SS, Geisler BP, Halpern EF, Dietz R, et al. Decision-analytic evaluation of the clinical effectiveness and cost-effectiveness of management programmes in chronic heart failure. Eur J Heart Fail. 2008; 10(10):1026–32.
5. Patel H, Ekman SMI, Höjgård S, Swedberg K, Schaufelberger M.Home care as an option in worsening chronic heart failure- a pilot study to evaluate feasibility, quality adjusted life years and cost-effectiveness. Eur J Heart Fail. 2008; 10(7):675–81.
6. Bocchi EA, Cruz F, Guimarães G, Moreira LFP, Issa VS, Ferreira SMA, et al. A long-term prospective randomized controlled study using repetitive education at six-month intervals and monitoring for adherence in heart failure outpatients: the REMADHE study. Circulation. 2008; 1(2):115-24.
7. Rabelo ER, Aliti G, Domingues FB, Clausell N. Cenários de educação para o manejo de pacientes com insuficiência cardíaca. Rev Latino-Am Enferm. 2007; 15 (2): 344-9.
8. Paz AA, Santos BRL. Programas de cuidado de enfermagem domiciliar. Rev Bras Enferm. 2003; 56(5):538-41.
9. Ho YL, Hsu TP, Chen CP, Lee CY, Lin IH, Hsu RB, et al. Improved cost-effectiveness for management of chronic heart failure by combined home-based intervention with clinical nursing specialists. J Formos Med Assoc. 2007;106(4):313–9.
10. Davidson P, Paull G, Rees D, Daly J, Cockburn J. Activities of home-based heart failure nurse specialists: a modified narrative analysis. Am J Crit Care. 2005; 14(5):426-33.
11. Mangini S, Silveira FS, Silva CP, Grativvol OS, Seguro LF, Ferreira SMA, et al. Insuficiência cardíaca descompensada na unidade de emergência de hospital especializado em cardiologia. Arq Bras de Cardiol. 2008; 90(6):433-40.
12. Rabelo ER, Aliti GB, Domingues FB, Braum S. Fatores precipitantes de descompensação da insuficiência cardíaca: estudo multicêntrico EMBRACE. Arq Bras de Cardiol. 2008;91(1):224.
13. Chaves M. O cuidado domiciliar no programa de atenção ao paciente crônico grave no hospital IPSEMG [ Dissertação ]. Belo Horizonte: Universidade Federal de Minas gerais; 2004.
14. Artinian NT, Magnan M, Sloan M, Lange PM. Self-care behaviours among patients with heart failure. Heart Lung. 2002; 31(3):161-72.
15. McEwen M, Wills EM. Bases teóricas para enfermagem. 2ª ed. Porto Alegre: Artmed; 2009.
16. Marriner-Tomey A. Modelos y teorias em enfermeria. 3ª ed. Madri: Mosby; 1995.
17. Monticelli M, Boehs AE, Guesser JC, Gehrmann T, Paiva K. Perfil de dissertações que utilizam a teoria de leininger vinculadas a um programa de mestrado em enfermagem do sul do país. Ciênc cuid saúde. 2008; 7(4):447-53.
18. Oliveira DL. A ‘nova’ saúde pública e a promoção da saúde via educação: entre a tradição e a inovação. Rev Latino-Am Enferm. 2005; 13(3):423-31.
19. Hsu YH, Mao CL, Wey M. Antihypertensive medication adherence among elderly Chinese Americans. J Transcult Nurs. 2010; 21(4):297-305.
20. Barretto ACP, Drumond NC, Mady C, Albuquerque DC., Brindeiro DF, Braile DM, et al. Revisão das II diretrizes da Sociedade Brasileira de Cardiologia para o diagnóstico e tratamento da insuficiência cardíaca. Arq Bras de Cardiol. 2002; 79(4):1-30.
21. Michel T, Seima MD, Lacerda MA, Bernardino E, Lenardt MH. As práticas educativas em enfermagem fundamentadas na teoria de Leininger. Cogitare enferm. 2010; 15(1): 131-7.
22. Fernandes MTO, Soares SM. Work with groups in Family Health: concepts, structure and strategies for transcultural care. A qualitative study. Online Braz J Nurs [ serial in the internet ]. 2007 [ cited 2011 ago 13 ] 6(3). Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/j.16764285.2007.1204/247
23. Tulio EC, Stefanelli MC, Centa ML. Vivenciando a visita domiciliar apesar de tudo. Fam Saúde Desenv. 2000; 2(2):71-9.
Received: 30/09/2011
Approved: 03/09/2012